
Chlamydia in Koalas
Chlamydia in Koalas
You might also like
- Gipsy Oracle Cards MeaningsDocument4 pagesGipsy Oracle Cards MeaningsFidel H. Viegas92% (12)
- SGOTDocument2 pagesSGOTDinesh Sreedharan0% (1)
- Chapter 012Document11 pagesChapter 012api-2813400240% (1)
- Caso Clínico - Chlamydia TrachomatisDocument4 pagesCaso Clínico - Chlamydia TrachomatisRigobertoNo ratings yet
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDocument7 pagesScabies and Pediculosis Pubis: An Update of Treatment Regimens and General Reviewsuryanto_malvinNo ratings yet
- GlandersDocument7 pagesGlandersRyan ChenNo ratings yet
- NocardiaDocument3 pagesNocardiasujithas0% (1)
- Miscellaneous Bacterial InfectionsDocument15 pagesMiscellaneous Bacterial InfectionsHumera Gull JunejoNo ratings yet
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDocument7 pagesScabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewNovita WulandariNo ratings yet
- Cestosis y Cestodos PDFDocument14 pagesCestosis y Cestodos PDFErnesto VersailleNo ratings yet
- Cryptococcal Lung MycosesDocument14 pagesCryptococcal Lung MycosesFebri Dwi HaryonoNo ratings yet
- Glanders: C H A P T E R 2 - 5 - 1 1Document10 pagesGlanders: C H A P T E R 2 - 5 - 1 1Ryan ChenNo ratings yet
- Diagnosis, Prevention, and Treatment of ScabiesDocument5 pagesDiagnosis, Prevention, and Treatment of ScabiesSince Ivanna RumbiakNo ratings yet
- Micp ReviewerDocument30 pagesMicp ReviewerFrancisca NairNo ratings yet
- Leprosy: An Overview of Pathophysiology: Disusun OlehDocument22 pagesLeprosy: An Overview of Pathophysiology: Disusun OlehDwi Endra Juli PraditoNo ratings yet
- Clinical Avian Nutrition Excerpt PDFDocument22 pagesClinical Avian Nutrition Excerpt PDFAlejandraNo ratings yet
- Clostridial infections-LR3Document8 pagesClostridial infections-LR3yomifNo ratings yet
- Ecthyma Contagiosum (Human Orf)Document2 pagesEcthyma Contagiosum (Human Orf)Deba P SarmaNo ratings yet
- Assignment Hdb10503 Basic MicrobiologyDocument4 pagesAssignment Hdb10503 Basic MicrobiologyNida RidzuanNo ratings yet
- Diagnosis of Leishmaniasis: Review ArticleDocument12 pagesDiagnosis of Leishmaniasis: Review ArticleTUfoodbiotech groupNo ratings yet
- 37-54 Salmonella in CalvesDocument18 pages37-54 Salmonella in CalvesAna OspinaNo ratings yet
- Klebsiella Pneumoniae Pathogenesis: Etiology/BacteriologyDocument4 pagesKlebsiella Pneumoniae Pathogenesis: Etiology/Bacteriologysuper cute100% (1)
- Retrospective Study of Feline and Canine Cryptococcosis in Australia From 1981 To 2001: 195 CasesDocument12 pagesRetrospective Study of Feline and Canine Cryptococcosis in Australia From 1981 To 2001: 195 CasesKlaus Ramirez SuarezNo ratings yet
- Tugas Kukel WulanDocument15 pagesTugas Kukel WulanDonny Ardika NovanandaNo ratings yet
- Clinical Microbiology Reviews-1998-Podschun-589.fullDocument15 pagesClinical Microbiology Reviews-1998-Podschun-589.fullDorin SaulescuNo ratings yet
- StrongyloidiasisDocument5 pagesStrongyloidiasisMufidah OthmanNo ratings yet
- ChlamydiaDocument13 pagesChlamydiaTitus MutwiriNo ratings yet
- Prospective Study in A Porcine Model of Sarcoptes Scabiei Indicates The Association of Th2 and Th17 Pathways With The Clinical Severity of ScabiesDocument17 pagesProspective Study in A Porcine Model of Sarcoptes Scabiei Indicates The Association of Th2 and Th17 Pathways With The Clinical Severity of ScabiespunyayaNo ratings yet
- Scabies: Signs and SymptomsDocument5 pagesScabies: Signs and Symptomsputri intanNo ratings yet
- L1 - Actinomyces and NocardiaDocument45 pagesL1 - Actinomyces and Nocardiadvph2fck6qNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document38 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- Cryptococcosis ManualDocument3 pagesCryptococcosis Manualnassem54No ratings yet
