
Week 8 - Assessment of The Ears
Week 8 - Assessment of The Ears
You might also like
- 100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and RationalesDocument28 pages100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and RationalesAijem Ryan93% (138)
- Otorhinolaryngology NotesDocument25 pagesOtorhinolaryngology NotesFako Filipinas100% (3)
- Comprehensive Board Exam ENT PDFDocument644 pagesComprehensive Board Exam ENT PDFdrskbarla50% (2)
- Schwartz's Hour Notes On TraumaDocument19 pagesSchwartz's Hour Notes On TraumaEver Seneca EscaLera100% (2)
- Anterior Triangle of The Neck JDVDocument5 pagesAnterior Triangle of The Neck JDVNica Lopez Fernandez100% (3)
- Assessment and Identification of Needs PDFDocument637 pagesAssessment and Identification of Needs PDFlbchongthu100% (1)
- H.A. Lec (L7 B) - Assessing Head and Neck, Eyes and Visual Acuity, Ears and BalanceDocument4 pagesH.A. Lec (L7 B) - Assessing Head and Neck, Eyes and Visual Acuity, Ears and BalanceCastallia LascuñaNo ratings yet
- MED OSCE NOTES: ChecklistsDocument14 pagesMED OSCE NOTES: ChecklistsBatch 2024 Internal MedicineNo ratings yet
- Zoology Mammals (Rabbit)Document3 pagesZoology Mammals (Rabbit)PerrieNo ratings yet
- MCN L ReviewerDocument8 pagesMCN L ReviewerkimaytacordaNo ratings yet
- S3-06 Ophthalmology Eyelid, Lacrimal - Orbital Disorders (v2) PDFDocument13 pagesS3-06 Ophthalmology Eyelid, Lacrimal - Orbital Disorders (v2) PDFAl SyNo ratings yet
- M4 - Didactic - NCM 118Document4 pagesM4 - Didactic - NCM 118KARL FESARITNo ratings yet
- Deafness For Medical Finals (Based On Newcastle University Learning Outcomes)Document7 pagesDeafness For Medical Finals (Based On Newcastle University Learning Outcomes)RedTabsNo ratings yet
- Pa PudDocument7 pagesPa PudJannetAsisNo ratings yet
- HA Notes FinalsDocument109 pagesHA Notes FinalsPERALTA, Airish Angel J.No ratings yet
- (Surgery) 3.03 General Principles of Trauma - Dr. LicupDocument12 pages(Surgery) 3.03 General Principles of Trauma - Dr. LicupKim DeeNo ratings yet
- Anne G Osborn MD FACR, Karen L Salzman MD, Jeffrey S Anderson MD-23-44Document22 pagesAnne G Osborn MD FACR, Karen L Salzman MD, Jeffrey S Anderson MD-23-44angulomareling9No ratings yet
- Cranial NervesDocument9 pagesCranial NervesRabin TacderNo ratings yet
- ProstodonciaDocument8 pagesProstodonciajaaa212163100% (1)
- Ha Semi FinalsDocument16 pagesHa Semi FinalsHielal DumpNo ratings yet
- Physical Assessment Head and NeckDocument75 pagesPhysical Assessment Head and NeckDeeeee100% (2)
- (ENT) 1.02 External Diseases of The Ear - Sia Vargas (Aug 12)Document22 pages(ENT) 1.02 External Diseases of The Ear - Sia Vargas (Aug 12)Noreen Hannah GabrielNo ratings yet
- Cephalocaudal KemerutDocument10 pagesCephalocaudal KemerutKIANA LOUISE ROMANONo ratings yet
- RadiologíaDocument12 pagesRadiologíaevelyn caballeeo odarNo ratings yet
- Extra Edge Info: OpthDocument2 pagesExtra Edge Info: OpthskNo ratings yet
- Week 6 - Assessment of The Head and NeckDocument4 pagesWeek 6 - Assessment of The Head and NeckJuan Miguel TevesNo ratings yet
- 6 - 12 NotesDocument5 pages6 - 12 NotesFefe JejeNo ratings yet
- Periodontics PDFDocument28 pagesPeriodontics PDFtriciaNo ratings yet
- 5.23 SURG II Abdominal Wall and Inguinal HerniasDocument8 pages5.23 SURG II Abdominal Wall and Inguinal HerniasSheila Lyn LacsonNo ratings yet
