Professional Documents
Culture Documents
Balanced Crystalloids Versus Saline For Critically Ill Patients (BEST-Living)
Balanced Crystalloids Versus Saline For Critically Ill Patients (BEST-Living)
Uploaded by
vali.levo7Original Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Balanced Crystalloids Versus Saline For Critically Ill Patients (BEST-Living)
Balanced Crystalloids Versus Saline For Critically Ill Patients (BEST-Living)
Uploaded by
vali.levo7Copyright:
Available Formats
Articles
Balanced crystalloids versus saline for critically ill patients
(BEST-Living): a systematic review and individual patient
data meta-analysis
Fernando G Zampieri, Alexandre B Cavalcanti, Gian Luca Di Tanna, Lucas P Damiani, Naomi E Hammond, Flavia R Machado, Sharon Micallef,
John Myburgh, Mahesh Ramanan, Balasubramanian Venkatesh, Todd W Rice, Matthew W Semler, Paul J Young, Simon Finfer
Summary
Background The effect of balanced crystalloids compared with that of saline in critically ill patients overall and in Lancet Respir Med 2024;
specific subgroups is unclear. We aimed to assess whether use of balanced solutions, compared with 12: 237–46
0·9% sodium chloride (saline), decreased in-hospital mortality in adult patients in intensive care units (ICUs). Published Online
November 30, 2023
https://doi.org/10.1016/
Methods For this systematic review and individual patient data meta-analysis, we searched PubMed, Embase, and S2213-2600(23)00417-4
CENTRAL databases from inception until March 1, 2022 (updated Sept 1, 2023) for individually randomised and See Comment pages 187 and 188
cluster-randomised trials comparing balanced solutions with saline for adult patients in the ICU. Eligible trials were HCor Research Institute, São
those that allocated patients to receive balanced solutions or saline for fluid resuscitation and maintenance fluids, or Paulo, Brazil (F G Zampieri PhD,
for maintenance fluids only; and administered the allocated fluid throughout ICU admission or, for trials using A B Cavalcanti PhD,
landmark mortality as their primary outcome, until the timepoint at which mortality was assessed (if ≥28 days). L P Damiani MSc); Brazilian
Research in Intensive Care
Authors of eligible trials were contacted to request individual patient data. Data obtained from eligible trials were Network—BRICNet, São Paulo,
merged, checked for accuracy, and centrally analysed by use of Bayesian regression models. The primary outcome Brazil (F G Zampieri,
was in-hospital mortality. Prespecified subgroups included patients with traumatic brain injury. This study was A B Cavalcanti,
F R Machado PhD); Department
registered with PROSPERO (CRD42022299282).
of Critical Care Medicine,
Faculty of Medicine and
Findings Our search identified 5219 records, yielding six eligible randomised controlled trials. Data obtained for Dentistry, University of
34 685 participants from the six trials, 17 407 assigned to receive balanced crystalloids and 17 278 to receive saline, Alberta, Edmonton, AB,
Canada (F G Zampieri); The
were included in the analysis. The mean age of participants was 58·8 years (SD 17·5). Of 34 653 participants with
George Institute for Global
available data, 14 579 (42·1%) were female and 20 074 (57·9%) were male. Among patients who provided consent to Health, Sydney, NSW, Australia
report in-hospital mortality, 2907 (16·8%) of 17 313 assigned balanced solutions and 2975 (17·3%) of 17 166 assigned (Prof G L Di Tanna, PhD,
saline died in hospital (odds ratio [OR] 0·962 [95% CrI 0·909 to 1·019], absolute difference –0·4 percentage N E Hammond PhD,
S Micallef BN,
points [–1·5 to 0·2]). The posterior probability that balanced solutions reduced mortality was 0·895. In patients with
Prof J Myburgh MD,
traumatic brain injury, 191 (19·1%) of 999 assigned balanced and 141 (14·7%) of 962 assigned saline died (OR 1·424 M Ramanan MMed,
[1·100 to 1·818], absolute difference 3·2 percentage points [0·7 to 8·7]). The probability that balanced solutions Prof B Venkatesh MD,
increased mortality in patients with traumatic brain injury was 0·975. In an independent risk of bias assessment, Prof S Finfer MD); University of
New South Wales, Sydney,
two trials were deemed to be at low risk of bias and four at high risk of bias.
NSW, Australia
(Prof G L Di Tanna,
Interpretation The probability that using balanced solutions in the ICU reduces in-hospital mortality is high, although N E Hammond, Prof J Myburgh,
the certainty of the evidence was moderate and the absolute risk reduction was small. In patients with traumatic brain Prof B Venkatesh, Prof S Finfer);
Department of Business
injury, using balanced solutions was associated with increased in-hospital mortality. Economics, Health and Social
Care, University of Applied
Funding HCor (Brazil) and The George Institute for Global Health (Australia). Sciences and Arts of Southern
Switzerland, Lugano,
Switzerland (Prof G L Di Tanna);
Copyright © 2023 Elsevier Ltd. All rights reserved. Malcolm Fisher Department of
Intensive Care Medicine, Royal
Introduction crystalloids are constituted with use of alternative anions North Shore Hospital, Sydney,
During an admission to the intensive care unit (ICU), to reduce the chloride concentration in the fluid, and NSW Australia (N E Hammond);
Anesthaesiology, Pain and
most patients receive intravenous fluid therapy as include compound sodium lactate (Ringer’s lactate, Intensive Care Department,
supportive therapy for the presenting critical illness.1 Hartmann’s solution) or acetate-containing solutions Hospital São Paulo, Federal
Crystalloid solutions are the fluids used most commonly (Plasma-Lyte 148, Ringer’s acetate). Potential benefits of University of São Paulo,
to correct symptomatic hypovolaemia due to fluid losses, balanced crystalloid solutions include the reduction of São Paulo, Brazil (F R Machado);
St George Hospital, Sydney,
improve haemodynamic function to optimise vital organ development of an iatrogenic hyperchloraemic metabolic NSW, Australia
function and as an intravenous vehicle to administer acidosis.2 (Prof J Myburgh); Intensive Care
medications.2 Widely used intravenous crystalloid Randomised clinical trials have compared the effects of Unit, Caboolture and The
solutions include 0·9% sodium chloride (saline) and balanced solutions with those of saline on patient-centred Prince Charles Hospitals, Metro
North Hospital and Health
solutions characterised by an electrolyte profile similar outcomes in critically ill patients.3−8 One study reported Services, Brisbane, QLD,
to extracellular fluid. These buffered, or balanced, that the use of balanced solutions was associated with a Australia (M Ramanan); School
www.thelancet.com/respiratory Vol 12 March 2024 237
Articles
of Medicine, University of
Queensland, Brisbane, QLD, Research in context
Australia (M Ramanan);
Intensive Care Unit, Wesley and Evidence before this study nuanced interpretation of its findings. The probability that
Princess Alexandra Hospitals, Randomised clinical trials have compared the effects of balanced crystalloid solutions were associated with reduced in-
Woolloongabba, QLD, Australia balanced crystalloid solutions and 0·9% sodium chloride hospital mortality overall was 0·895. The probability that
(Prof B Venkatesh); Division of
Allergy, Pulmonary, and Critical
(saline) in patients treated in intensive care units (ICUs). One balanced solutions were associated with lower mortality
Care Medicine, Vanderbilt cluster-randomised trial reported that the use of balanced exceeded 0·90 in patients without traumatic brain injury
University Medical Center, solutions was associated with a reduction in the composite (>0·97), patients who did not receive 0·9% saline before
Nashville, TN, USA outcome of death, new renal replacement therapy, or persistent enrolment (>0·98), and female patients (0·95). The probability
(Prof T W Rice MD,
M W Semler MD); Department
kidney dysfunction. No individual trial reported a statistically that balanced solutions were associated with higher mortality
of Intensive Care, Wellington significant effect on mortality. A Bayesian trial-level in patients with traumatic brain injury was 0·975. The effect of
Regional Hospital, Wellington, meta-analysis of randomised trials reported a probability of balanced solutions versus saline on mortality was similar in
New Zealand (P J Young PhD); 0·895 that, compared with saline, use of balanced solutions in a subgroups defined by serum sodium and chloride
Medical Research Institute of
New Zealand, Wellington, New
heterogeneous population of ICU patients was associated with concentration and blood pH. We assessed the certainty of the
Zealand (P J Young); Australian reduced mortality. However, existing data suggest that the evidence in relation to mortality as moderate. These results
and New Zealand Intensive treatment effect might be heterogeneous, with differing effects support those of previous trial-level meta-analyses that there is
Care Research Centre, Monash
in different subgroups of patients. An individual patient data a high probability that balanced solutions are associated
University, Melbourne, VIC,
Australia (P J Young); meta-analysis not only provides an overall estimate of the reduced mortality overall, the exception being patients with
Department of Critical Care, treatment effect, but allows patients to be categorised into traumatic brain injury in whom mortality is increased. The
University of Melbourne, subgroups of interest to clinicians on the basis of pre- results add important information about effects in subgroups
Melbourne, VIC, Australia
randomisation characteristics that were not examined or of patients defined by diagnosis, demographics, and
(P J Young); School of Public
Health, Imperial College reported in publications from the original individual trials or biochemical parameters.
