Download as pdf or txt
You might also like
- Erase HerpesDocument73 pagesErase HerpesObaraMeyi71% (7)
- Artikel 2 LDocument6 pagesArtikel 2 L.No ratings yet
- Sportsmedicineandphysfitness (Jurnal Sport)Document17 pagesSportsmedicineandphysfitness (Jurnal Sport)Fadhli Al FaruqNo ratings yet
- Melese 2020 - Effectiveness of Kinesiotaping OA Knee SRMA jpr-13-1267Document10 pagesMelese 2020 - Effectiveness of Kinesiotaping OA Knee SRMA jpr-13-1267Ikhsan JohnsonNo ratings yet
- Work Related Musculoskeletal Disorders in Physiotherapists Challenges and Coping Strategies WRMSDs in PhysiotherapistsDocument5 pagesWork Related Musculoskeletal Disorders in Physiotherapists Challenges and Coping Strategies WRMSDs in PhysiotherapistsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Efcacy of Acupuncture CombinedDocument21 pagesEfcacy of Acupuncture Combined4evertigerNo ratings yet
- Stuck-Moving Needle Acupuncture Myofascial Trigger Point To Treat Idiopathic Frozen Shoulder: Study Protocol For A Randomized Controlled TrialDocument13 pagesStuck-Moving Needle Acupuncture Myofascial Trigger Point To Treat Idiopathic Frozen Shoulder: Study Protocol For A Randomized Controlled TrialCarl MacCordNo ratings yet
- Role of Electrotherapy in Treating Chronic Musculoskeletal Conditions: A Narrative Review of The Last 5 YearsDocument14 pagesRole of Electrotherapy in Treating Chronic Musculoskeletal Conditions: A Narrative Review of The Last 5 YearsInternational Health ReviewNo ratings yet
- To Explore The Effect of Exergames For Increasing The Ranges of The Shoulder Joint in Incomplete Spinal Cord Injury Patients: A Case StudyDocument5 pagesTo Explore The Effect of Exergames For Increasing The Ranges of The Shoulder Joint in Incomplete Spinal Cord Injury Patients: A Case StudyIJAR JOURNALNo ratings yet
- Fmed 09 956188Document21 pagesFmed 09 956188NataliaNo ratings yet
- Art - 253A10.1186 - 252F1746 1340 18 23Document8 pagesArt - 253A10.1186 - 252F1746 1340 18 23im6002643No ratings yet
- Assessment of Quadriceps Muscle Thickness Using BedsideDocument9 pagesAssessment of Quadriceps Muscle Thickness Using BedsideJoaquin LopezNo ratings yet
- The Effect of Exercise Therapy On Knee Osteoarthritis: A Randomized Clinical TrialDocument10 pagesThe Effect of Exercise Therapy On Knee Osteoarthritis: A Randomized Clinical TrialElva Diany SyamsudinNo ratings yet
- Efficacy of High-Intensity Home Mechanical Stretch Therapy For Treatment of Shoulder Stiffness A Retrospective Review PDFDocument9 pagesEfficacy of High-Intensity Home Mechanical Stretch Therapy For Treatment of Shoulder Stiffness A Retrospective Review PDFDaniel Ruiz VallejoNo ratings yet
- Kapusta J. 2022. Long Term Effectiveness ESWT Plantar Fasciitis in Amateur Runners.Document11 pagesKapusta J. 2022. Long Term Effectiveness ESWT Plantar Fasciitis in Amateur Runners.Javier MartinNo ratings yet
- OsteoarthritisDocument8 pagesOsteoarthritisTobe Healty UseNo ratings yet
- The Global Summit On The Efficacy and EfDocument23 pagesThe Global Summit On The Efficacy and EfMirtaNo ratings yet
- 7218-Article Text-53915-1-10-20231229Document8 pages7218-Article Text-53915-1-10-20231229popa.ion1213No ratings yet
- Musculoskeletal Care - 2024 - Powell - Is Exercise Therapy The Right Treatment For Rotator Cuff Related Shoulder PainDocument12 pagesMusculoskeletal Care - 2024 - Powell - Is Exercise Therapy The Right Treatment For Rotator Cuff Related Shoulder PainxurraNo ratings yet
- Spinal Cord Injury RehabilitationDocument9 pagesSpinal Cord Injury RehabilitationVaibhav BhatiaNo ratings yet