- Pedia Report 13Document10 pagesPedia Report 13laurie.charlynjaneNo ratings yet
- SGD Case Bustamante Patricia MaricDocument30 pagesSGD Case Bustamante Patricia MaricJewelNo ratings yet
- Head and Neck Assessment NursingDocument8 pagesHead and Neck Assessment NursingNicks NacarioNo ratings yet
- Head and Neck Assessment NursingDocument8 pagesHead and Neck Assessment NursingNicks NacarioNo ratings yet
- Introduction To Animal Morph and AnatomyDocument5 pagesIntroduction To Animal Morph and AnatomyReanna NoelNo ratings yet
- (ENT) 1.04 Problems of Inner Ear 1 - Calavera (Aug 24)Document11 pages(ENT) 1.04 Problems of Inner Ear 1 - Calavera (Aug 24)Noreen Hannah GabrielNo ratings yet
- PHYSIOLOGY EXAM - Orig 1 1Document6 pagesPHYSIOLOGY EXAM - Orig 1 1thelmaaguinawangNo ratings yet
- 2024 ENT Trans04 DiseasesoftheEarPart1Document7 pages2024 ENT Trans04 DiseasesoftheEarPart1EADOH RO2No ratings yet
- ANA.S4.CA21.Female Reproductive SystempdfDocument6 pagesANA.S4.CA21.Female Reproductive SystempdfCazz HeyNo ratings yet
- Trauma Module FinalDocument34 pagesTrauma Module FinalMarian YuqueNo ratings yet
- Maternal AnatomyDocument9 pagesMaternal AnatomyAika Agudilla100% (2)
- RhinoplastyDocument86 pagesRhinoplastyyashobantab2021No ratings yet
- 2 Assessment of The EarsDocument8 pages2 Assessment of The EarsKeith Chastine Miraballes100% (1)
- Assessment of The Ears - StudentDocument8 pagesAssessment of The Ears - StudentSherinne Jane CariazoNo ratings yet
- Trans Oto 14 ENT EmergenciesDocument8 pagesTrans Oto 14 ENT EmergenciesAbegail IbañezNo ratings yet
- 8.2 Inguinal Hernias, PUV, and VUR - March 14 - Dr. Gellido & Dr. LawenkoDocument8 pages8.2 Inguinal Hernias, PUV, and VUR - March 14 - Dr. Gellido & Dr. LawenkoJess PeltraNo ratings yet
- 2 Newborn AssesmentDocument23 pages2 Newborn Assesment.No ratings yet
- Assessing The Nose and SinusesDocument5 pagesAssessing The Nose and SinusesYudi TrigunaNo ratings yet
- Acd 3: Neck: Clinical ImportanceDocument11 pagesAcd 3: Neck: Clinical Importancestudent10100No ratings yet
- High Risk Labour FinalDocument60 pagesHigh Risk Labour FinalSusan HepziNo ratings yet
- HEALTH ASSESSMENT - Breasts & Regional LymphaticsDocument5 pagesHEALTH ASSESSMENT - Breasts & Regional LymphaticsMich Hiel OforraNo ratings yet
- Cirugi Ì ADocument7 pagesCirugi Ì Ab64hwmkpckNo ratings yet
- Assessment Method Used Normal Findings: Head Head Is Free FromDocument6 pagesAssessment Method Used Normal Findings: Head Head Is Free FromGil PerezNo ratings yet
- French 16 - Inguinal HerniasDocument8 pagesFrench 16 - Inguinal HerniasPrince VallejosNo ratings yet
- Basic Physical Assessment Guide 9282010Document1 pageBasic Physical Assessment Guide 9282010Hau WangNo ratings yet
- Nasal Blockage & Sinus Disease 2Document40 pagesNasal Blockage & Sinus Disease 2HanahigaNo ratings yet
- BIO 271 Study Questions Ch. 15: Ear DisordersDocument8 pagesBIO 271 Study Questions Ch. 15: Ear Disorderskelsey jacksonNo ratings yet
- PAEDS OSCE ReviewDocument64 pagesPAEDS OSCE Reviewamanda deonananNo ratings yet
- General Assessment: Additional Notes: BlueDocument4 pagesGeneral Assessment: Additional Notes: BlueKaiken DukeNo ratings yet
- Health AssessmentDocument13 pagesHealth AssessmentJasmin MolanoNo ratings yet