London, London, UK trial-level meta-analyses.
(Prof S Finfer)
Implications of all the available evidence
Added value of this study The totality of existing evidence supports the use of balanced
Correspondence to:
Prof Simon Finfer, The George This systematic review and individual patient data meta- crystalloid solutions in patients in ICUs, except for those with
Institute for Global Health, analysis included six randomised trials with 34 685 patients traumatic brain injury, in whom saline should be preferred.
Sydney, NSW 2042, Australia analysed within a Bayesian framework to provide a more
sfinfer@georgeinstitute.org.
au
reduction in a composite outcome measure of death, Given the results of a recent aggregated meta-analysis,
new renal replacement therapy, or persistent kidney which were close to traditional statistical significance,
dysfunction.4 No trial reported a statistically significant we chose to use a Bayesian framework to provide a more
difference in mortality. A recent trial-level meta-analysis comprehensive analysis of the effect of balanced
of randomised clinical trials reported a 0·895 probability solutions. Bayesian analyses provide an assessment of
that the use of balanced solutions was associated with the probability of benefit for situations in which benefit
lower mortality than saline.9 is considered probable, but the results are not
To address the remaining uncertainty over the use of statistically significant on the basis of traditional
balanced solutions in the ICU, we did an individual frequentist null hypothesis testing.12 They also provide a
patient-data meta-analysis of randomised clinical trials more nuanced approach to the effect sizes that are
analysed within a Bayesian framework to provide compatible with data (and prior information, if
estimates of the probability of benefits associated with available). Reviews of Bayesian methods in critical care
use of balanced solutions compared with saline in can be found elsewhere.13,14
a heterogeneous population of adult patients and in In relation to the use of individual patient data in meta-
prespecified subgroups. Bayesian methods were used as analyses, the Cochrane handbook states, “In most cases
they allow a more nuanced interpretation of the results, participants will not have specifically consented to
compared with traditional frequentist null hypothesis inclusion in the meta-analysis. However, as the meta-
testing that relies on a dichotomised interpretation of a analysis is posing the same research question, and is
p value to accept or reject a hypothesis. essentially updating the trial they did consent to, the
usual view is that separate consent is not required.
Methods However, it is advisable that data received are
Overview anonymised.” In keeping with this principle, our meta-
The BEST-Living Study is a living, individual patient-data analysis addressed the same question as the trials for
meta-analysis with a prespecified protocol and statistical which we have data, and all data were anonymised before
analysis plan designed to compare the effects of using transfer.
balanced solutions with those of saline in the ICU on This systematic review is reported in accordance with
patient-centred outcomes in critically ill adult patients.10,11 PRISMA-IPD guidelines.15,16
238 www.thelancet.com/respiratory Vol 12 March 2024
Articles
Search strategy and selection criteria GRADE (Grading of Recommendations Assessment,
The initial search was done on March 1, 2022, in Development and Evaluation) approach for assessing
MEDLINE, Embase, and the Cochrane Central Register certainty.17,18
of Controlled Trials (CENTRAL). Key search terms were
balanced crystalloids[Title] OR (balanced solution[Title] Outcomes
OR (balanced multielectrolyte solution[Title] OR The primary outcome was all-cause in-hospital mortality
plasmalyte[Title] OR plasma-lyte[Title] OR “plasma lyte censored at 90 days. Secondary outcomes were survival
148”[Title] OR “lactated ringer”[Title] OR “ringer at last follow-up, treatment with renal replacement
lactate”[Title] OR “normal saline”[Title]”. Full search therapy commenced during the index ICU admission,
details are provided in the appendix (p 3) and in the and days alive and out of hospital and out of ICU within See Online for appendix
statistical analysis plan.11 The eligibility of identified 28 days.
studies was assessed independently by two reviewers Prespecified subgroup analyses were done for the
(FGZ and LPD), with disagreement resolved by a third primary outcome and for treatment with renal
reviewer (ABC). replacement therapy in subgroups of patients identified
Eligible randomised clinical trials were those that by baseline characteristics of sex (male or female),
enrolled adults treated in an ICU; allocated individuals presence or absence of sepsis (as defined by each trial),
or clusters to receive balanced solutions or saline for presence or absence of traumatic brain injury, baseline
fluid resuscitation and maintenance fluids, or for serum chloride concentration (categorised as low
maintenance fluids only; and administered the allocated [<100 mmol/L], normal [100–110 mmol/L], or high
study fluid for the duration of the ICU admission or, for [>110 mmol/L]), acid-base status as defined by baseline
trials using landmark mortality as their primary pH (severe acidaemia [pH <7·20], mild acidaemia
outcome, until the timepoint at which mortality was [pH 7·20 to <7·35], normal [pH 7·35 to 7·45], or
assessed, provided mortality was assessed at 28 days or alkalaemia [pH >7·45]), volumes of intravenous saline
later. A priori, we defined balanced solutions as any received before randomisation (none, 1–999 mL, or
intravenous crystalloid solution in which the difference ≥1000 mL of saline received), and study design (cluster
between the sodium and chloride concentrations was at versus individual randomisation). Hypotheses for each
least 15 mmol/L. prespecified subgroup are presented in the appendix
We excluded trials that mandated the use of study (p 7) and in the statistical analysis plan.11 One planned
fluids for only part of participants’ ICU stays (other than subgroup analysis estimating effects in patients with
trials assessing landmark mortality beyond day 28 that non-traumatic acute brain injury was planned but could
did not mandate use of study fluids after that timepoint); not be done due to an absence of prospective
that enrolled only surgical patients; in which study fluids classification of patients in the included trials (appendix
were used for resuscitation only; that did not report in- p 8).
hospital mortality or mortality at a landmark timepoint A post-hoc analysis based on serum sodium con
of at least 28 days; and that had loss to follow-up for in- centration at baseline (<135, 135–145, or >145 mmol/L)
hospital mortality of more than 10%. was also added during the review process.
Data collection and data items Statistical analysis
The review was sponsored by the HCor Research The statistical analysis plan was finalised before data
Institute (São Paulo, Brazil) with formalised collaborative were merged or analysed.11 The primary analysis was
research agreements between the sponsor and respective based on a one-step meta-analysis using a Bayesian
author investigators and their associated institutions. hierarchical model with the intervention of interest
A data skeleton (appendix p 4) was sent to corresponding (balanced solution vs saline) as a fixed-effect covariate
authors for populating respective trial information, and two layers: the ICU (or cluster) nested within trial
which was housed on a secure server at the HCor as hierarchical effects.
Research Institute. Complete cases were included in the The primary model used for this and future iterations
analysis, with no imputation for missing data. Data is a non-informative prior for the effect size of the
quality was assured by replicating the primary analysis intervention (prior for the log odds ratio [OR] of the
of each trial, the results of which were compared with intervention defined as normal with mean 0 and
the published results of each trial; trialists were informed SD 0·355).19 Alternative analyses for the primary
about any discrepancies and allowed to respond or endpoint included an adjusted model (adjusted for age,
update their uploaded results. sex, surgical vs non-surgical admission, and sepsis),
different prior analyses (including optimistic and
Risk of bias assessment and certainty of evidence pessimistic priors), and a frequentist mixed model.
