Download as pdf or txt
You might also like
- All Paeds Online Variants CompiledDocument103 pagesAll Paeds Online Variants CompiledNektarios TsakalosNo ratings yet
- 5 - Diagnostic Approach of DyspneaDocument30 pages5 - Diagnostic Approach of Dyspneaivan halimNo ratings yet
- Asma Dan COPDDocument52 pagesAsma Dan COPDErik II100% (1)
- The Cerebral Arterio-Venous Malformations Radiological PortrayalDocument4 pagesThe Cerebral Arterio-Venous Malformations Radiological PortrayalBRNSS Publication Hub InfoNo ratings yet
- Cerebral Venous Thrombosis: A Practical GuideDocument12 pagesCerebral Venous Thrombosis: A Practical Guidedanby danbyNo ratings yet
- Patterns of Ischemic Posterior Circulation Strokes: A Clinical, Anatomical, and Radiological ReviewDocument9 pagesPatterns of Ischemic Posterior Circulation Strokes: A Clinical, Anatomical, and Radiological ReviewsamuelNo ratings yet
- Causes of Stroke PDFDocument16 pagesCauses of Stroke PDFEmmanuel AguilarNo ratings yet
- Cerebral Venous Thrombosis PDFDocument12 pagesCerebral Venous Thrombosis PDFBirrie DeresseNo ratings yet
- Heart Disease IXDocument5 pagesHeart Disease IXJOUBERT ALVAREZ100% (1)
- AL. 1 Enfermedad CV Ateroesclerã Tica Figura 1Document5 pagesAL. 1 Enfermedad CV Ateroesclerã Tica Figura 1Carol Mata BarreraNo ratings yet
- Diagnostics 13 00447 v4Document20 pagesDiagnostics 13 00447 v4RanitaNo ratings yet
- Distribution Territories and Causative Mechanisms of Ischemic StrokeDocument11 pagesDistribution Territories and Causative Mechanisms of Ischemic StrokeMatheus Nucci RiccettoNo ratings yet
- Distribution Territories and Causative MechanismsDocument12 pagesDistribution Territories and Causative MechanismsIkhsan FebriansyahNo ratings yet
- Ging of Acute Ischemic Stroke: Marwan El-Koussy, Gerhard Schroth, Caspar Brekenfeld, Marcel ArnoldDocument23 pagesGing of Acute Ischemic Stroke: Marwan El-Koussy, Gerhard Schroth, Caspar Brekenfeld, Marcel ArnoldAnonymous iea4m0ZRNo ratings yet
- Doppler Transcreaneal y Ecografía Del Nervio ÓpticoDocument15 pagesDoppler Transcreaneal y Ecografía Del Nervio ÓpticoBenjamínGalvanNo ratings yet
- Hemodinamika SSSDocument12 pagesHemodinamika SSSEmir BegagićNo ratings yet
- Diagnostics 12 00258 v2Document20 pagesDiagnostics 12 00258 v2Sara GaoNo ratings yet
- Byrne, CT Imaging of Acute Ischemic StrokeDocument15 pagesByrne, CT Imaging of Acute Ischemic StrokeririsNo ratings yet
- Vasculopatias SNCDocument16 pagesVasculopatias SNCGonçalo CabralNo ratings yet
- Photoacoustic Imaging For Monitoring of Stroke Diseases A Review Yang2021Document16 pagesPhotoacoustic Imaging For Monitoring of Stroke Diseases A Review Yang2021Elizabeth EspitiaNo ratings yet
- s40140 021 00483 0 PDFDocument9 pagess40140 021 00483 0 PDFanisakhildaNo ratings yet
- 1 s2.0 S0303846722002499 MainDocument17 pages1 s2.0 S0303846722002499 MainEva HikmahNo ratings yet
- Angina MicrovasvularDocument8 pagesAngina MicrovasvularLex X PabloNo ratings yet