- Ped - Pcc.s1.l04.clinico-Radiologic Correlation (D)Document6 pagesPed - Pcc.s1.l04.clinico-Radiologic Correlation (D)VICTOR AMORESNo ratings yet
- Physical AssessmentDocument90 pagesPhysical AssessmentReann LeeNo ratings yet
- Oral Physiology Reviewer 1Document51 pagesOral Physiology Reviewer 1recuenco.2019100868No ratings yet
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- ParasitologyDocument4 pagesParasitologyJuan Miguel TevesNo ratings yet
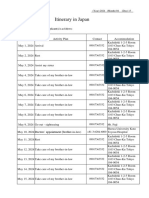
- Itinerary in Japan: The Travel Itinerary of The Visa Applicant(s) Is As FollowsDocument2 pagesItinerary in Japan: The Travel Itinerary of The Visa Applicant(s) Is As FollowsJuan Miguel TevesNo ratings yet
- CU 9. Evaluation Documentation of Health Education.Document7 pagesCU 9. Evaluation Documentation of Health Education.Juan Miguel TevesNo ratings yet
- Comms 3 LEC FrontpageDocument28 pagesComms 3 LEC FrontpageJuan Miguel TevesNo ratings yet
- CU 7 Developing Health Education PlanDocument9 pagesCU 7 Developing Health Education PlanJuan Miguel TevesNo ratings yet
- Teves Icc Act1Document2 pagesTeves Icc Act1Juan Miguel TevesNo ratings yet
- Emona Volume 1 Experiment PCM-codingDocument18 pagesEmona Volume 1 Experiment PCM-codingJuan Miguel TevesNo ratings yet
- Week 10 - Assessment of The Thorax and LungsDocument8 pagesWeek 10 - Assessment of The Thorax and LungsJuan Miguel TevesNo ratings yet
- STAS Midterm ReviewerDocument8 pagesSTAS Midterm ReviewerJuan Miguel TevesNo ratings yet
- MicrobiologyDocument5 pagesMicrobiologyJuan Miguel TevesNo ratings yet
- Data Communication CodesDocument12 pagesData Communication CodesJuan Miguel TevesNo ratings yet
- Special Senses 1Document14 pagesSpecial Senses 1Juan Miguel TevesNo ratings yet
- Cellular Structures and FunctionsDocument3 pagesCellular Structures and FunctionsJuan Miguel TevesNo ratings yet
- IPAQDocument3 pagesIPAQJuan Miguel TevesNo ratings yet
- 2022 Par QDocument4 pages2022 Par QJuan Miguel TevesNo ratings yet
- Rules and Regulation in VolleyballDocument2 pagesRules and Regulation in VolleyballJuan Miguel TevesNo ratings yet
- Special LawDocument8 pagesSpecial LawJuan Miguel TevesNo ratings yet
- Investment and Portfolio Management - BookDocument40 pagesInvestment and Portfolio Management - BookJuan Miguel TevesNo ratings yet
- A. It Consists of Squamous EpitheliumDocument7 pagesA. It Consists of Squamous EpitheliumUzair KhanNo ratings yet
- Hearing ImpairmentDocument20 pagesHearing ImpairmentAlexandra Villaflor HernandezNo ratings yet
- MEDSURG II (2nd Sem - ENDTERM NOTES)Document39 pagesMEDSURG II (2nd Sem - ENDTERM NOTES)Meryville JacildoNo ratings yet
- Middle Ear ImplantsDocument5 pagesMiddle Ear ImplantsPrakashNo ratings yet
- Assessment of HearingDocument51 pagesAssessment of HearingSwetha PasupuletiNo ratings yet
- 75 Ent Questions Rajiv DhawanDocument182 pages75 Ent Questions Rajiv DhawanexplorerheavyNo ratings yet
- Ent Pyq's by DR SaraDocument50 pagesEnt Pyq's by DR SaraAstlin JNo ratings yet
- ENT MCQ (Not Answered)Document75 pagesENT MCQ (Not Answered)mohamed mowafeyNo ratings yet
- Advance ReadDocument8 pagesAdvance ReadKeziah GhaileNo ratings yet
- Tes Garpu TalaDocument13 pagesTes Garpu TalaSamuel ChristianNo ratings yet
