Download as pdf or txt
You might also like
- Bordwell - French Impressionist CinemaDocument162 pagesBordwell - French Impressionist CinemaSimona Borcea100% (1)
- Flower ShopDocument5 pagesFlower Shopndafuma71% (7)
- Krapfl, Gasparotto - 1982 - Behavioral Systems AnalysisDocument18 pagesKrapfl, Gasparotto - 1982 - Behavioral Systems AnalysisCamila Oliveira Souza PROFESSORNo ratings yet
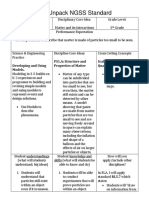
- Itl 518 Unpacking Ngss StandardDocument3 pagesItl 518 Unpacking Ngss Standardapi-432465054100% (1)
- Fast Food RestaurantsDocument47 pagesFast Food RestaurantsFares EL DeenNo ratings yet
- Jama Gussin 2024 Oi 240026 1714681236.3071Document14 pagesJama Gussin 2024 Oi 240026 1714681236.3071Ubed An'threeNo ratings yet
- Health Resource Utilization and Medical Care Cost of Acute Care Elderly Unit PatientsDocument7 pagesHealth Resource Utilization and Medical Care Cost of Acute Care Elderly Unit Patientspintoa_1No ratings yet
- Cancer Brief 090413Document8 pagesCancer Brief 090413MarianaNo ratings yet
- GN Kidney InternationalDocument8 pagesGN Kidney InternationalJessica Victoria SudanawidjajaNo ratings yet
- Burden of Serious Harms From Diagnostic Error in The USADocument12 pagesBurden of Serious Harms From Diagnostic Error in The USACBS PhiladelphiaNo ratings yet
- Cancer Warning Symptoms AwarenessDocument9 pagesCancer Warning Symptoms AwarenessAdmasu BelayNo ratings yet
- J9 How Little We Know Herpes ZosterDocument4 pagesJ9 How Little We Know Herpes ZosterNur Adha AtjoNo ratings yet
- A Toolkit For Senior Friendly Hospitals A Project of The RGP of TorontoDocument13 pagesA Toolkit For Senior Friendly Hospitals A Project of The RGP of Torontoandreas100% (2)
- 加拿大食道癌Document8 pages加拿大食道癌Joseph ChenNo ratings yet
- HHS Public Access: Readmission Diagnoses After Severe Sepsis and Other Acute Medical ConditionsDocument5 pagesHHS Public Access: Readmission Diagnoses After Severe Sepsis and Other Acute Medical ConditionsRodrigoSachiFreitasNo ratings yet
- Classifi Cation of Treatment-Related Mortality in Children WithDocument7 pagesClassifi Cation of Treatment-Related Mortality in Children WithIgnatia Rosalia KiranaNo ratings yet
- 4 Trends and Outcomes of HospitalizationsDocument7 pages4 Trends and Outcomes of HospitalizationsAnayanzy VarelaNo ratings yet
- Prevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care HospitalsDocument14 pagesPrevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care HospitalsBECERRA CACHO MIGUEL ANGELNo ratings yet
- Inouye 2007Document8 pagesInouye 2007Veridiana Assencio SilvaNo ratings yet
- Global Incidence of Frailty and Prefrailty Among Community-Dwelling Older Adults_ A Systematic Review and Meta-analysis.Document18 pagesGlobal Incidence of Frailty and Prefrailty Among Community-Dwelling Older Adults_ A Systematic Review and Meta-analysis.Alberto GómoNo ratings yet
- Research Article: The Bethesda System For Reporting Thyroid Cytopathology: A Cytohistological StudyDocument8 pagesResearch Article: The Bethesda System For Reporting Thyroid Cytopathology: A Cytohistological StudyAbdullah KhalilNo ratings yet
- 1 s2.0 S1083879120306686 MainDocument2 pages1 s2.0 S1083879120306686 MainCommon JaiswalNo ratings yet
- 10 1001jama 2016 4454Document9 pages10 1001jama 2016 4454Abdi HidayatNo ratings yet
- Healthcare Utilization Is High in Adult Patients Relapsing After Allogeneic Hematopoietic Cell TransplantationDocument7 pagesHealthcare Utilization Is High in Adult Patients Relapsing After Allogeneic Hematopoietic Cell TransplantationRafael TerceiroNo ratings yet
- Improving Medication Reconciliation at Hospital Admission, Discharge and Ambulatory Care Through A Transition of Care TeamDocument6 pagesImproving Medication Reconciliation at Hospital Admission, Discharge and Ambulatory Care Through A Transition of Care TeamRiza Yulia RezkiNo ratings yet