- Management of Cardiogenic Shock After Acute - 2023Document10 pagesManagement of Cardiogenic Shock After Acute - 2023Angy KarakostaNo ratings yet
- Imaging of Cerebral Ischemic Edema and Neuronal DeathDocument9 pagesImaging of Cerebral Ischemic Edema and Neuronal Deathgwyneth.green.512No ratings yet
- Stable Angina MV SBDocument11 pagesStable Angina MV SBAndi NamirahNo ratings yet
- 2022-Coronary Flow Assessment Using 3D Ultrafast Ultrasound Localization MicrosDocument16 pages2022-Coronary Flow Assessment Using 3D Ultrafast Ultrasound Localization MicrosWeicen ChenNo ratings yet
- 2020 Evc Isquemico Localizacion ClinicaDocument19 pages2020 Evc Isquemico Localizacion ClinicaJuan Pablo B. FloresNo ratings yet
- Wa0033.Document20 pagesWa0033.dyegoutNo ratings yet
- CT For Treatment Selection in Acute Ischemic Stroke: A Code Stroke PrimerDocument22 pagesCT For Treatment Selection in Acute Ischemic Stroke: A Code Stroke PrimerSantiago TapiaNo ratings yet
- Neurological and Head and Neck Menifestations of Sickle Cell DiseaseDocument20 pagesNeurological and Head and Neck Menifestations of Sickle Cell Disease1.thekey.1No ratings yet
- Imaging of Cerebellopontine Angle Lesions: An Update. Part 1: Enhancing Extra-Axial LesionsDocument11 pagesImaging of Cerebellopontine Angle Lesions: An Update. Part 1: Enhancing Extra-Axial LesionsKhương Hà NguyễnNo ratings yet
- Coronary Computed Tomographic Angiography Studies A Brief Review in Analysis Interpretation and 9711Document4 pagesCoronary Computed Tomographic Angiography Studies A Brief Review in Analysis Interpretation and 9711Redhwan Abdullah qaid AlshubiNo ratings yet
- Nuclear Cardiology: Role in The World of Multimodality Cardiac ImagingDocument5 pagesNuclear Cardiology: Role in The World of Multimodality Cardiac ImagingElena FlorentinaNo ratings yet
- Reversible Vasoconstriction SyndromeDocument16 pagesReversible Vasoconstriction SyndromeAnonymous ZUaUz1wwNo ratings yet
- Diasquisis L PDFDocument5 pagesDiasquisis L PDFValentina Sanhueza Gatica100% (1)
- Jurnal Reading: Imaging in Acute StrokeDocument30 pagesJurnal Reading: Imaging in Acute StrokeBejo LanangNo ratings yet
- Cerebral Autoregulation in Subarachnoid HemorrhageDocument29 pagesCerebral Autoregulation in Subarachnoid HemorrhageAnonymous QLadTClydkNo ratings yet
- Intracranial CystsDocument9 pagesIntracranial CystsjosephNo ratings yet
- Fmedt 04 748949Document12 pagesFmedt 04 748949Orlin ZlatarskiNo ratings yet
- Vasculopathy and Vasculitis: 7.1 Defi Nition 7.4 Vasculitis of The CNSDocument2 pagesVasculopathy and Vasculitis: 7.1 Defi Nition 7.4 Vasculitis of The CNSPhạm Hữu ThườngNo ratings yet
- SVN 2019 000305Document10 pagesSVN 2019 000305zak sutomoNo ratings yet
- Acute and Episodic Vestibular Syndromes Caused by Ischemic Stroke: Predilection Sites and Risk FactorsDocument12 pagesAcute and Episodic Vestibular Syndromes Caused by Ischemic Stroke: Predilection Sites and Risk FactorsKarl Martin PinedaNo ratings yet
- 33 IjecsDocument6 pages33 IjecsSURAJIT DUTTANo ratings yet