- Common Intestinal ParasitesDocument16 pagesCommon Intestinal ParasitesbaliuwNo ratings yet
- Nocardia, Bordetella, HaemophilusDocument31 pagesNocardia, Bordetella, HaemophilusLourdes Cumagon BasiuangNo ratings yet
- Avsah v9 Id1091Document4 pagesAvsah v9 Id1091Azeneth CarolinaNo ratings yet
- Hookworm: Ancylostoma Duodenale and Necator AmericanusDocument18 pagesHookworm: Ancylostoma Duodenale and Necator AmericanusPutri AmandaNo ratings yet
- Chapter 56Document57 pagesChapter 56Rahmat MuliaNo ratings yet
- Document 3Document3 pagesDocument 3theresia 102018040No ratings yet
- Jurnal OM 2Document6 pagesJurnal OM 2Reiza PrabandanaNo ratings yet
- Lecture Rickettsia Chlamydia, MycoplasmaDocument49 pagesLecture Rickettsia Chlamydia, MycoplasmaHabeeb Ali Baig100% (3)
- Microbiology Assignment Malaria Group1Document19 pagesMicrobiology Assignment Malaria Group1wallacec1017No ratings yet
- ASCARIASISDocument13 pagesASCARIASISSandra MichelleNo ratings yet
- Pink Pigtail in A Skin Biopsy: ScabiesDocument12 pagesPink Pigtail in A Skin Biopsy: ScabiesDeba P SarmaNo ratings yet
- An Introduction of MalariaDocument19 pagesAn Introduction of MalariaSomesh GuptaNo ratings yet
- ChlamydiaDocument22 pagesChlamydiadelia rahmaNo ratings yet
- Diseases: Infected With Scabies Again? Focus in Management in Long-Term Care FacilitiesDocument12 pagesDiseases: Infected With Scabies Again? Focus in Management in Long-Term Care FacilitiesGede AdiNo ratings yet
- Papular UrticariaDocument10 pagesPapular UrticariaNuri Sakina SuhartoNo ratings yet
- Immunoproteomic Approach To Elucidating The Pathogenesis of Cryptococcosis Caused by Cryptococcus GattiiDocument10 pagesImmunoproteomic Approach To Elucidating The Pathogenesis of Cryptococcosis Caused by Cryptococcus GattiiGabriella FreitasNo ratings yet
- Naegleria FowleriDocument14 pagesNaegleria FowleriAya AyaNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document36 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- Coexistence of Cutaneous Tuberculosis (Scrofuloderma) and Hanseniasis-A Rare PresentationDocument2 pagesCoexistence of Cutaneous Tuberculosis (Scrofuloderma) and Hanseniasis-A Rare PresentationGesza Utama PutraNo ratings yet
- Proceedings of The 34th World Small Animal Veterinary Congress WSAVA 2009Document4 pagesProceedings of The 34th World Small Animal Veterinary Congress WSAVA 2009Fitri HeartNo ratings yet
- Unknown: Pink Pigtail in A Skin Biopsy: What Is Your Diagnosis?Document3 pagesUnknown: Pink Pigtail in A Skin Biopsy: What Is Your Diagnosis?Deba P SarmaNo ratings yet
- Disease Caused by ProtozoansDocument21 pagesDisease Caused by ProtozoansBrijesh KumarNo ratings yet
- Cell Structure of Cryptococcus FungiDocument19 pagesCell Structure of Cryptococcus FungiArshjyoti SinghNo ratings yet
- Hookworm Infection - UpToDateDocument12 pagesHookworm Infection - UpToDatedesilasarybasriNo ratings yet
- Scabies Mites Alter The Skin Microbiome and PromoteDocument13 pagesScabies Mites Alter The Skin Microbiome and Promotemohammed bouchibaNo ratings yet
- Chapter 62 The Yeasts and Yeastlike OrganismsDocument33 pagesChapter 62 The Yeasts and Yeastlike OrganismsbartsnewNo ratings yet
- Groupone MycologyDocument14 pagesGroupone MycologyTilahun TesemaNo ratings yet
- Overview of Infectious Coryza in Chickens: Veterinary ManualDocument4 pagesOverview of Infectious Coryza in Chickens: Veterinary ManualSamapanNo ratings yet
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- Ilham Maulana CVDocument3 pagesIlham Maulana CVYusran FachryNo ratings yet
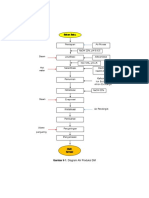
- Gambar 6 1. Diagram Alir Produksi DMDocument3 pagesGambar 6 1. Diagram Alir Produksi DMYusran FachryNo ratings yet
- 1.4 Product Distribution: Table 1.5 Percentage Distribution To 5 AreaDocument3 pages1.4 Product Distribution: Table 1.5 Percentage Distribution To 5 AreaYusran FachryNo ratings yet