- 1 s2.0 S0003999319303892 MainDocument8 pages1 s2.0 S0003999319303892 MainRizkyrafiqoh afdinNo ratings yet
- Burger Et Al 2016 Effect of Corticosteroid Injections Versus Physiotherapy On Pain Shoulder Range of Motion andDocument9 pagesBurger Et Al 2016 Effect of Corticosteroid Injections Versus Physiotherapy On Pain Shoulder Range of Motion andchandni saxenaNo ratings yet
- Total Knee ArthroplastyDocument35 pagesTotal Knee ArthroplastyAngela Maria Valero BorjaNo ratings yet
- Self EfficacyDocument11 pagesSelf EfficacyjeprastNo ratings yet
- The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisDocument21 pagesThe Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-Analysisilham Maulana ArifNo ratings yet
- Elnady2020 Article InShoulderAdhesiveCapsulitisUlDocument10 pagesElnady2020 Article InShoulderAdhesiveCapsulitisUlMarcus YoonNo ratings yet
- A Brief Note On Orthopedic PhysiotherapyDocument2 pagesA Brief Note On Orthopedic Physiotherapyasfand khanNo ratings yet
- 029 2020-Trofa-The-evidence-for-common-nonsurgicalDocument8 pages029 2020-Trofa-The-evidence-for-common-nonsurgicalTamara DalidetNo ratings yet
- PublishedversionDocument7 pagesPublishedversionAsvino SheejNo ratings yet
- Jurnal Total Knee ArthroplastyDocument9 pagesJurnal Total Knee ArthroplastykiranaNo ratings yet
- Hand Grip Strength As A Proposed New Vital Sign of Health: A Narrative Review of EvidencesDocument14 pagesHand Grip Strength As A Proposed New Vital Sign of Health: A Narrative Review of EvidencesAlex LimaNo ratings yet
- Exercises For Hand Osteoarthritis A Systematic Review of Clinical Practice Guidelines and Consensus RecommendationsDocument17 pagesExercises For Hand Osteoarthritis A Systematic Review of Clinical Practice Guidelines and Consensus RecommendationsMICHAEL ERNESTO QUINCHE RODRIGUEZNo ratings yet
- Effectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee OsteoarthritisDocument17 pagesEffectiveness of An 11-Week Exercise Intervention For Patients With Hip or Knee Osteoarthritisyago.pessoaNo ratings yet
- DexamethasoneDocument12 pagesDexamethasoneDenilson BarbosaNo ratings yet
- Effect of Swedish Massage and Hot Mud With Calotropis Gigantea Application Among Knee Joint Osteoarthritis Cases-A Randomized Control TrialDocument5 pagesEffect of Swedish Massage and Hot Mud With Calotropis Gigantea Application Among Knee Joint Osteoarthritis Cases-A Randomized Control TrialIJAR JOURNALNo ratings yet
- Knee Osteoarthritis: An Overview of Recent Interventions: Bijeet Bardoloi, Chungki Bhutia, Dinesh Bhatia, Sudip PaulDocument18 pagesKnee Osteoarthritis: An Overview of Recent Interventions: Bijeet Bardoloi, Chungki Bhutia, Dinesh Bhatia, Sudip PaultiaanastaNo ratings yet
- Does Ultrasonography Guided Steroid Injections Provide Better Outcome in Shoulder Impingement Syndrome? A Prospective StudyDocument12 pagesDoes Ultrasonography Guided Steroid Injections Provide Better Outcome in Shoulder Impingement Syndrome? A Prospective StudyIJAR JOURNALNo ratings yet
- Cam Lecture NotesDocument8 pagesCam Lecture Notesapi-601041704No ratings yet
- Applsci 11 04338 v2Document9 pagesApplsci 11 04338 v2Sherly L WaromiNo ratings yet
- The Effect of Dry Needling On The Radiating Pain in Subjects With Discogenic Low Back Pain: A Randomized Control TrialDocument8 pagesThe Effect of Dry Needling On The Radiating Pain in Subjects With Discogenic Low Back Pain: A Randomized Control TrialValeria AlfaroNo ratings yet
- Effectiveness of Positional Release TechDocument4 pagesEffectiveness of Positional Release TechEdo okati leNo ratings yet