Risk of bias in the included studies and certainty of the Survival analyses were done with time-to-event models
review evidence was assessed by independent experts following a Bayesian semiparametric survival time with
using the Cochrane Risk of bias and tool and the a non-informative prior for the intervention
www.thelancet.com/respiratory Vol 12 March 2024 239
Articles
mean of 0 and SD of 4. The proportion of patients probability of the intervention (use of balanced
treated with new renal replacement therapy initiated solutions) being associated with an OR less than 1·0.
during the index ICU admission was assessed using the We also present relative risks and absolute risk
same model as the primary outcome. Length of hospital differences obtained from posterior expected
stay was analysed with a cumulative logistic model for probabilities. As described in the statistical analysis
days alive and free of hospital or ICU admission (both plan, a region of practical equivalence (ROPE) for the
truncated at 28 days, with patients who died given a effect of the intervention on the primary outcome as an
score of –1 using non-informative priors). Exploratory OR was defined as 0·955–1·046,11 shown as the
analyses were assessed with frequentist generalised percentage of the posterior probability distribution
mixed models with interaction between time and contained in the ROPE. For further details see appendix
intervention and with patients as a random intercept. (p 6).
We did a two-stage individual patient data meta- Results for the survival outcome are presented as
analysis for the primary outcome: effect sizes obtained hazard ratio (HR) and corresponding 95% CrI. Results
from each trial were aggregated using a Bayesian meta- for secondary binary outcomes are presented similarly
analysis. In addition, we did a Bayesian meta-analysis of to the primary endpoint, with exception of ROPE, which
aggregated trial-level data for hospital mortality and use was not defined for all secondary endpoints. Results for
of renal replacement therapy. subgroup analyses are presented as forest plots for the
Results for the primary outcome are presented as OR, probability of benefit, and probability of direction of
median OR (95% credible intervals [CrI]) and the the interaction for each subgroup; other measurements
probability of direction, defined as the posterior of effect size including relative risk and absolute risk
reduction are also shown. A list of deviations from
original plans to performed analysis is summarised in
5920 records identified
appendix (p 8).
4797 from databases
1123 from registers All analyses were done with R version 4.2.2 with
packages brms and bayesmeta.20,21
This study was registered with PROSPERO
701 records removed before screening
267 duplicates (CRD42022299282).
434 marked as ineligible by automation
tools
Role of the funding source
The funders of the study had no role in study design,
5219 records screened data collection, data analysis, data interpretation, or
writing of the report.
5138 records excluded
Results
The initial search was concluded on March 1, 2022. Of
81 records retrieved and assessed for eligibility the 5219 records screened, 81 were assessed for eligibility,
and six met the eligibility criteria and were selected for
75 records excluded
analysis (figure 1).3–8 All investigators agreed to share
19 surgical patients only data. Characteristics of the included studies, including
12 registry of included trial the type of balanced fluid used and volumes received
12 secondary analysis of RCT
8 not an RCT after randomisation, are shown in table 1. Of the
7 fluids used for resuscitation only six included studies, four were cluster-randomised trials
6 recruiting or not yet recruiting
4 truncated fluid use
and two were individually randomised. Two studies were
3 unable to obtain status conducted in the USA, one in Australia, one in New
2 not critically ill patients Zealand, one in Australia and New Zealand combined,
1 study in children
1 use of colloids and one in Brazil. In all trials, patients received balanced
solutions or saline for resuscitation, and all received
compatible intravenous crystalloid therapy during their
6 studies included*
ICU stay.
The search was repeated on Sept 1, 2023. We identified
Figure 1: Study identification and selection
691 new records; 37 were duplicates, 634 were ineligible
Flow diagram shows identification, screening, and selection of studies from the
initial search (concluded on March 1, 2022). On repeat search (Sept 1, 2023), we on initial review, the remaining 20 were retrieved and
identified 691 new records, among which 37 were duplicates; 20 of the underwent full-text review to assess for eligibility. None
remaining 654 were retrieved and assessed for eligibility, but none met our met our study’s eligibility criteria.
study’s eligibility criteria. *Two further records were identified by citation
A total of 34 685 patients were included in the meta-
searching, of which two were retrieved and assessed for eligibility but were
excluded as fluids were used for resuscitation only. No records were found analysis: 17 407 assigned to receive balanced crystalloids
through searches of websites or organisations. and 17 278 to receive saline. The mean age was 58·8 years
240 www.thelancet.com/respiratory Vol 12 March 2024
Articles
Number of Centres; Randomisation Masking Population Primary outcome Median fluid use, mL Balanced fluid
patients intensive care
units
Balanced Saline
solution
SPLIT (2015)3 2278 4 Cluster Masked Critically ill patients Acute kidney injury* 2000 2000 Plasma-Lyte 148
SALT (2017)4 974 1 Cluster Unmasked Critically ill patients Feasibility, MAKE30† 1617 1424 Plasma-Lyte A or
lactated Ringer solution
SMART (2018)5 15 802 1; 5 Cluster Unmasked Critically ill patients MAKE30† 1000 1020 Plasma-Lyte A or
lactated Ringer solution
BaSICS (2021)6 10 520 75 Individual Masked Critically ill patients 90-day survival 2900‡ 2900‡ Plasma-Lyte 148
PLUS (2022)7 5037 53 Individual Masked Critically ill patients 90-day survival 3900 3700 Plasma-Lyte 148
SCOPE-DKA (2021)8 93 7 Cluster Unmasked Patients with diabetic Ketoacidosis 6798¶ 6574¶ Plasma-Lyte 148
ketoacidosis resolution§
The 19-patient difference between the sum of each trial and the individual participant data meta-analysis results reflects the use of a complete case analysis in this Article. 15 patients from the BaSICs trial and
191 from the PLUS trial were excluded from the primary analysis as consent to use of their data was either withheld or withdrawn. Additionally, four patients from the SCOPE-DKA trial were excluded from the
survival analysis as date of hospital discharge was unknown. *Doubling of serum creatinine concentration, or a serum creatinine concentration of ≥3·96 mg/dL with an increase of ≥0·5 mg/dL. †Composite
endpoint of mortality, doubling of serum creatinine, or treatment with renal replacement therapy during hospitalisation, truncated at 30 days. ‡Fluid used up to 3 days after enrolment. §Base excess to at least
−3 mEq/L at 48 h post-ICU admission. ¶Mean value.
Table 1: Characteristics of included trials
(SD 17·5). Among patients with available data,
Balanced n=17 407 Saline n=17 278
20 074 (57·9%) of 34 653 patients were male,
14 579 (42·1%) were female, 20 919 (60·6%) of 34 520 were Age, years 58·6 (17·5), n=17 407 58·9 (17·4), n=17 278
non-surgical admissions, and 6585 (19·1%) of 34 427 had Sex
an admission diagnosis of sepsis (table 2; appendix Male 10 043/17 383 (57·8%) 10 031/17 270 (58·1%)
pp 10–11). For analyses adjusted for age, sex, and admission Female 7340/17 383 (42·2%) 7239/17 270 (41·9%)
type (surgical vs non-surgical) and sepsis, complete case Admission type
data were available for 17 293 assigned to receive balanced Surgical 6791/17 325 (39·2%) 6810/17 195 (39·6%)
crystalloids and 17 153 assigned to receive saline. Non-surgical 10 534/17 325 (60·8%) 10 385/17 195 (60·4%)
Consent to report in-hospital mortality was obtained Days from ICU admission to study 0·38 (2·72), n=17 323 0·37 (3·57), n=17 196
for 17 313 participants assigned balanced crystalloids enrolment
and 17 166 assigned saline. Among these patients, Sepsis 3286/17 276 (19·0%) 3299/17 151 (19·2%)
2907 (16·8%) assigned balanced crystalloids and Traumatic brain injury 999/17 325 (5·8%) 962/17 195 (5·6%)
2975 (17·3%) assigned saline died in hospital (OR 0·962 Vasopressor use at enrolment 5927/16 162 (36·7%) 5965/16 076 (37·1%)
[95% CrI 0·909 to 1·019], absolute difference Inotrope use at enrolment 5236/7656 (68·4%) 5310/7723 (68·8%)
–0·4 percentage points [–1·5 to 0·2]). The posterior Mechanical ventilation at enrolment 7905/17 325 (45·6%) 7904/17 195 (46·0%)
probability that the use of balanced crystalloid solutions Fluid use before enrolment 10 801/15 599 (69·2%) 10 687/15 490 (69·0%)
decreased the risk of in-hospital death compared with Saline, mL 426·9 (951·6), n=17 214 544·7 (1026·0), n=17 096
saline use was 0·895; 58·8% of the probability mass was Balanced solution, mL 1018·8 (1555·1), n=17 214 884·0 (1500·5), n=17 096
concentrated in the defined ROPE (table 3; figure 2A). Renal replacement therapy 496/17 320 (2·9%) 529/17 192 (3·1%)
Using alternative priors, the posterior probability of Sodium, mmol/L 138·0 (5·1), n=12 657 138·1 (5·2), n=12 630
benefit for balanced solutions could be as low as 0·821 Chloride, mmol/L 104·7 (6·3), n=12 049 105·0 (6·2), n=11 967
(pessimistic prior) and as high as 0·932 (optimistic prior; Creatinine, mmol/L 0·121 (0·125), n=16 301 0·122 (0·127), n=16 231
table 3). From the frequentist model, the OR for in- pH 7·34 (0·11), n=6136 7·34 (0·10), n=6112
hospital death with balanced crystalloids compared with Base excess, mmol/L –4·7 (6·3), n=2300 –4·5 (6·0), n=2294
saline was 0·962 (95% CI 0·908 to 1·020; absolute Data are mean (SD) or n/N (%). ICU=intensive care unit.