- Perianal Condyloma Acuminata: Factors That Contribute To The RecurrenceDocument3 pagesPerianal Condyloma Acuminata: Factors That Contribute To The RecurrencetaagrettaaNo ratings yet
- Application of Different Scoring Systems and Their Value in Pediatric Intensive Care UnitDocument6 pagesApplication of Different Scoring Systems and Their Value in Pediatric Intensive Care UnitPreksha AdeNo ratings yet
- Menopausal Hormone Therapy and The Incidence of Carpal Tunnel Syndrome in Postmenopausal Women: Findings From The Women's Health InitiativeDocument15 pagesMenopausal Hormone Therapy and The Incidence of Carpal Tunnel Syndrome in Postmenopausal Women: Findings From The Women's Health InitiativeDwiky YuanasikaNo ratings yet
- Hon-2020-How Well Do Ems Providers Predict IntDocument14 pagesHon-2020-How Well Do Ems Providers Predict IntDereje BayissaNo ratings yet
- Medi 96 E6799Document8 pagesMedi 96 E6799Utami DewiNo ratings yet
- Melanoma Incidence, Recurrence, and Mortality in An Integrated Healthcare System: A Retrospective Cohort StudyDocument9 pagesMelanoma Incidence, Recurrence, and Mortality in An Integrated Healthcare System: A Retrospective Cohort StudyPande Agung MahariskiNo ratings yet
- HospitalDocument5 pagesHospitalhinatakunhinata75No ratings yet
- Early Referral To A Palliative Team Improves End-Of-life Care Among Gynecological Cancer PatientsDocument11 pagesEarly Referral To A Palliative Team Improves End-Of-life Care Among Gynecological Cancer PatientsArmando José MaldonadoNo ratings yet
- Original Investigation: Key PointsDocument12 pagesOriginal Investigation: Key Pointsziqian weiNo ratings yet
- 2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaDocument7 pages2010 - Epidemioloy of Ulcerative Keratitis in Northern CaliforniaPrasetya AnugrahNo ratings yet
- Frailty in Emergency Departments - LancetDocument1 pageFrailty in Emergency Departments - LancetOscar David Gamarra PerezNo ratings yet
- An Investigation of The Apparent Breast Cancer Epidemic in France: Screening and Incidence Trends in Birth CohortsDocument8 pagesAn Investigation of The Apparent Breast Cancer Epidemic in France: Screening and Incidence Trends in Birth CohortscinthyalucioNo ratings yet
- Circ 113 21 E788Document47 pagesCirc 113 21 E788NICU LEVELNo ratings yet
- Owen 2013Document9 pagesOwen 2013Yacine Tarik AizelNo ratings yet
- ProfilaksisDocument4 pagesProfilaksisLatifah MaharaniNo ratings yet
- Development of The Bereavement Risk Inventory and Screening Questionnaire (BRISQ) : Item Generation and Expert Panel FeedbackDocument10 pagesDevelopment of The Bereavement Risk Inventory and Screening Questionnaire (BRISQ) : Item Generation and Expert Panel FeedbackShinta PriyanggaNo ratings yet
- Relationship: MyocardialDocument3 pagesRelationship: MyocardialSara RamirezNo ratings yet
- Trauma ThorakDocument6 pagesTrauma ThorakIndahNo ratings yet
- Compartir Geri OncoDocument4 pagesCompartir Geri OncoHenrikNo ratings yet
- Jamasurgery Shah 2018 Oi 180008Document10 pagesJamasurgery Shah 2018 Oi 180008John SmithNo ratings yet
- Aizer, Marital, Survival CancerDocument8 pagesAizer, Marital, Survival CancerFitri SetyawatiNo ratings yet
- Ournal of Linical Ncology: PurposeDocument11 pagesOurnal of Linical Ncology: PurposeRicky Cornelius TariganNo ratings yet
- Jama Quinn 2020 Oi 200087 1602283774.26341Document12 pagesJama Quinn 2020 Oi 200087 1602283774.26341charmyshkuNo ratings yet
- Comparison of Palliative Care Delivery in The Last Year of Life Between Adults With Terminal Noncancer Illness or CancerDocument13 pagesComparison of Palliative Care Delivery in The Last Year of Life Between Adults With Terminal Noncancer Illness or CancerSharif HossainNo ratings yet
- Comparaciòn News2 en Infectados Alerta Temprana de IngresoDocument12 pagesComparaciòn News2 en Infectados Alerta Temprana de IngresoFemyLealNo ratings yet