- Biomedicines 10 02830 v2Document12 pagesBiomedicines 10 02830 v2Septi Dimas jamaludinNo ratings yet
- Acute StrokeDocument12 pagesAcute StrokeAnonymous 0ymhODNo ratings yet
- Demensia Vaskuler 2Document20 pagesDemensia Vaskuler 2Adam MochtarNo ratings yet
- Cerebral Venous Thrombosis - A Comprehensive ReviewDocument11 pagesCerebral Venous Thrombosis - A Comprehensive ReviewAdmin neuro-usu.idNo ratings yet
- Multimodality Cardiac Imaging of A Ventricular SepDocument4 pagesMultimodality Cardiac Imaging of A Ventricular SephengkileonardNo ratings yet
- Pacing Clinical Electrophis - 2022 - MartiniDocument10 pagesPacing Clinical Electrophis - 2022 - MartiniRobertoNo ratings yet
- Seitz A. Update On Coronary Artery Spasm 2022 - A Narrative Review. International Journal of CardiologyDocument6 pagesSeitz A. Update On Coronary Artery Spasm 2022 - A Narrative Review. International Journal of CardiologyDaniel MoralesNo ratings yet
- Management of Acute Ischemic Stroke: Michael S Phipps, Carolyn A CroninDocument15 pagesManagement of Acute Ischemic Stroke: Michael S Phipps, Carolyn A CroninPatty MArivel ReinosoNo ratings yet
- RM en Estenosis y Regurgitación Aortica. J Cardiovasc Dev Dis 2022Document15 pagesRM en Estenosis y Regurgitación Aortica. J Cardiovasc Dev Dis 2022Ernesto J. Rocha ReyesNo ratings yet
- The Cerebral Circulation and Cerebrovascular Disease II Pathogenesis of Cerebrovascular DiseaseDocument9 pagesThe Cerebral Circulation and Cerebrovascular Disease II Pathogenesis of Cerebrovascular DiseaseLAURA ALEJANDRA GALVIS QUINTERONo ratings yet
- Cerebrovascular DiseaseDocument3 pagesCerebrovascular DiseaseLourdes VillelaNo ratings yet
- A System Based' Approach To Risk Assessment of The Cervical Spine Prior ToDocument9 pagesA System Based' Approach To Risk Assessment of The Cervical Spine Prior ToRudolfGerNo ratings yet
- Diagnosing STEMI in Right Then Left Bundle Branch Block Pattern Ventricular Escape Rhythm (Case Report) - Oxford Medical Case Report 2022 - 2Document4 pagesDiagnosing STEMI in Right Then Left Bundle Branch Block Pattern Ventricular Escape Rhythm (Case Report) - Oxford Medical Case Report 2022 - 2Dolly JazmiNo ratings yet
- J Permed 2012 03 002Document4 pagesJ Permed 2012 03 002Mariano DomanicoNo ratings yet
- The Clinical Features and Differential Diagnosis of Acute StrokeDocument19 pagesThe Clinical Features and Differential Diagnosis of Acute StrokeGiorgianaNo ratings yet
- Small Vessel Disease in The Heart and Brain Berry (2019) ##Document16 pagesSmall Vessel Disease in The Heart and Brain Berry (2019) ##Jim BeamNo ratings yet
- Coronary Vasomotion AbnormalitiesFrom EverandCoronary Vasomotion AbnormalitiesHiroaki ShimokawaNo ratings yet
- Cavernomas of the CNS: Basic Science to Clinical PracticeFrom EverandCavernomas of the CNS: Basic Science to Clinical PracticeOndřej BradáčNo ratings yet
- Microcirculation: From Bench to BedsideFrom EverandMicrocirculation: From Bench to BedsideMaria DorobantuNo ratings yet