difference –0·4 percentage points [95% CI –1·1 to 0·2];
p=0·192; table 3). Table 2: Aggregated patient characteristics according to randomisation group
The two-stage, individual patient data meta-analysis
yielded an OR for in-hospital death for balanced solutions
versus saline of 0·956 (95% CrI 0·878 to 1·040; New use of renal replacement therapy occurred in
probability of benefit of 0·870; appendix p 16). 934 (5·6%) of 16 628 participants assigned balanced
The HR for survival to longest available follow-up for solutions and 993 (5·9%) of 16 803 assigned saline
patients assigned balanced crystalloid solutions versus (OR 0·931 [95% CrI 0·849 to 1·020], absolute risk
saline was 0·964 (95% CrI 0·918 to 1·010; table 3, difference –0·4 percentage points [–1·3 to 0·1],
figure 2B). probability of benefit 0·930; table 3).
www.thelancet.com/respiratory Vol 12 March 2024 241
Articles
In the trial-level meta-analysis using non-informative
Data are n/N (%) or mean (SD), unless otherwise specified. ICU=intensive care unit. HR=hazard ratio. OR=odds ratio. RR=relative risk. ROPE=region of practical equivalence. CrI=credible interval. *Represents the proportion of the posterior probability of
benefit that is contained in a ROPE, defined as an OR between 0·955–1·046. †Represents the probability that the posterior for the OR favours the intervention (an OR <1 for all columns, except for the cumulative odds models for “free-days” outcomes
Absolute risk difference,
priors for heterogeneity and a neutral prior for the
¶Sensitivity analysis excluding SCOPE-DKA (post-hoc analysis). ||Adjusted for age, sex, sepsis, and admission type. **Values in parentheses are 95% CI; generalised mixed model with random intercept for study or site; p=0·192. ††HR (95% CrI). ‡‡In
where the OR for benefit is >1). ‡A random slope for the effect of the intervention within the site in the trial was added (post-hoc analysis). §Includes all patients, including those receiving renal replacement therapy at enrolment (post-hoc analysis).
effect of the intervention, the OR for mortality with
percentage points
–0·4 (–1·5 to 0·2)
use of balanced solutions versus saline was
–0·4 (–1·1 to 0·2)
–0·4 (–1·3 to 0·1)
–0·5 (–1·5 to 0·3)
–0·3 (–1·2 to 0·3)
–0·5 (–2·6 to 1·1)
–0·3 (–1·3 to 0·3)
–0·5 (–1·5 to 0·1)
0·94 (95% CrI 0·86–1·03; probability of benefit of 0·92).
(95% CrI)
The corresponding OR for renal replacement therapy
was 0·94 (0·82 to 1·09; probability of benefit of 0·82;
··
··
··
··
appendix pp 17–18).
Subgroup results for in-hospital mortality are shown in
0·978 (0·930 to 1·026)
0·968 (0·921 to 1·016)
0·936 (0·857 to 1·020)
0·963 (0·914 to 1·012)
0·972 (0·920 to 1·025)
0·967 (0·917 to 1·016)
0·970 (0·924 to 1·017)
0·961 (0·821 to 1·072)
figure 3 and in the appendix (p 12), and those for use of
renal replacement therapy are shown in the appendix
RR (95% CrI)
(pp 13, 15). Denominators are reported for each subgroup
as the baseline data needed to classify participants into
subgroups was not available for all participants. The
··
··
··
··
probability that balanced solutions were associated with
lower mortality exceeded 0·90 in the following
Probability
of benefit†
subgroups: patients without traumatic brain injury
0·689
0·895
0·854
0·483
0·903
0·930
0·814
0·932
0·821
(0·975), patients who did not receive 0·9% saline before
··
··
··
enrolment (0·988), and female patients (0·950). In
patients with traumatic brain injury, 191 (19·1%) of 999
ROPE %*
assigned balanced solutions died and 141 (14·7%) of 962
50·6%
58·8%
74·8%
66·0%
44·5%
60·3%
··
··
··
··
··
assigned saline died (OR 1·424 [95% CrI 1·100–1·818],
··
absolute difference 3·2 percentage points [0·7–8·7]). the
probability that balanced solutions increased mortality in
0·964 (0·918 to 1·010)††
0·967 (0·909 to 1·029)
0·962 (0·908 to 1·020)
0·962 (0·909 to 1·019)
0·999 (0·962 to 1·037)
0·954 (0·802 to 1·087)
0·963 (0·909 to 1·021)
0·931 (0·849 to 1·020)
0·956 (0·903 to 1·010)
0·973 (0·920 to 1·030)
1·010 (0·973 to 1·050)
patients with traumatic brain injury was 0·975.
Comparing patients with and without traumatic brain
injury, the interaction probability of direction was greater
OR (95% CrI)
than 0·99; for all other comparisons between subgroups,
including those based on baseline chloride concentration
··
and pH, the interaction probability of direction was less
than 0·80. The probability that balanced solutions were
2975/17 166 (17·3%)
associated with reduced risk of new treatment with renal
993/16 803 (5·9%)
replacement therapy exceeded 0·90 in the following
Saline solution
dialysis-free patients at baseline; data missing for 79 patients. §§Ordinal Bayesian proportional OR models.
19·2 (10·3)
14·7 (10·2)
subgroups: patients with sepsis (97·5), patients without
traumatic brain injury (93·3), patients with baseline
··
··
··
··
··
··
··
··
blood pH of 7·20–7·35 (91·0), patients who did not
receive saline before enrolment (90·4), female patients
(92·0), patients enrolled in cluster-randomised trials
2907/17 313 (16·8%)
(90·7), and patients with baseline serum sodium
934/16 628 (5·6%)
Balanced solution
concentration less than 135 mmol/L (98·5).
14·8 (10·1)
19·3 (10·2)
The independent risk of bias assessment for included
trials is shown in the appendix (p 9). Two trials were
··
··
··
··
··
··
··
··
deemed to be at low risk of bias6,7 and four at high risk of
bias.3–5,8
The evidence relating to in-hospital mortality and use
Days alive and out of hospital within 28 days§§
of renal replacement therapy was assessed to be of
Main model without SCOPE-DKA study§¶
Random slope for intervention in trial‡§
moderate certainty due to risk of bias (for in-hospital
In-hospital renal replacement therapy‡‡
Days alive out of ICU within 28 days§§
mortality) or inconsistency (for use of renal replacement
therapy; appendix p 14).