- Community Pharmacy MedicationDocument11 pagesCommunity Pharmacy MedicationVander JuniorNo ratings yet
- Tendências Na Incidência e Fatores de Risco Associados À Mortalidade Por Suicídio Entre Pacientes Com Câncer de MamaDocument7 pagesTendências Na Incidência e Fatores de Risco Associados À Mortalidade Por Suicídio Entre Pacientes Com Câncer de MamaLeonardo CarvalhoNo ratings yet
- Brain CancerDocument7 pagesBrain Cancerbanteng wibisonoNo ratings yet
- BMJ 2022 070603.fullDocument11 pagesBMJ 2022 070603.fullAnnisa Zaskia AlexandraNo ratings yet
- Crisis Intervention For People With Severe Mental IllnessesDocument2 pagesCrisis Intervention For People With Severe Mental IllnessespechyvarasNo ratings yet
- ContentserverDocument7 pagesContentserverapi-278377715No ratings yet
- Epidemiology of Vestibular Schwannoma in The United States 2004-2016Document8 pagesEpidemiology of Vestibular Schwannoma in The United States 2004-2016Indra PrimaNo ratings yet
- bellew-et-al-2016-impact-of-an-emergency-department-observation-unit-management-algorithm-for-atrial-fibrillationDocument10 pagesbellew-et-al-2016-impact-of-an-emergency-department-observation-unit-management-algorithm-for-atrial-fibrillationChoga ArlandoNo ratings yet
- Proton Pump Inhibitor Use and The Risk of Chronic Kidney DiseaseDocument9 pagesProton Pump Inhibitor Use and The Risk of Chronic Kidney DiseaseDita IndahNo ratings yet
- Phelan 2018Document16 pagesPhelan 2018Santiago MayorNo ratings yet
- Manuscript of Risk Factors For Cancer Cervix: An Analysis of 1000 CasesDocument4 pagesManuscript of Risk Factors For Cancer Cervix: An Analysis of 1000 CasesHerman FiraNo ratings yet
- Dementia and Hospital Readmission Rates: A Systematic ReviewDocument8 pagesDementia and Hospital Readmission Rates: A Systematic ReviewImam GodlyNo ratings yet
- 01 CCM 0000119424 31648 1eDocument6 pages01 CCM 0000119424 31648 1eumi far ainNo ratings yet
- Suicidal Death Within A Year of A Cancer Diagnosis A Population Based StudyDocument8 pagesSuicidal Death Within A Year of A Cancer Diagnosis A Population Based StudyLeonardo CarvalhoNo ratings yet
- Development of an Electronic Frailty Index for Hospitalized Older Adults in SwedenDocument9 pagesDevelopment of an Electronic Frailty Index for Hospitalized Older Adults in SwedencharmyshkuNo ratings yet
- Cramon-2021-Individual-nutritional-interventionDocument13 pagesCramon-2021-Individual-nutritional-interventioncharmyshkuNo ratings yet
- Effectiveness and Cost-Effectiveness of Home Palliative Care Services For Adults With Advanced Illness and Their CaregiversDocument232 pagesEffectiveness and Cost-Effectiveness of Home Palliative Care Services For Adults With Advanced Illness and Their CaregiverscharmyshkuNo ratings yet
- A multidimensional approach to frailty in older peopleDocument20 pagesA multidimensional approach to frailty in older peoplecharmyshkuNo ratings yet
- 10.1002@sici1097-02581998101517@192265@@aid-sim9183.0.co2-bDocument17 pages10.1002@sici1097-02581998101517@192265@@aid-sim9183.0.co2-bcharmyshkuNo ratings yet
- Statistics in Medicine - 2023 - Ségalas - Propensity score matching after multiple imputation when a confounder has missingDocument14 pagesStatistics in Medicine - 2023 - Ségalas - Propensity score matching after multiple imputation when a confounder has missingcharmyshkuNo ratings yet
- JHKGS9612 P 009Document5 pagesJHKGS9612 P 009charmyshkuNo ratings yet
- Effects of Facilitated Family Case Conferencing For Advanced Dementia - A Cluster Randomised Clinical Trial.Document16 pagesEffects of Facilitated Family Case Conferencing For Advanced Dementia - A Cluster Randomised Clinical Trial.charmyshkuNo ratings yet
- jamaotolaryngology_sawaf_2023_oi_230010_1685130136.11146Document8 pagesjamaotolaryngology_sawaf_2023_oi_230010_1685130136.11146charmyshkuNo ratings yet