- Yilkal Zemene, M.D., ENT, Head and Neck Surgeon Mekelle University, MekelleDocument34 pagesYilkal Zemene, M.D., ENT, Head and Neck Surgeon Mekelle University, MekelleruthNo ratings yet
- Hearing LossDocument22 pagesHearing Losssimran kaurNo ratings yet
- Eye and Ears AssessmentDocument17 pagesEye and Ears AssessmentPrincess Añabeza100% (1)
- Assessing EarsDocument11 pagesAssessing EarsRhea Mae Visda RoaNo ratings yet
- FTC 106 G3Document15 pagesFTC 106 G3Ann YeongNo ratings yet
- OtosclerosisDocument9 pagesOtosclerosisSuprit SnNo ratings yet
- Hearing LossDocument9 pagesHearing Lossvicky singhNo ratings yet
- Clinical Neurology: Week 4 Lectures 7 and 8Document74 pagesClinical Neurology: Week 4 Lectures 7 and 8Miss BNo ratings yet
- Ear AssessmentDocument23 pagesEar AssessmentRotsen B. VelascoNo ratings yet
- ENT Ear I Scenarios (Compiled)Document35 pagesENT Ear I Scenarios (Compiled)rumman tariqNo ratings yet
- Anatomy and Physiology: External EarDocument73 pagesAnatomy and Physiology: External Earvidge5No ratings yet
- Lecture 2 - Audiometry PracticalDocument42 pagesLecture 2 - Audiometry PracticalSaera Hafiz Nikita100% (1)
- Aiims ENTDocument92 pagesAiims ENTSagar MukherjeeNo ratings yet
- Multiple Disability Original HandoutDocument42 pagesMultiple Disability Original HandoutHabtamu DebasuNo ratings yet
- Audiogram Interpretation Summary Slides 1 4Document31 pagesAudiogram Interpretation Summary Slides 1 4api-506629610No ratings yet
- Hearing-Impairment Case StudyDocument10 pagesHearing-Impairment Case StudyIrish Eunice Felix100% (1)
- Canalplasty For ExostosisDocument10 pagesCanalplasty For ExostosisRamya KamathNo ratings yet








































































































Download as pdf or txt
You might also like
- 100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and RationalesDocument28 pages100 Item MEDICAL SURGICAL Nursing Examination Correct Answers and RationalesAijem Ryan93% (138)
- Otorhinolaryngology NotesDocument25 pagesOtorhinolaryngology NotesFako Filipinas100% (3)
- Comprehensive Board Exam ENT PDFDocument644 pagesComprehensive Board Exam ENT PDFdrskbarla50% (2)
- Schwartz's Hour Notes On TraumaDocument19 pagesSchwartz's Hour Notes On TraumaEver Seneca EscaLera100% (2)
- Anterior Triangle of The Neck JDVDocument5 pagesAnterior Triangle of The Neck JDVNica Lopez Fernandez100% (3)
- Assessment and Identification of Needs PDFDocument637 pagesAssessment and Identification of Needs PDFlbchongthu100% (1)
- H.A. Lec (L7 B) - Assessing Head and Neck, Eyes and Visual Acuity, Ears and BalanceDocument4 pagesH.A. Lec (L7 B) - Assessing Head and Neck, Eyes and Visual Acuity, Ears and BalanceCastallia LascuñaNo ratings yet
- MED OSCE NOTES: ChecklistsDocument14 pagesMED OSCE NOTES: ChecklistsBatch 2024 Internal MedicineNo ratings yet
- Zoology Mammals (Rabbit)Document3 pagesZoology Mammals (Rabbit)PerrieNo ratings yet
- MCN L ReviewerDocument8 pagesMCN L ReviewerkimaytacordaNo ratings yet
- S3-06 Ophthalmology Eyelid, Lacrimal - Orbital Disorders (v2) PDFDocument13 pagesS3-06 Ophthalmology Eyelid, Lacrimal - Orbital Disorders (v2) PDFAl SyNo ratings yet
- M4 - Didactic - NCM 118Document4 pagesM4 - Didactic - NCM 118KARL FESARITNo ratings yet