Table 3: Summary of effect sizes
Discussion
Frequentist model**
In this individual patient data meta-analysis
Adjusted model||
Pessimistic prior
Optimistic prior
In-hospital death
incorporating data from randomised clinical trials, the
Main model
use of balanced solutions for intravenous fluid therapy
in adults in the ICU was associated with a high
Survival
probability of reduced in-hospital mortality overall. The
main Bayesian analysis suggests the OR for in-hospital
242 www.thelancet.com/respiratory Vol 12 March 2024
Articles
death for balanced solutions compared with saline
A
is 0·962 (ie, approximately a 4% reduction in the odds of
15
dying) with a 95% CrI of 0·909 to 1·019 (ie, around a Favours balanced solutions Favours saline
9% reduction or a 2% increase in the odds of dying,
respectively). These values are consistent with those
Posterior probability density
from the frequentist analysis (OR 0·962 10
[95% CI 0·908–1·020]). The point estimates and the CrIs
and CIs are consistent with the posterior probability
of 89·5% that the use of balanced solutions reduces
5
mortality by some amount, the converse of which is a
10·5% probability that it does not reduce mortality.
While the results of the Bayesian and frequentist
analyses are consistent, the inferences that can be drawn 0
from them might differ. A purely frequentist view would 0·84 0·88 0·92 0·96 1·00 1·04
be that there was no difference between balanced OR
solutions and saline, as the upper limit of the 95% CI
B
is 1·020. By contrast, the Bayesian analysis implies a
100 Saline solution
high probability that balanced solutions reduce mortality. Balanced solution
We defined a margin of practical equivalence, which can 36
be viewed as the range of ORs indicating that a treatment 32
Cumulative mortality (%)
should not be selected based on assessment of efficacy 28
alone, as an OR of 0·955–1·046. Thus, although our 24
analysis suggests a high probability that balanced 20
solutions reduce mortality by a small amount, other 16
factors such as acquisition cost might influence whether 12
clinicians choose to use them. When acquisition costs 8
are similar, clinicians might consider a 4% or less 4
reduction in risk of death sufficient evidence to choose 0
balanced solutions. However, the estimate for the 0 15 30 45 60 75 90
absolute reduction in mortality was 0·4 percentage Time (days)
Number at risk
points, meaning that 250 patients would have to be Saline solution 17166 7690 6393 6032 5872 5782 5717
Balanced solution 17313 7580 6357 6036 5878 5786 5726
treated with balanced solutions to prevent one death. In
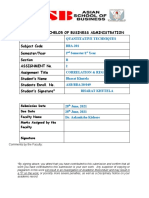
situations where balanced solutions are more expensive Figure 2: Posterior probability distribution for in-hospital mortality and cumulative mortality
and health-care resources are limited, this possible (A) Plot of the posterior probability distribution for OR for in-hospital mortality for balanced solutions versus
benefit might not be considered compelling. saline. The vertical dotted line indicates an OR of 1·00 (point of equivalence between treatments). (B) Survival
curves according to fluid type. OR=odds ratio.
The use of balanced solutions was associated with
increased in-hospital mortality in patients with traumatic
brain injury and decreased in-hospital risk of death in concentration nor blood pH at enrolment could be used
patients without traumatic brain injury. These findings to identify patients in whom saline use was associated
support the use of balanced solutions in patients without with reduced mortality. These data do not support the
traumatic brain injury. There was also a high probability hypothesis that blood pH or chloride concentration are
that balanced solutions reduced treatment with renal the mechanism by which balanced solutions and saline
replacement therapy. are associated with differences in outcomes. We found
The direction of treatment effect replicates the findings no heterogeneity of treatment effect on the basis of
of a recent trial-level systematic review and meta- baseline serum sodium concentration.
analysis,9 but the ability of our analysis to separate Balanced solutions and saline are widely used in
patients with and without traumatic brain injury provides clinical practice. This study provides clinicians with
stronger evidence for both of those populations. In information that could inform choices about which fluid
addition, a probabilistic interpretation of the effect of to use for patients treated in an ICU.22 The combined
balanced solutions on treatment with renal replacement trials provide evidence that balanced solutions should be
therapy is also provided. The use of individual patient- favoured in critically ill patients without traumatic brain
level data from randomised clinical trials allowed for injury.
estimation of treatment effects in a range of subgroups This individual patient data meta-analysis has
of potential interest to clinicians. Apart from patients limitations. First, in an independent assessment, some
with traumatic brain injury, subgroups in which saline trials included in the analysis were judged to have a
use was associated with improved outcomes were not high risk of bias, predominantly due to cluster
identified. In particular, neither blood chloride randomisation, resulting in concerns over allocation
www.thelancet.com/respiratory Vol 12 March 2024 243
Articles
In-hospital death, n/N (%) Odds ratio Probability Probability of
(95% credible of benefit* direction of
interval) interaction†
Balanced solution Saline solution
Sepsis3–8 0·60
No 1834/13 932 (13·2%) 1834/13 775 (13·3%) 0·981 (0·914–1·057) 0·682
Yes 1070/3370 (31·8%) 1136/3383 (33·6%) 0·935 (0·847–1·040) 0·893
Traumatic brain injury3–8 >0·99
No 2713/16 304 (16·6%) 2830/16 198 (17·5%) 0·942 (0·886–1·000) 0·975
Yes 191/999 (19·1%) 141/962 (14·7%) 1·424 (1·100–1·818) 0·003‡
Baseline serum chloride concentration, mmol/L5–8 0·54
<100 481/1992 (24·1%) 451/1867 (24·2%) 0·998 (0·864–1·153) 0·515
100 to 110 1060/7831 (13·5%) 1097/7724 (14·2%) 0·948 (0·865–1·043) 0·860
>110 408/2205 (18·5%) 462/2342 (19·7%) 0·917 (0·787–1·071) 0·867
pH6–8 0·66
<7·20 200/488 (41·0%) 221/494 (44·7%) 0·849 (0·642–1·119) 0·877
7·20 to <7·35 506/2424 (20·9%) 550/2527 (21·8%) 0·966 (0·837–1·121) 0·676
7·35 to 7·45 425/2457 (17·3%) 418/2368 (17·7%) 0·956 (0·821–1·119) 0·710
>7·45 216/747 (28·9%) 200/696 (28·7%) 1·014 (0·797–1·285) 0·458
Saline use before enrolment3–7 0·68
None 1865/11 903 (15·7%) 1819/10 618 (17·1%) 0·922 (0·856–0·990) 0·988
1 to 999 mL 410/1953 (21·0%) 399/2087 (19·1%) 1·097 (0·942–1·286) 0·128
≥1000 mL 621/3326 (18·7%) 747/4353 (17·2%) 0·996 (0·882–1·122) 0·521
Sex3–8 0·65
Female 1229/7305 (16·8%) 1299/7204 (18·0%) 0·928 (0·851–1·011) 0·950
Male 1673/9995 (16·7%) 1674/9956 (16·8%) 0·987 (0·914–1·068) 0·642
Study randomisation3–8 0·45
Cluster 1160/8510 (13·6%) 1172/8356 (14·0%) 0·964 (0·882–1·053) 0·786
Individual 1747/8803 (19·8%) 1803/8810 (20·5%) 0·961 (0·890–1·036) 0·841
Serum sodium concentration before enrolment, mmol/L5,6,8§ 0·51
<135 552/2407 (22·9%) 534/2307 (23·1%) 0·992 (0·871–1·133) 0·548
135 to 145 1394/9682 (14·4%) 1451/9735 (14·9%) 0·963 (0·883–1·041) 0·820
>145 230/566 (40·6%) 247/587 (42·1%) 0·953 (0·754–1·193) 0·666
0·6 0·7 0·8 0·9 1·0 1·1 1·2 1·3 1·4 1·6 1·8
Favours balanced solutions Favours saline
Figure 3: Forest plot of subgroup analysis of in-hospital mortality
Chloride and pH are the last recorded values before individual patient randomisation. The trials contributing data for each subgroup are indicated by reference numbers: SPLIT,3 SALT,4 SMART5 BaSICS,6
PLUS,7 and SCOPE-DKA.8 *Probability that balanced solution reduces the risk of in-hospital death compared with saline. †Estimate of the probability mass of the posterior for the interaction that points
towards an increase or decrease of effect. ‡The probability of harm (ie, increased mortality) was 0·975. §Post-hoc subgroup.