- Effects of A Transitional Palliative Care Model On Patients With End-Stage Heart Failure - A Randomised Controlled TrialDocument9 pagesEffects of A Transitional Palliative Care Model On Patients With End-Stage Heart Failure - A Randomised Controlled TrialcharmyshkuNo ratings yet
- Kaasalainen 2020 Current Issues With Implementing A Palliative Approach in Long Term Care Where Do We Go From HereDocument3 pagesKaasalainen 2020 Current Issues With Implementing A Palliative Approach in Long Term Care Where Do We Go From HerecharmyshkuNo ratings yet
- SERIOUS ILLNESS COMMUNICATION PROJECT - ProtocolDocument142 pagesSERIOUS ILLNESS COMMUNICATION PROJECT - ProtocolcharmyshkuNo ratings yet
- EAPC White Paper On Outcome MeasurementDocument17 pagesEAPC White Paper On Outcome MeasurementcharmyshkuNo ratings yet
- s12904 021 00847 7Document9 pagess12904 021 00847 7charmyshkuNo ratings yet
- Using Palliative Leaders in Facilities To Transform Care For People With Alzheimer's Disease (UPLIFT-AD) - Protocol of A Palliative Care Clinical Trial in Nursing HomesDocument10 pagesUsing Palliative Leaders in Facilities To Transform Care For People With Alzheimer's Disease (UPLIFT-AD) - Protocol of A Palliative Care Clinical Trial in Nursing HomescharmyshkuNo ratings yet
- The Effects of Advance Care Planning Intervention On Nursing Home Residents - A Systematic Review and Meta-Analysis of Randomised Controlled TrialsDocument10 pagesThe Effects of Advance Care Planning Intervention On Nursing Home Residents - A Systematic Review and Meta-Analysis of Randomised Controlled TrialscharmyshkuNo ratings yet
- Improved Quality of Death and Dying in Care Homes - A Palliative Care Stepped Wedge Randomized Control Trial in AustraliaDocument8 pagesImproved Quality of Death and Dying in Care Homes - A Palliative Care Stepped Wedge Randomized Control Trial in AustraliacharmyshkuNo ratings yet
- The Use of The PARIHS Framework in Implementation Research and PracticeDocument51 pagesThe Use of The PARIHS Framework in Implementation Research and PracticecharmyshkuNo ratings yet
- The RESOLVE PCOM Implementation StrategyDocument9 pagesThe RESOLVE PCOM Implementation StrategycharmyshkuNo ratings yet
- An Electronic Adherence Measurement Intervention To Reduce Clinical Inertia in The Treatment of Uncontrolled Hypertension - The MATCH Cluster Randomized Clinical TrialDocument7 pagesAn Electronic Adherence Measurement Intervention To Reduce Clinical Inertia in The Treatment of Uncontrolled Hypertension - The MATCH Cluster Randomized Clinical TrialcharmyshkuNo ratings yet
- The Impact of Need-Based Care On Formal Caregivers' Wellbeing in Nursing Homes - A Cluster Randomized Controlled TrialDocument10 pagesThe Impact of Need-Based Care On Formal Caregivers' Wellbeing in Nursing Homes - A Cluster Randomized Controlled TrialcharmyshkuNo ratings yet
- Boogaard Et Al 2018 Effects of Two Feedback Interventions On End of Life Outcomes in Nursing Home Residents WithDocument10 pagesBoogaard Et Al 2018 Effects of Two Feedback Interventions On End of Life Outcomes in Nursing Home Residents WithcharmyshkuNo ratings yet
- Improved Quality of Death and Dying in Care Homes - A Palliative Care Stepped Wedge Randomized Control Trial in Australia (Protocal)Document34 pagesImproved Quality of Death and Dying in Care Homes - A Palliative Care Stepped Wedge Randomized Control Trial in Australia (Protocal)charmyshkuNo ratings yet
- 2020, JCO - disseminationandImplementationofPalliative CareinOncologyDocument8 pages2020, JCO - disseminationandImplementationofPalliative CareinOncologycharmyshkuNo ratings yet
- Impact of Nursing Home Palliative Care Teams On End-of-Life Outcomes - A Randomized Controlled TrialDocument8 pagesImpact of Nursing Home Palliative Care Teams On End-of-Life Outcomes - A Randomized Controlled TrialcharmyshkuNo ratings yet