- Deafness For Medical Finals (Based On Newcastle University Learning Outcomes)Document7 pagesDeafness For Medical Finals (Based On Newcastle University Learning Outcomes)RedTabsNo ratings yet
- Pa PudDocument7 pagesPa PudJannetAsisNo ratings yet
- HA Notes FinalsDocument109 pagesHA Notes FinalsPERALTA, Airish Angel J.No ratings yet
- (Surgery) 3.03 General Principles of Trauma - Dr. LicupDocument12 pages(Surgery) 3.03 General Principles of Trauma - Dr. LicupKim DeeNo ratings yet
- Anne G Osborn MD FACR, Karen L Salzman MD, Jeffrey S Anderson MD-23-44Document22 pagesAnne G Osborn MD FACR, Karen L Salzman MD, Jeffrey S Anderson MD-23-44angulomareling9No ratings yet
- Cranial NervesDocument9 pagesCranial NervesRabin TacderNo ratings yet
- ProstodonciaDocument8 pagesProstodonciajaaa212163100% (1)
- Ha Semi FinalsDocument16 pagesHa Semi FinalsHielal DumpNo ratings yet
- Physical Assessment Head and NeckDocument75 pagesPhysical Assessment Head and NeckDeeeee100% (2)
- (ENT) 1.02 External Diseases of The Ear - Sia Vargas (Aug 12)Document22 pages(ENT) 1.02 External Diseases of The Ear - Sia Vargas (Aug 12)Noreen Hannah GabrielNo ratings yet
- Cephalocaudal KemerutDocument10 pagesCephalocaudal KemerutKIANA LOUISE ROMANONo ratings yet
- RadiologíaDocument12 pagesRadiologíaevelyn caballeeo odarNo ratings yet
- Extra Edge Info: OpthDocument2 pagesExtra Edge Info: OpthskNo ratings yet
- Week 6 - Assessment of The Head and NeckDocument4 pagesWeek 6 - Assessment of The Head and NeckJuan Miguel TevesNo ratings yet
- 6 - 12 NotesDocument5 pages6 - 12 NotesFefe JejeNo ratings yet
- Periodontics PDFDocument28 pagesPeriodontics PDFtriciaNo ratings yet
- 5.23 SURG II Abdominal Wall and Inguinal HerniasDocument8 pages5.23 SURG II Abdominal Wall and Inguinal HerniasSheila Lyn LacsonNo ratings yet
- Pedia Report 13Document10 pagesPedia Report 13laurie.charlynjaneNo ratings yet
- SGD Case Bustamante Patricia MaricDocument30 pagesSGD Case Bustamante Patricia MaricJewelNo ratings yet
- Head and Neck Assessment NursingDocument8 pagesHead and Neck Assessment NursingNicks NacarioNo ratings yet
- Head and Neck Assessment NursingDocument8 pagesHead and Neck Assessment NursingNicks NacarioNo ratings yet
- Introduction To Animal Morph and AnatomyDocument5 pagesIntroduction To Animal Morph and AnatomyReanna NoelNo ratings yet
- (ENT) 1.04 Problems of Inner Ear 1 - Calavera (Aug 24)Document11 pages(ENT) 1.04 Problems of Inner Ear 1 - Calavera (Aug 24)Noreen Hannah GabrielNo ratings yet
- PHYSIOLOGY EXAM - Orig 1 1Document6 pagesPHYSIOLOGY EXAM - Orig 1 1thelmaaguinawangNo ratings yet
- 2024 ENT Trans04 DiseasesoftheEarPart1Document7 pages2024 ENT Trans04 DiseasesoftheEarPart1EADOH RO2No ratings yet
- ANA.S4.CA21.Female Reproductive SystempdfDocument6 pagesANA.S4.CA21.Female Reproductive SystempdfCazz HeyNo ratings yet
- Trauma Module FinalDocument34 pagesTrauma Module FinalMarian YuqueNo ratings yet
- Maternal AnatomyDocument9 pagesMaternal AnatomyAika Agudilla100% (2)
- RhinoplastyDocument86 pagesRhinoplastyyashobantab2021No ratings yet
- 2 Assessment of The EarsDocument8 pages2 Assessment of The EarsKeith Chastine Miraballes100% (1)
- Assessment of The Ears - StudentDocument8 pagesAssessment of The Ears - StudentSherinne Jane CariazoNo ratings yet
- Trans Oto 14 ENT EmergenciesDocument8 pagesTrans Oto 14 ENT EmergenciesAbegail IbañezNo ratings yet