concealment. Second, primary outcome data were not 19 147 cluster-randomised participants included in this
available for some participants because, in critical care meta-analysis) and had multiple crossovers, and
trials of urgent interventions, institutional review therefore the highest risk of carryover effects. As a
boards and ethics committees might allow participant secondary analysis to adjust for carryover effects did not
enrolment without previous informed consent; however, affect the SMART study results, we did not repeat that
participants or their legal surrogates can subsequently analysis. Fourth, we planned to evaluate the subgroup
withhold consent to the use of their data, leading to loss of patients with non-traumatic acute brain injuries;
of outcome data. This loss resulted in 15 patients from however, extracting data on this subgroup of patients
the BaSICS trial6 and 191 patients from the PLUS trial7 was not possible due to lack of prospective
being excluded from the primary analysis, and four subclassification of patients in the included trials. Thus,
patients from the SCOPE-DKA trial8 being excluded the relative risks and benefits of balanced solutions
from the survival analysis due to missing follow-up versus saline in patients with non-traumatic acute brain
data. Third, in the cluster-randomised trials, patients injury remains unclear, and further research in such
might have received both balanced solution and saline if patients is warranted. Fifth, this study included data
present in the ICU when the units changed from using from randomised clinical trials that compared a range
one fluid to the other, and this carryover effect might of balanced solutions with saline, but did not allow for
have affected the results. SMART5 was the largest the effects of different balanced solutions to be
cluster-randomised trial (representing 15 802 of the compared.
244 www.thelancet.com/respiratory Vol 12 March 2024
Articles
Our report is the first iteration of a living review in the Australian National Health and Medical Research Council, research
which the search will be repeated each year and the funding and consulting fees from Baxter Healthcare related to
intravenous fluid therapy, research funding and consulting fees from
analysis updated when new eligible trial data become RevImmune unrelated to fluid therapy, and research funding from
available. Endpoint Health unrelated to fluid therapy, all paid to his institution;
In conclusion, overall, there is a high probability that and owning stock options in Sepsis Scout, unrelated to fluid therapy.
use of balanced solutions compared with saline in the Data sharing
ICU is associated with reduced in-hospital mortality and Requests for access to data should be directed to the investigators of the
reduced treatment with renal replacement therapy, with included trials who retain ownership of their data. The authors do not
have legal authority to share those data.
the evidence being of moderate certainty. However, in
patients with traumatic brain injury, balanced solutions Acknowledgments
The independent risk of bias assessment for this study was done by
probably increase mortality. Caroline Kamp Jørgensen and Johan Holgersson.
Contributors
References
FGZ wrote the initial draft of the systematic review protocol, and all 1 Myburgh JA, Mythen MG. Resuscitation fluids. N Engl J Med 2013;
authors revised and approved it. FGZ, GLDT, and LPD wrote the statistical 369: 1243–51.
analysis plan, and all authors revised and approved it. FGZ, LPD, and ABC 2 Semler MW, Kellum JA. Balanced crystalloid solutions.
searched and selected studies. FGZ and LPD merged databases and Am J Respir Crit Care Med 2019; 199: 952–60.
checked for accuracy. FGZ, GLDT, and LPD analysed the data. FGZ, ABC, 3 Young P, Bailey M, Beasley R, et al. Effect of a buffered crystalloid
GLDT, LPD, and SF have directly accessed the data. FGZ and SF wrote the solution vs saline on acute kidney injury among patients in the
first draft of the manuscript and all remaining authors revised it. All intensive care unit: the SPLIT randomized clinical trial. JAMA 2015;
authors commented on drafts of the manuscript, approved the final 314: 1701–10.
manuscript for submission, and were responsible for the decision to 4 Semler MW, Wanderer JP, Ehrenfeld JM, et al. Balanced crystalloids
submit the manuscript. FGZ and SF had full access to all of the data and versus saline in the intensive care unit. the SALT randomized trial.
the final responsibility to submit for publication. Am J Respir Crit Care Med 2017; 195: 1362–72.
5 Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids
Declaration of interests
versus saline in critically ill adults. N Engl J Med 2018;
FGZ reports receiving consulting fees from Baxter (USA) and 378: 829–39.
Bactiguard (Sweden), and grants, paid to his institution from Ionis
6 Zampieri FG, Machado FR, Biondi RS, et al. Effect of intravenous
Pharmaceuticals (USA), and receiving logistical support and donation fluid treatment with a balanced solution vs 0.9% saline solution on
of study materials from Baxter Hospitalar for the BaSICS trial. mortality in critically ill patients: the BaSICS randomized clinical
ABC reports receiving logistical support and donation of study materials trial. JAMA 2021; 326: 1–12.
from Baxter Hospitalar for the BaSICS trial. GLDT reports receiving 7 Finfer S, Micallef S, Hammond N, et al. Balanced multielectrolyte
consulting fees from Gilead paid to his then employer (The George solution versus saline in critically ill adults. N Engl J Med 2022;
Institute for Global Health) for work outside the scope of this paper. 386: 815–26.
LPD reports receiving fees for statistical analysis from Nestlé and 8 Ramanan M, Attokaran A, Murray L, et al. Sodium chloride or
Endpoint Health, all unrelated to the scope of this study. NEH reports Plasmalyte-148 evaluation in severe diabetic ketoacidosis
research funding and donation of study materials from Baxter (SCOPE-DKA): a cluster, crossover, randomized, controlled trial.
Healthcare related to intravenous fluid therapy, research funding from Intensive Care Med 2021; 47: 1248–57.
Endpoint Health, and consulting fees from RevImmune unrelated to 9 Hammond NE, Zampieri FG, Di Tanna GL, et al. Balanced
fluid therapy, all paid to her employer; and competitive research grants crystalloids versus saline in critically ill adults: a systematic review
from the Australian National Health and Medical Research Council and with meta-analysis. NEJM Evid 2022; 1: EVIDoa2100010.
Medical Research Future Fund. FRM reports receiving consulting fees 10 Zampieri FG, Cavalcanti AB, Di Tanna GL, et al. Protocol for
from Baxter and receiving logistical support and donation of study balanced versus saline trialists: living systematic review and
materials from Baxter Hospitalar for the BaSICS trial. SM declares no individual patient data meta-analysis of randomised controlled trials
competing interests. JM reports research funding and donation of study (BEST-Living study). Crit Care Resusc 2022; 24: 128–36.
materials from Baxter Healthcare related to intravenous fluid therapy, 11 Zampieri FG, Cavalcanti AB, Di Tanna GL, et al. Statistical analysis
paid to his employer; research funding from Endpoint Health unrelated plan for balanced versus saline trialists living systematic review
individual patient and aggregated data meta-analysis of randomized
to fluid therapy; and competitive research grants from the Australian
controlled trials (BEST-Living study). medRxiv 2022; published
National Health and Medical Research Council and Medical Research online Sept 9. https://doi.org/10.1101/2022.09.06.22279363
Future Fund. MR reports donation of study materials from Baxter (preprint).
Healthcare related to intravenous fluid therapy and competitive 12 Goligher EC, Tomlinson G, Hajage D, et al. Extracorporeal
research grants from the Australian Medical Research Future Fund. membrane oxygenation for severe acute respiratory distress
BV reports donation of study materials from Baxter Healthcare related syndrome and posterior probability of mortality benefit in a post
to intravenous fluid therapy, research funding from Endpoint Health hoc Bayesian analysis of a randomized clinical trial. JAMA 2018;
unrelated to fluid therapy, and consulting fees from RevImmune 320: 2251–59.
unrelated to fluid therapy, all paid to his institution; and competitive 13 Yarnell CJ, Abrams D, Baldwin MR, et al. Clinical trials in critical
research grants from the Australian National Health and Medical care: can a Bayesian approach enhance clinical and scientific
Research Council. TWR reports receiving consulting fees received from decision making? Lancet Respir Med 2021; 9: 207–16.