- Adherence To Key Recommendations For Design and Analysis of Stepped-Wedge Cluster Randomized Trials - A Review of Trials Published 2016-2022Document12 pagesAdherence To Key Recommendations For Design and Analysis of Stepped-Wedge Cluster Randomized Trials - A Review of Trials Published 2016-2022charmyshkuNo ratings yet
- (2023) JAMDATiming of Goals of Care Discussions in Nursing Homes - A Systematic ReviewDocument11 pages(2023) JAMDATiming of Goals of Care Discussions in Nursing Homes - A Systematic ReviewcharmyshkuNo ratings yet
- 2004 - GREENHALGH - Diffusion of Innovations in Service Organizations Systematic Review andDocument49 pages2004 - GREENHALGH - Diffusion of Innovations in Service Organizations Systematic Review andcharmyshkuNo ratings yet
- Lesson 1 1 1Document21 pagesLesson 1 1 1kiyorokiiNo ratings yet
- Big Data in Human Resources - Talent Analytics (People Analytics) Comes of Age PDFDocument6 pagesBig Data in Human Resources - Talent Analytics (People Analytics) Comes of Age PDFmatias_moroni_1No ratings yet
- February CADocument71 pagesFebruary CAHit SuccessNo ratings yet
- A Review Analytical Quality Control and Methodology in Internal Quality Control of Chemical AnalysisDocument9 pagesA Review Analytical Quality Control and Methodology in Internal Quality Control of Chemical AnalysisResearch ParkNo ratings yet
- Developmental Stages in Middle and Late AdolescenceDocument19 pagesDevelopmental Stages in Middle and Late AdolescenceHalley SuingNo ratings yet
- HA Convention Opening SpeechDocument8 pagesHA Convention Opening SpeechwakakaNo ratings yet
- Supply Chain Management in Construction and Engineer-To-Order IndustriesDocument9 pagesSupply Chain Management in Construction and Engineer-To-Order IndustriesMuhammad ShoaibNo ratings yet
- Discounts and Warranties As Factors of Product MarketabilityDocument11 pagesDiscounts and Warranties As Factors of Product MarketabilityMarjorie Joyce BarituaNo ratings yet
- Vocatives in Nkengasong'S Black Caps and Red Feathers and Achebe'SDocument17 pagesVocatives in Nkengasong'S Black Caps and Red Feathers and Achebe'SWalter yepdiaNo ratings yet
- DISS Module 1Document8 pagesDISS Module 1Rheamae LaoNo ratings yet
- CASE - Larsson Kolb Dialysis 2016Document2 pagesCASE - Larsson Kolb Dialysis 2016Paarth SonwaneyNo ratings yet
- Surveying RTP MODDocument106 pagesSurveying RTP MODPrakash Kumar KumarNo ratings yet
- Business Research: Part A: Question 1Document17 pagesBusiness Research: Part A: Question 1akyregisterNo ratings yet
- The Development of ICF Core Sets For Autism Spectrum DisorderDocument6 pagesThe Development of ICF Core Sets For Autism Spectrum Disorderlinm@kilvington.vic.edu.auNo ratings yet
- Edgar Allan Poe UnitDocument7 pagesEdgar Allan Poe Unitapi-272831096No ratings yet
- 19680-Article Text-71593-1-6-20220815Document7 pages19680-Article Text-71593-1-6-20220815iffah19ahmadNo ratings yet
- The Prototypicality of BrandsDocument9 pagesThe Prototypicality of Brandsranjann349No ratings yet
- Education Sciences: Parental Involvement During Pandemic Times: Challenges and OpportunitiesDocument17 pagesEducation Sciences: Parental Involvement During Pandemic Times: Challenges and OpportunitiesJanine CanlasNo ratings yet
- Science in The Preschool ClassroomDocument7 pagesScience in The Preschool ClassroomDwina AlaphiaNo ratings yet
- Majority QFRs Raimondo Part 2Document36 pagesMajority QFRs Raimondo Part 2NBC 10 WJARNo ratings yet
- Beaeka General Business PLC Exploration Work Programme For CoalDocument38 pagesBeaeka General Business PLC Exploration Work Programme For CoalGeta EjiguNo ratings yet
- CH 2Document13 pagesCH 2Ebsa AdemeNo ratings yet
- Quarter 1Document141 pagesQuarter 1Gerry Areola AquinoNo ratings yet
- Jurnal Teori Pertukaran SosialDocument11 pagesJurnal Teori Pertukaran SosialRhama PutraNo ratings yet
- Factors Affecting The Utilization of Library Resources AmongDocument14 pagesFactors Affecting The Utilization of Library Resources AmongOlive Therese100% (1)