- 8.2 Inguinal Hernias, PUV, and VUR - March 14 - Dr. Gellido & Dr. LawenkoDocument8 pages8.2 Inguinal Hernias, PUV, and VUR - March 14 - Dr. Gellido & Dr. LawenkoJess PeltraNo ratings yet
- 2 Newborn AssesmentDocument23 pages2 Newborn Assesment.No ratings yet
- Assessing The Nose and SinusesDocument5 pagesAssessing The Nose and SinusesYudi TrigunaNo ratings yet
- Acd 3: Neck: Clinical ImportanceDocument11 pagesAcd 3: Neck: Clinical Importancestudent10100No ratings yet
- High Risk Labour FinalDocument60 pagesHigh Risk Labour FinalSusan HepziNo ratings yet
- HEALTH ASSESSMENT - Breasts & Regional LymphaticsDocument5 pagesHEALTH ASSESSMENT - Breasts & Regional LymphaticsMich Hiel OforraNo ratings yet
- Cirugi Ì ADocument7 pagesCirugi Ì Ab64hwmkpckNo ratings yet
- Assessment Method Used Normal Findings: Head Head Is Free FromDocument6 pagesAssessment Method Used Normal Findings: Head Head Is Free FromGil PerezNo ratings yet
- French 16 - Inguinal HerniasDocument8 pagesFrench 16 - Inguinal HerniasPrince VallejosNo ratings yet
- Basic Physical Assessment Guide 9282010Document1 pageBasic Physical Assessment Guide 9282010Hau WangNo ratings yet
- Nasal Blockage & Sinus Disease 2Document40 pagesNasal Blockage & Sinus Disease 2HanahigaNo ratings yet
- BIO 271 Study Questions Ch. 15: Ear DisordersDocument8 pagesBIO 271 Study Questions Ch. 15: Ear Disorderskelsey jacksonNo ratings yet
- PAEDS OSCE ReviewDocument64 pagesPAEDS OSCE Reviewamanda deonananNo ratings yet
- General Assessment: Additional Notes: BlueDocument4 pagesGeneral Assessment: Additional Notes: BlueKaiken DukeNo ratings yet
- Health AssessmentDocument13 pagesHealth AssessmentJasmin MolanoNo ratings yet
- Ped - Pcc.s1.l04.clinico-Radiologic Correlation (D)Document6 pagesPed - Pcc.s1.l04.clinico-Radiologic Correlation (D)VICTOR AMORESNo ratings yet
- Physical AssessmentDocument90 pagesPhysical AssessmentReann LeeNo ratings yet
- Oral Physiology Reviewer 1Document51 pagesOral Physiology Reviewer 1recuenco.2019100868No ratings yet
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- ParasitologyDocument4 pagesParasitologyJuan Miguel TevesNo ratings yet
- Itinerary in Japan: The Travel Itinerary of The Visa Applicant(s) Is As FollowsDocument2 pagesItinerary in Japan: The Travel Itinerary of The Visa Applicant(s) Is As FollowsJuan Miguel TevesNo ratings yet
- CU 9. Evaluation Documentation of Health Education.Document7 pagesCU 9. Evaluation Documentation of Health Education.Juan Miguel TevesNo ratings yet
- Comms 3 LEC FrontpageDocument28 pagesComms 3 LEC FrontpageJuan Miguel TevesNo ratings yet
- CU 7 Developing Health Education PlanDocument9 pagesCU 7 Developing Health Education PlanJuan Miguel TevesNo ratings yet
- Teves Icc Act1Document2 pagesTeves Icc Act1Juan Miguel TevesNo ratings yet
- Emona Volume 1 Experiment PCM-codingDocument18 pagesEmona Volume 1 Experiment PCM-codingJuan Miguel TevesNo ratings yet
- Week 10 - Assessment of The Thorax and LungsDocument8 pagesWeek 10 - Assessment of The Thorax and LungsJuan Miguel TevesNo ratings yet
- STAS Midterm ReviewerDocument8 pagesSTAS Midterm ReviewerJuan Miguel TevesNo ratings yet
- MicrobiologyDocument5 pagesMicrobiologyJuan Miguel TevesNo ratings yet