- Tk22 Revised Midterm ReportDocument85 pagesTk22 Revised Midterm ReportYusran FachryNo ratings yet
- Insulation in LNG Storage and PipingDocument55 pagesInsulation in LNG Storage and PipingYusran FachryNo ratings yet
- Chemistry of Methyl Ester SulfonatesDocument8 pagesChemistry of Methyl Ester SulfonatesYusran FachryNo ratings yet
- TK11 Outline Assignment1 PDFDocument2 pagesTK11 Outline Assignment1 PDFYusran FachryNo ratings yet
- TK11 Outline Assignment1Document2 pagesTK11 Outline Assignment1Yusran FachryNo ratings yet
- 4horsemen PDFDocument2 pages4horsemen PDFYusran FachryNo ratings yet
- The 2 Covid-19 Wave in South Africa: Transmissibility & A 501.V2 VariantDocument12 pagesThe 2 Covid-19 Wave in South Africa: Transmissibility & A 501.V2 VariantBathandwa Malingo100% (6)
- Airway Assessment and ManagementDocument32 pagesAirway Assessment and ManagementAbishek NewbeginNo ratings yet
- Shaws-Textbook-Of-Gynaecology-17 487Document1 pageShaws-Textbook-Of-Gynaecology-17 487imran khanNo ratings yet
- 01 NGT Procedure With RationaleDocument4 pages01 NGT Procedure With RationaleAryaj SulitNo ratings yet
- Fix MAPPING AQSHA 3 SELASA, 09 NOVEMBER 2021Document10 pagesFix MAPPING AQSHA 3 SELASA, 09 NOVEMBER 2021Febbby Mutia SafiraNo ratings yet
- Ashton ManualDocument100 pagesAshton ManualAndrei BombardieruNo ratings yet
- Burkhart CVDocument6 pagesBurkhart CVapi-535300613No ratings yet
- S1 2021 409100 BibliographyDocument16 pagesS1 2021 409100 Bibliographyberliana PutriNo ratings yet
- Toxic Effects, Drug CalculationDocument185 pagesToxic Effects, Drug CalculationAntonette Africa MercadoNo ratings yet
- 14 Drug StudyDocument15 pages14 Drug StudyTricia AlvarezNo ratings yet
- PASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceDocument2 pagesPASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceJhigo Villar Franco PascualNo ratings yet
- Take Away 2 - Airbus Hazard Prevention Handbook (Distribution Copy)Document41 pagesTake Away 2 - Airbus Hazard Prevention Handbook (Distribution Copy)UbernatorNo ratings yet
- Prevalence of Nematode Contracaecum and Cestode Ligula Intestinalis Parasites Infection in Two Fish Species at Lake TanaDocument8 pagesPrevalence of Nematode Contracaecum and Cestode Ligula Intestinalis Parasites Infection in Two Fish Species at Lake TanaIJARP PublicationsNo ratings yet
- Drug Study GuideDocument2 pagesDrug Study GuideAubrey SungaNo ratings yet
- 2020 Chapter Lung Cancer and Tobacco Smoking FinalDocument21 pages2020 Chapter Lung Cancer and Tobacco Smoking FinalMarco MerazNo ratings yet
- A Guide For Grandparents of Children With CancerDocument24 pagesA Guide For Grandparents of Children With CancerVanessa SilvaNo ratings yet
- Medical Mnemonics 4 PrintDocument65 pagesMedical Mnemonics 4 Printanne0521100% (1)
- Topic 3 Module 1 and 2 CombinedDocument24 pagesTopic 3 Module 1 and 2 CombinedPortia NothobileNo ratings yet
- TDI Classifications 2020Document3 pagesTDI Classifications 2020baridinoNo ratings yet
- Gram PosetiveDocument82 pagesGram Posetiveabrham sharewNo ratings yet
- Extending The Parent-Delivered Early Start Denver Model To Young Children With Fragile X SyndromeDocument17 pagesExtending The Parent-Delivered Early Start Denver Model To Young Children With Fragile X SyndromeLuis SeixasNo ratings yet
- 18 Infective EndocarditisDocument15 pages18 Infective EndocarditisCabdiNo ratings yet
- Upper Airway Obstruction: Ref.: Nelson Essentials of Pediatrics 7 - Edit. Nelson's Textbook of Pediatrics 20 - EditDocument5 pagesUpper Airway Obstruction: Ref.: Nelson Essentials of Pediatrics 7 - Edit. Nelson's Textbook of Pediatrics 20 - EditAli Abd AlrezaqNo ratings yet
- Metal AllergyDocument6 pagesMetal AllergyLinda RamadhantyNo ratings yet