Cumberland Pharmaceuticals and Cytovale and fees for serving as a 14 Zampieri FG, Casey JD, Shankar-Hari M, Harrell FE Jr,
data safety and monitoring board member from Sanofi, all unrelated to Harhay MO. Using Bayesian methods to augment the
the scope of this paper; and grants from the US National Institutes for interpretation of critical care trials. an overview of theory and
Health, Centers for Disease Control, and Department of Defence, all example reanalysis of the alveolar recruitment for acute respiratory
paid to his institution. MWS reports receiving grants from the US distress syndrome trial. Am J Respir Crit Care Med 2021;
203: 543–52.
National Institutes for Health and Department of Defence unrelated to
the current work; and consulting fees and honoraria from Baxter 15 Stewart LA, Clarke M, Rovers M, et al. Preferred Reporting Items
for Systematic Review and Meta-Analyses of individual participant
Healthcare related to intravenous fluid therapy. PJY reports receiving
data: the PRISMA-IPD Statement. JAMA 2015; 313: 1657–65.
competitive grants from the Health Research Council of New Zealand
16 Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020
unrelated to this work; consulting fees from AM Pharma unrelated to
statement: an updated guideline for reporting systematic reviews.
this work; and consulting fees from Baxter Healthcare related to BMJ 2021; 372: n71.
intravenous fluid therapy. SF reports competitive research grants from
www.thelancet.com/respiratory Vol 12 March 2024 245
Articles
17 Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for 20 Bürkner PC. Bayesian item response modeling in R with brms and
assessing risk of bias in randomised trials. BMJ 2019; 366: l4898. stan. J Stat Softw 2021; 100: 1–54.
18 Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 21 Röver C. Bayesian random-effects meta-analysis using the
3. Rating the quality of evidence. J Clin Epidemiol 2011; 64: 401–06. bayesmeta R package. J Stat Softw 2020; 93: 1–51.
19 Zampieri FG, Casey JD, Shankar-Hari M, Harrell FE Jr, 22 Young PJ, Nickson CP, Perner A. When should clinicians act on
Harhay MO. Using Bayesian Methods to Augment the non-statistically significant results from clinical trials? JAMA 2020;
Interpretation of Critical Care Trials. An Overview of Theory and 323: 2256–57.
Example Reanalysis of the Alveolar Recruitment for Acute
Respiratory Distress Syndrome Trial. Am J Respir Crit Care Med
2021; 203: 543–52.
246 www.thelancet.com/respiratory Vol 12 March 2024
You might also like
- Pipeline Studio Gas Network Simulator PDFDocument4 pagesPipeline Studio Gas Network Simulator PDFhamza2085100% (1)
- Projects Prasanna Chandra 7E Ch4 Minicase SolutionDocument3 pagesProjects Prasanna Chandra 7E Ch4 Minicase SolutionJeetNo ratings yet
- Tugas RCT SenaDocument10 pagesTugas RCT SenaArfad El HabibieNo ratings yet
- Classifi Cation of Treatment-Related Mortality in Children WithDocument7 pagesClassifi Cation of Treatment-Related Mortality in Children WithIgnatia Rosalia KiranaNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: BackgroundDita Putri DamayantiNo ratings yet
- Mortality Risk Attributable To High and Low Ambient TemperatureDocument7 pagesMortality Risk Attributable To High and Low Ambient TemperatureRoel PlmrsNo ratings yet
- C19 Useless AntiviralDocument13 pagesC19 Useless Antiviral2jbkrf5bkcNo ratings yet
- LatitudeDocument15 pagesLatitudeJulio MineraNo ratings yet
- Statin Has Low Impact To Reduce CVD Risk 2022 - Oi - 220004 - 1650900292.38571Document8 pagesStatin Has Low Impact To Reduce CVD Risk 2022 - Oi - 220004 - 1650900292.38571Saiduzzaman TarafderNo ratings yet
- Outpatient Treatment of COVID-19 and Incidence of post-COVID-19 Condition Over 10 MonthsDocument11 pagesOutpatient Treatment of COVID-19 and Incidence of post-COVID-19 Condition Over 10 MonthsStavya DubeyNo ratings yet
- Peg Ifn MelanomaDocument10 pagesPeg Ifn Melanomaapi-26302710No ratings yet
- Balanced Multielectrolyte Solution Versus Saline in Critically Ill AdultsDocument12 pagesBalanced Multielectrolyte Solution Versus Saline in Critically Ill AdultsDe Frede EditoreNo ratings yet
- Balanceadas Vs Salinas NEJM 2022Document12 pagesBalanceadas Vs Salinas NEJM 2022Doreli RuizNo ratings yet
- Efficacy and Safety of Rezafungin and Caspofungin in Candidaemia and Invasive CandidiasisDocument10 pagesEfficacy and Safety of Rezafungin and Caspofungin in Candidaemia and Invasive Candidiasisluis sanchezNo ratings yet
- Jurnal Radiologi 1Document9 pagesJurnal Radiologi 1Papay MaulidyaNo ratings yet
- Antibiotics For Lower Respiratory Tract Infection in ChildrenDocument10 pagesAntibiotics For Lower Respiratory Tract Infection in ChildrenResidentes HIP 2022No ratings yet
- Jamainternal Byrne 2022 Oi 220004 1647010631.26452Document8 pagesJamainternal Byrne 2022 Oi 220004 1647010631.26452Irving Santiago SandovalNo ratings yet
- Friedman 2015Document7 pagesFriedman 2015yunNo ratings yet
- Blood Pressure Lowering and Risk of New Type 2 DiabetesDocument8 pagesBlood Pressure Lowering and Risk of New Type 2 DiabetesFanny Isabel Rubio CampaNo ratings yet
- PIIS2213260017304745Document10 pagesPIIS2213260017304745Juan Pablo CasanovaNo ratings yet
- Caitlin M P Jones Opioid Analgesia For Acute Low BackDocument9 pagesCaitlin M P Jones Opioid Analgesia For Acute Low BacktsyrahmaniNo ratings yet
- 2020 Terri Glioma PRODocument7 pages2020 Terri Glioma PRORimpa Basu AchariNo ratings yet
- 8 28 PDFDocument8 pages8 28 PDFfirmansyahddsNo ratings yet
- Articles: BackgroundDocument8 pagesArticles: BackgroundfirmansyahddsNo ratings yet
- PIIS2213260023004186Document11 pagesPIIS2213260023004186teresa mendozaNo ratings yet
- Krag 2010Document7 pagesKrag 2010Daniel La Concha RodriguezNo ratings yet
- Jolliffe2017 PDFDocument10 pagesJolliffe2017 PDFhadiNo ratings yet
- Meta Statin Induce DMDocument8 pagesMeta Statin Induce DMErvan ZuhriNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundTatanNo ratings yet
- Kim 2015Document9 pagesKim 2015Ke XuNo ratings yet
- Piis2666524724000016 240415 074055Document9 pagesPiis2666524724000016 240415 074055Joe Christopher Olivares LopezNo ratings yet
- Manage TrialDocument10 pagesManage Trialgareth.goldNo ratings yet
- Efek Samping Obat TBDocument12 pagesEfek Samping Obat TBLeonita L. ArdiatiNo ratings yet
- Paul 2018Document10 pagesPaul 2018Ricardo UchuyaNo ratings yet
- Pacific StrokeDocument11 pagesPacific StrokemrabhilekhNo ratings yet
- Proton FLASH Radiotherapy For The Treatment of Symptomatic Bone Metastases4Document8 pagesProton FLASH Radiotherapy For The Treatment of Symptomatic Bone Metastases4karnjNo ratings yet
- Articles: BackgroundDocument13 pagesArticles: BackgroundSilva Neta OktariNo ratings yet
- Comparison of Isotonic and Hypotonic Intravenous Maintenance Fluids A Randomized Clinical TrialDocument8 pagesComparison of Isotonic and Hypotonic Intravenous Maintenance Fluids A Randomized Clinical TrialyunNo ratings yet