- Data Communication CodesDocument12 pagesData Communication CodesJuan Miguel TevesNo ratings yet
- Special Senses 1Document14 pagesSpecial Senses 1Juan Miguel TevesNo ratings yet
- Cellular Structures and FunctionsDocument3 pagesCellular Structures and FunctionsJuan Miguel TevesNo ratings yet
- IPAQDocument3 pagesIPAQJuan Miguel TevesNo ratings yet
- 2022 Par QDocument4 pages2022 Par QJuan Miguel TevesNo ratings yet
- Rules and Regulation in VolleyballDocument2 pagesRules and Regulation in VolleyballJuan Miguel TevesNo ratings yet
- Special LawDocument8 pagesSpecial LawJuan Miguel TevesNo ratings yet
- Investment and Portfolio Management - BookDocument40 pagesInvestment and Portfolio Management - BookJuan Miguel TevesNo ratings yet
- A. It Consists of Squamous EpitheliumDocument7 pagesA. It Consists of Squamous EpitheliumUzair KhanNo ratings yet
- Hearing ImpairmentDocument20 pagesHearing ImpairmentAlexandra Villaflor HernandezNo ratings yet
- MEDSURG II (2nd Sem - ENDTERM NOTES)Document39 pagesMEDSURG II (2nd Sem - ENDTERM NOTES)Meryville JacildoNo ratings yet
- Middle Ear ImplantsDocument5 pagesMiddle Ear ImplantsPrakashNo ratings yet
- Assessment of HearingDocument51 pagesAssessment of HearingSwetha PasupuletiNo ratings yet
- 75 Ent Questions Rajiv DhawanDocument182 pages75 Ent Questions Rajiv DhawanexplorerheavyNo ratings yet
- Ent Pyq's by DR SaraDocument50 pagesEnt Pyq's by DR SaraAstlin JNo ratings yet
- ENT MCQ (Not Answered)Document75 pagesENT MCQ (Not Answered)mohamed mowafeyNo ratings yet
- Advance ReadDocument8 pagesAdvance ReadKeziah GhaileNo ratings yet
- Tes Garpu TalaDocument13 pagesTes Garpu TalaSamuel ChristianNo ratings yet
- Yilkal Zemene, M.D., ENT, Head and Neck Surgeon Mekelle University, MekelleDocument34 pagesYilkal Zemene, M.D., ENT, Head and Neck Surgeon Mekelle University, MekelleruthNo ratings yet
- Hearing LossDocument22 pagesHearing Losssimran kaurNo ratings yet
- Eye and Ears AssessmentDocument17 pagesEye and Ears AssessmentPrincess Añabeza100% (1)
- Assessing EarsDocument11 pagesAssessing EarsRhea Mae Visda RoaNo ratings yet
- FTC 106 G3Document15 pagesFTC 106 G3Ann YeongNo ratings yet
- OtosclerosisDocument9 pagesOtosclerosisSuprit SnNo ratings yet
- Hearing LossDocument9 pagesHearing Lossvicky singhNo ratings yet
- Clinical Neurology: Week 4 Lectures 7 and 8Document74 pagesClinical Neurology: Week 4 Lectures 7 and 8Miss BNo ratings yet
- Ear AssessmentDocument23 pagesEar AssessmentRotsen B. VelascoNo ratings yet
- ENT Ear I Scenarios (Compiled)Document35 pagesENT Ear I Scenarios (Compiled)rumman tariqNo ratings yet
- Anatomy and Physiology: External EarDocument73 pagesAnatomy and Physiology: External Earvidge5No ratings yet
- Lecture 2 - Audiometry PracticalDocument42 pagesLecture 2 - Audiometry PracticalSaera Hafiz Nikita100% (1)
- Aiims ENTDocument92 pagesAiims ENTSagar MukherjeeNo ratings yet
- Multiple Disability Original HandoutDocument42 pagesMultiple Disability Original HandoutHabtamu DebasuNo ratings yet
- Audiogram Interpretation Summary Slides 1 4Document31 pagesAudiogram Interpretation Summary Slides 1 4api-506629610No ratings yet
- Hearing-Impairment Case StudyDocument10 pagesHearing-Impairment Case StudyIrish Eunice Felix100% (1)
- Canalplasty For ExostosisDocument10 pagesCanalplasty For ExostosisRamya KamathNo ratings yet