- THT Bimbel Ukdi Mantap 2015 - NorestrictionDocument227 pagesTHT Bimbel Ukdi Mantap 2015 - NorestrictionpanduNo ratings yet
- Embryology of Urinary SystemDocument4 pagesEmbryology of Urinary SystemZllison Mae Teodoro MangabatNo ratings yet
- Neuroscience FK UPH 2014: Multiple Choice QuestionsDocument33 pagesNeuroscience FK UPH 2014: Multiple Choice QuestionsSanzuiNo ratings yet
- Pain ManagementDocument162 pagesPain ManagementFASIKAW GIZAWNo ratings yet
- CTCAEDocument72 pagesCTCAEArun NairNo ratings yet
- What Is Pleural Effusion?: Chest X-RayDocument6 pagesWhat Is Pleural Effusion?: Chest X-RayVinceNo ratings yet
- Shouming Sun Thesis 09062020 - WyanDocument103 pagesShouming Sun Thesis 09062020 - WyanwdwdNo ratings yet
- Cow's Milk Protein AllergyDocument7 pagesCow's Milk Protein Allergy6130015013 MOCHAMMAD SULUNG NOVIYANTO SKMNo ratings yet
- 1437 - Ichd III Beta Cephalalgia Issue 9 2013Document187 pages1437 - Ichd III Beta Cephalalgia Issue 9 2013kiki melindaNo ratings yet
- Long COVID or post-COVID-19 Syndrome Putative Pathophysiology, Risk FactorsDocument18 pagesLong COVID or post-COVID-19 Syndrome Putative Pathophysiology, Risk FactorsVane SchulzeNo ratings yet
- Abruptio PlacentaDocument29 pagesAbruptio PlacentaAudrey DelfinNo ratings yet
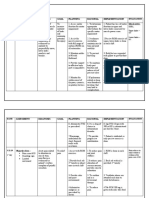
- Nursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataDocument8 pagesNursing Care Plan: Assessment Diagnosis Goal Planning Rational Implementation Objective DataMoonNo ratings yet
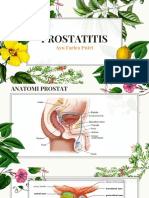
- PROSTATITIS (Tentiran Dr. Rinto)Document34 pagesPROSTATITIS (Tentiran Dr. Rinto)Anonymous kkogwa9CjNo ratings yet
- Dr. Samir - Paediatric SpineDocument33 pagesDr. Samir - Paediatric SpinelertegimluNo ratings yet
- Oral - Medicine Book ListDocument334 pagesOral - Medicine Book ListSrinivas HarikrishnanNo ratings yet
- 544179LC PDFDocument8 pages544179LC PDFJude Aldo PaulNo ratings yet
- Vitiligo A Review 2020 PDFDocument22 pagesVitiligo A Review 2020 PDFhannah khumairahNo ratings yet
- Hipertrofi Cardiomiopathy.2020.08.045Document82 pagesHipertrofi Cardiomiopathy.2020.08.045Ghina NinditasariNo ratings yet
- Quizlet Hygienist ComputerDocument5 pagesQuizlet Hygienist ComputerCamila FreitasNo ratings yet
- Metabolic Acidosis - Alkalosis Study GuideDocument1 pageMetabolic Acidosis - Alkalosis Study GuideJe KirsteneNo ratings yet
- Diuretics Pharmacology 79 88Document6 pagesDiuretics Pharmacology 79 88Neha RoyNo ratings yet
- By Sana Asif Siddiqui Instructor PsychiatryDocument22 pagesBy Sana Asif Siddiqui Instructor PsychiatrySaman HamidNo ratings yet
- Magnesium Chloride Hex A Hydrate TherapyDocument2 pagesMagnesium Chloride Hex A Hydrate TherapyDora L. Gutierrez100% (1)
- Antiadrenergic DrugsDocument44 pagesAntiadrenergic DrugsHUZAIFA YAMAANNo ratings yet
- Fabry DiseaseDocument63 pagesFabry DiseaseKunal PaulNo ratings yet
- CommentsDocument1 pageCommentsHACK WITH PKNo ratings yet
- Enarm Casos Clinicos en Ingles PDFDocument101 pagesEnarm Casos Clinicos en Ingles PDFLuis Angel Amezcua100% (1)