- Journal Reading SarafDocument10 pagesJournal Reading SarafRifa RoazahNo ratings yet
- EsteroidesDocument10 pagesEsteroidesArturo Vargas AguilarNo ratings yet
- BMJ j3887 FullDocument10 pagesBMJ j3887 FullRiri Maisytoh PutriNo ratings yet
- Efficacy and Safety of Oral Solithromycin Versus Oral Moxiflacin (RAND)Document10 pagesEfficacy and Safety of Oral Solithromycin Versus Oral Moxiflacin (RAND)Maite De LeonNo ratings yet
- Vitamin D Supplementation To Prevent Asthma Exacerbations - A Sys9tematic Review and Meta-Analysis of Individual Participant DataDocument10 pagesVitamin D Supplementation To Prevent Asthma Exacerbations - A Sys9tematic Review and Meta-Analysis of Individual Participant Datamirr daaNo ratings yet
- TX Nmda EncefDocument9 pagesTX Nmda EncefserftyNo ratings yet
- Ahmad 2018Document14 pagesAhmad 2018Cristopher OchoaNo ratings yet
- Schöffski Et Al. - 2016 - Eribulin Versus Dacarbazine in Previously TreatedDocument9 pagesSchöffski Et Al. - 2016 - Eribulin Versus Dacarbazine in Previously TreatedM.No ratings yet
- Abstracts of The 18th Congress of The European Geriatric Medicine SocietyDocument439 pagesAbstracts of The 18th Congress of The European Geriatric Medicine SocietyCristina Fernández DíazNo ratings yet
- Jurnal Global Health Prevalens DM Pada TB AktifDocument13 pagesJurnal Global Health Prevalens DM Pada TB AktiftamiFUNo ratings yet
- Jco 22 02347Document11 pagesJco 22 02347Quang Thái NguyễnNo ratings yet
- Oral CorticoidesDocument13 pagesOral CorticoidesANDREA CABRERA de MARTINEZNo ratings yet
- Keynote 048Document14 pagesKeynote 048brenomendespNo ratings yet
- Seoane 2007Document9 pagesSeoane 2007andresfelipelamosNo ratings yet
- Adalimumab Plus Methotrexate For Uveitis in Juvenile Idiopathic ArthritisDocument17 pagesAdalimumab Plus Methotrexate For Uveitis in Juvenile Idiopathic ArthritisaisNo ratings yet
- Articles: BackgroundDocument12 pagesArticles: BackgroundCésar Aguirre RomeroNo ratings yet
- The Oswestry Risk IndexDocument7 pagesThe Oswestry Risk IndexRamon LagoNo ratings yet
- Int Endodontic J - 2022 - Weissheimer - Head and Neck Radiotherapy Effects On The Dental Pulp Vitality and Response ToDocument16 pagesInt Endodontic J - 2022 - Weissheimer - Head and Neck Radiotherapy Effects On The Dental Pulp Vitality and Response ToDhiaa AloweadatNo ratings yet
- Radiol 15131519Document11 pagesRadiol 15131519ArifHidayatNo ratings yet
- Clinical Course of Untreated Cerebral Cavernous MalformationsDocument8 pagesClinical Course of Untreated Cerebral Cavernous MalformationsMalaspulgasNo ratings yet
- Efficacy of Levetiracetam, Fosphenytoin, and Valproate For Established Status Epilepticus by Age Group (ESETT) : A Double-Blind, Responsive-Adaptive, Randomised Controlled TrialDocument8 pagesEfficacy of Levetiracetam, Fosphenytoin, and Valproate For Established Status Epilepticus by Age Group (ESETT) : A Double-Blind, Responsive-Adaptive, Randomised Controlled TrialEva FadilaNo ratings yet
- 1 s2.0 S0140673621002191 MainDocument11 pages1 s2.0 S0140673621002191 Maintravel doctorNo ratings yet
- Stroke Assessment by Telemedicine 1709687983Document7 pagesStroke Assessment by Telemedicine 1709687983Márcio Wellington de SouzaNo ratings yet
- Innovations in Modern Endocrine SurgeryFrom EverandInnovations in Modern Endocrine SurgeryMichael C. SingerNo ratings yet
- Elective Data and Analysis Prelim ExaminationDocument1 pageElective Data and Analysis Prelim ExaminationGian CarloNo ratings yet
- Statistics For Nursing Research A Workbook For Evidence Based Practice Oct 17 2019 - 0323654118 - Elsevier Susan K Grove Full Download ChapterDocument52 pagesStatistics For Nursing Research A Workbook For Evidence Based Practice Oct 17 2019 - 0323654118 - Elsevier Susan K Grove Full Download Chapterrobert.thomas145100% (7)
- M3 Part 2: Regression AnalysisDocument21 pagesM3 Part 2: Regression AnalysisGouri LakshmiNo ratings yet
- Exercise 3.3: CRD and Post Hoc Test (Practice Exercises 1 and 2)Document4 pagesExercise 3.3: CRD and Post Hoc Test (Practice Exercises 1 and 2)Dawn Ilish Nicole DiezNo ratings yet
- STI - 03 - Data Presentation & ParameterDocument47 pagesSTI - 03 - Data Presentation & ParameterMuhamad Abi HaykalNo ratings yet
- What Is KNNDocument9 pagesWhat Is KNNvaishalikarvir26No ratings yet
- Data Analytics ResumeDocument4 pagesData Analytics Resumeafllueyey100% (1)
- Some Methods of Detection of Outliers in Linear Regression Model-Ranjit PDFDocument19 pagesSome Methods of Detection of Outliers in Linear Regression Model-Ranjit PDFmuralidharanNo ratings yet
- A320 Series Flight DataDocument142 pagesA320 Series Flight DataRaniero FalzonNo ratings yet
- Hydrology AssignmentDocument6 pagesHydrology AssignmentHopeson NazombeNo ratings yet
- Megan Bryant Hw2Document14 pagesMegan Bryant Hw2meganNo ratings yet
- Analisis Perhitungan Metode InterpolasiDocument7 pagesAnalisis Perhitungan Metode InterpolasiArina Mana SikanaNo ratings yet
- STAT 4800: Homework Assignment #3Document2 pagesSTAT 4800: Homework Assignment #3Muhammad AsifNo ratings yet
- DS&BD Lab ManulDocument98 pagesDS&BD Lab ManulAjeet GuptaNo ratings yet
- Project Report On Customer Lifetime ValueDocument23 pagesProject Report On Customer Lifetime ValueShubham EkapureNo ratings yet
- Dissertation Report On E-Tailing/electronic RetailingDocument41 pagesDissertation Report On E-Tailing/electronic RetailingSatyabrata Sahu100% (1)
- Chapter1 PDFDocument54 pagesChapter1 PDFdebojyotiNo ratings yet
- Assignment 2 QTBDocument5 pagesAssignment 2 QTBTamanna KotnalaNo ratings yet
- Standard Deviation QuizDocument1 pageStandard Deviation QuizEmerin RioNo ratings yet
- BCGZrbIgSUOhma2yIGlDWw BF C2 W4a Seasonal Dummy VariablesDocument19 pagesBCGZrbIgSUOhma2yIGlDWw BF C2 W4a Seasonal Dummy VariablesManuel Alejandro Sanabria AmayaNo ratings yet
- RegressionDocument3 pagesRegressionaraceliNo ratings yet
- Frequency Distribution, Cross-Tabulation, and Hypothesis TestingDocument4 pagesFrequency Distribution, Cross-Tabulation, and Hypothesis TestingThùyy VyNo ratings yet
- Mid-Semester Regular Data Mining QP v1 PDFDocument2 pagesMid-Semester Regular Data Mining QP v1 PDFsangeetha kNo ratings yet
- Revised Research Chapter 1 and 2Document18 pagesRevised Research Chapter 1 and 2Swayzel Sta MonicaNo ratings yet
- What Is Exploratory Data Analysis - by Prasad Patil - Towards Data ScienceDocument17 pagesWhat Is Exploratory Data Analysis - by Prasad Patil - Towards Data SciencephilipNo ratings yet
- Questions For Quantitative Research From Units 1 To 4Document10 pagesQuestions For Quantitative Research From Units 1 To 4IvanNo ratings yet
- Elementary Statistics: Describing, Exploring, and Comparing DataDocument31 pagesElementary Statistics: Describing, Exploring, and Comparing DataNatalie MigoyaNo ratings yet
- Course: Statistiek Voor PremastersDocument51 pagesCourse: Statistiek Voor PremastersLucas AalbersNo ratings yet