- Evaluating Meridian-Sinew Release Therapy For The Treatment of Knee OsteoarthritisDocument10 pagesEvaluating Meridian-Sinew Release Therapy For The Treatment of Knee OsteoarthritisGuilherme PenicheNo ratings yet
- Joana Ortho ArticleDocument13 pagesJoana Ortho ArticleIrish CostalesNo ratings yet
- CPG RESTRAIN GuidelinesDocument8 pagesCPG RESTRAIN GuidelinesaartiNo ratings yet
- Home-Based Management of Knee Osteoarthrosis During Covid Pandemic 2020Document7 pagesHome-Based Management of Knee Osteoarthrosis During Covid Pandemic 2020Gonzalo JimenezNo ratings yet
- TheEffectofDeepFrictionMassageversus PDFDocument8 pagesTheEffectofDeepFrictionMassageversus PDFRiniaridhaNo ratings yet
- Physical Therapy For Cerebellar Ataxia PDFDocument19 pagesPhysical Therapy For Cerebellar Ataxia PDFAmylase Trypsin100% (1)
- The Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewDocument7 pagesThe Impact of Long-Term Follow-Up On Total Hip Arthroplasty: A Systematic ReviewIJAR JOURNALNo ratings yet
- Arthritis Care Research - 2016 - de Rooij - Efficacy of Tailored Exercise Therapy On Physical Functioning in PatientsDocument10 pagesArthritis Care Research - 2016 - de Rooij - Efficacy of Tailored Exercise Therapy On Physical Functioning in PatientsToli kkakrNo ratings yet
- Acupuncture Treatment On The Motor Area of The Sca PDFDocument12 pagesAcupuncture Treatment On The Motor Area of The Sca PDFSANGGA BUWANANo ratings yet
- The Effectiveness of Massage Therapy For The Treatment of Nonspesific LBPDocument9 pagesThe Effectiveness of Massage Therapy For The Treatment of Nonspesific LBPFirmansah SaputraNo ratings yet
- The Effectiveness of A 12 Week Exercise Programme in Hip Osteoarthritis A Randomised Controlled TrialDocument6 pagesThe Effectiveness of A 12 Week Exercise Programme in Hip Osteoarthritis A Randomised Controlled TrialHerald Scholarly Open AccessNo ratings yet
- Osteoartritis 2022 OarsiDocument10 pagesOsteoartritis 2022 OarsiJorge GámezNo ratings yet
- Effectiveness of Intradialytic Stretching Exercise On Pain Due To Muscle Cramps Among Patients Undergoing HaemodialysisDocument7 pagesEffectiveness of Intradialytic Stretching Exercise On Pain Due To Muscle Cramps Among Patients Undergoing HaemodialysisAhmad IsmailNo ratings yet
- The Short-Term Effects of Hydrotherapy On Pain and Self-Perceived Functional Status in Individuals Living With Osteoarthritis of The Knee JointDocument6 pagesThe Short-Term Effects of Hydrotherapy On Pain and Self-Perceived Functional Status in Individuals Living With Osteoarthritis of The Knee JointMiftah ghaniNo ratings yet
- Quadriceps Arthrogenic Muscle Inhibition: The Effects of Experimental Knee Joint Effusion On Motor Cortex ExcitabilityDocument7 pagesQuadriceps Arthrogenic Muscle Inhibition: The Effects of Experimental Knee Joint Effusion On Motor Cortex ExcitabilityPedro SimõesNo ratings yet
- Article 1Document10 pagesArticle 1Rashmi SheelvantNo ratings yet
- Design The Upper Limb Exoskeleton Arm For Reinforcement The Weakness in The Human MusclesDocument8 pagesDesign The Upper Limb Exoskeleton Arm For Reinforcement The Weakness in The Human MusclesYASH SANJAY.INGLENo ratings yet
- Prevention of Muscle Atrophy in ICUDocument10 pagesPrevention of Muscle Atrophy in ICUCamilo OsorioNo ratings yet
- Myoskeletal Injuries in The Podiatric ProfessionDocument10 pagesMyoskeletal Injuries in The Podiatric ProfessionelproedrosNo ratings yet
- Sports Hernia and Athletic Pubalgia: Diagnosis and TreatmentFrom EverandSports Hernia and Athletic Pubalgia: Diagnosis and TreatmentDavid R. DiduchNo ratings yet
- Thyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Document11 pagesThyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Vaishnavi SheteNo ratings yet
- Infant Massage: Manual TherapiesDocument13 pagesInfant Massage: Manual Therapiesdian100% (1)
- Therapy - TranslatedDocument66 pagesTherapy - TranslatedMashashi MatsumotoNo ratings yet
- Use of Antibiotics For Acute Respiratory Infection (ARI) in Puskesmas Karang Rejo, TarakanDocument7 pagesUse of Antibiotics For Acute Respiratory Infection (ARI) in Puskesmas Karang Rejo, TarakanAugust WattimenaNo ratings yet
- Hospital and Healthcare FacilitiesDocument23 pagesHospital and Healthcare FacilitiesGueanne ConsolacionNo ratings yet
- What Are The Different Ways in Which A Genetic Condition Can Be Inherited?Document4 pagesWhat Are The Different Ways in Which A Genetic Condition Can Be Inherited?Chad ParasNo ratings yet
- TizanidineDocument2 pagesTizanidinebhawanisrNo ratings yet
- Quality Indicators Key ProcessesDocument8 pagesQuality Indicators Key ProcessesAlexandr ChuvakovNo ratings yet
- Notice: Meetings: Recognized Standards List Modifications (Recognition List Number 018)Document12 pagesNotice: Meetings: Recognized Standards List Modifications (Recognition List Number 018)Justia.comNo ratings yet
- Community Diagnosis of Purok Teresita, Barangay Buhangin Proper 1, Buhangin Davao CityDocument80 pagesCommunity Diagnosis of Purok Teresita, Barangay Buhangin Proper 1, Buhangin Davao CitySabesh DhoniNo ratings yet
- (English (Auto-Generated) ) Vaccines Vs Reality Dr. Andrew Kaufman (DownSub - Com)Document133 pages(English (Auto-Generated) ) Vaccines Vs Reality Dr. Andrew Kaufman (DownSub - Com)Indira MaycellaNo ratings yet
- Att Schedule 2014Document316 pagesAtt Schedule 2014adllurikaushikNo ratings yet
- Strategies For Dementia Prevention: Latest Evidence and ImplicationsDocument16 pagesStrategies For Dementia Prevention: Latest Evidence and ImplicationsRitmaNo ratings yet
- 50-Year-Old Man Overcomes His Battle With Lung Cancer Using Cannabis Oil, Stuns CBS NewsDocument16 pages50-Year-Old Man Overcomes His Battle With Lung Cancer Using Cannabis Oil, Stuns CBS Newstahirmaqpk100% (1)
- Teleconference 23 Juli 2019Document11 pagesTeleconference 23 Juli 2019Vita DesriantiNo ratings yet
- 15-28 - Intestinal Motility DisordersDocument5 pages15-28 - Intestinal Motility DisordersHanako AranillaNo ratings yet
- Chest Guidelines - WarfarinDocument41 pagesChest Guidelines - Warfarinkedaw100% (1)
- Assembly PENNAGARAM GH 2019Document15 pagesAssembly PENNAGARAM GH 2019jdhs dharmapuriNo ratings yet
- Full Mouth Rehabilitation ProgramDocument4 pagesFull Mouth Rehabilitation ProgramAnuRaveendranNo ratings yet
- Allergic Rhinitis and RhinosinusitisDocument53 pagesAllergic Rhinitis and RhinosinusitisSinta FiraniNo ratings yet
- Module 6Document4 pagesModule 6Leah LlobellNo ratings yet
- Ophtha TMC Lec3Document16 pagesOphtha TMC Lec3Anonymous ic2CDkFNo ratings yet
- Concept MapDocument1 pageConcept MapKatrineNo ratings yet
- Research Proposal First Draft (Adamu Moti)Document25 pagesResearch Proposal First Draft (Adamu Moti)ODAA TUBENo ratings yet
- Tacrolimus in DermatologyDocument4 pagesTacrolimus in DermatologyDimas PrajagoptaNo ratings yet
- ICD X Gigi Dan Mulut P Care BPJS 2019Document4 pagesICD X Gigi Dan Mulut P Care BPJS 2019puskesmassonggonNo ratings yet
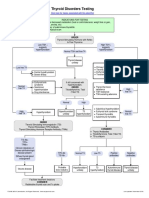
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperNo ratings yet
- Case01.Acute PainDocument56 pagesCase01.Acute PainshairaorquetaNo ratings yet
- Puzzle Human Body OrgansDocument3 pagesPuzzle Human Body OrgansMaria Zennin ReballosNo ratings yet