- Sex Education Is A Must Learn Topic in Schools 1Document5 pagesSex Education Is A Must Learn Topic in Schools 1Sophia Mariel GonzalNo ratings yet
- PIDATO BAHASA INGGRIS Smoking DangerDocument1 pagePIDATO BAHASA INGGRIS Smoking DangerMuhammadNo ratings yet
- Multiple-Choice Questions: Biology: Food and Humans Combined Science: Chapter 6 Food and HumansDocument25 pagesMultiple-Choice Questions: Biology: Food and Humans Combined Science: Chapter 6 Food and Humans何柏濤No ratings yet


































































































Download as pdf or txt
You might also like
- Gipsy Oracle Cards MeaningsDocument4 pagesGipsy Oracle Cards MeaningsFidel H. Viegas92% (12)
- SGOTDocument2 pagesSGOTDinesh Sreedharan0% (1)
- Chapter 012Document11 pagesChapter 012api-2813400240% (1)
- Caso Clínico - Chlamydia TrachomatisDocument4 pagesCaso Clínico - Chlamydia TrachomatisRigobertoNo ratings yet
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDocument7 pagesScabies and Pediculosis Pubis: An Update of Treatment Regimens and General Reviewsuryanto_malvinNo ratings yet
- GlandersDocument7 pagesGlandersRyan ChenNo ratings yet
- NocardiaDocument3 pagesNocardiasujithas0% (1)
- Miscellaneous Bacterial InfectionsDocument15 pagesMiscellaneous Bacterial InfectionsHumera Gull JunejoNo ratings yet
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDocument7 pagesScabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewNovita WulandariNo ratings yet
- Cestosis y Cestodos PDFDocument14 pagesCestosis y Cestodos PDFErnesto VersailleNo ratings yet
- Cryptococcal Lung MycosesDocument14 pagesCryptococcal Lung MycosesFebri Dwi HaryonoNo ratings yet
- Glanders: C H A P T E R 2 - 5 - 1 1Document10 pagesGlanders: C H A P T E R 2 - 5 - 1 1Ryan ChenNo ratings yet
- Diagnosis, Prevention, and Treatment of ScabiesDocument5 pagesDiagnosis, Prevention, and Treatment of ScabiesSince Ivanna RumbiakNo ratings yet
- Micp ReviewerDocument30 pagesMicp ReviewerFrancisca NairNo ratings yet
- Leprosy: An Overview of Pathophysiology: Disusun OlehDocument22 pagesLeprosy: An Overview of Pathophysiology: Disusun OlehDwi Endra Juli PraditoNo ratings yet
- Clinical Avian Nutrition Excerpt PDFDocument22 pagesClinical Avian Nutrition Excerpt PDFAlejandraNo ratings yet
- Clostridial infections-LR3Document8 pagesClostridial infections-LR3yomifNo ratings yet
- Ecthyma Contagiosum (Human Orf)Document2 pagesEcthyma Contagiosum (Human Orf)Deba P SarmaNo ratings yet
- Assignment Hdb10503 Basic MicrobiologyDocument4 pagesAssignment Hdb10503 Basic MicrobiologyNida RidzuanNo ratings yet
- Diagnosis of Leishmaniasis: Review ArticleDocument12 pagesDiagnosis of Leishmaniasis: Review ArticleTUfoodbiotech groupNo ratings yet
- 37-54 Salmonella in CalvesDocument18 pages37-54 Salmonella in CalvesAna OspinaNo ratings yet
- Klebsiella Pneumoniae Pathogenesis: Etiology/BacteriologyDocument4 pagesKlebsiella Pneumoniae Pathogenesis: Etiology/Bacteriologysuper cute100% (1)
- Retrospective Study of Feline and Canine Cryptococcosis in Australia From 1981 To 2001: 195 CasesDocument12 pagesRetrospective Study of Feline and Canine Cryptococcosis in Australia From 1981 To 2001: 195 CasesKlaus Ramirez SuarezNo ratings yet
- Tugas Kukel WulanDocument15 pagesTugas Kukel WulanDonny Ardika NovanandaNo ratings yet
- Clinical Microbiology Reviews-1998-Podschun-589.fullDocument15 pagesClinical Microbiology Reviews-1998-Podschun-589.fullDorin SaulescuNo ratings yet
- StrongyloidiasisDocument5 pagesStrongyloidiasisMufidah OthmanNo ratings yet
- ChlamydiaDocument13 pagesChlamydiaTitus MutwiriNo ratings yet
- Prospective Study in A Porcine Model of Sarcoptes Scabiei Indicates The Association of Th2 and Th17 Pathways With The Clinical Severity of ScabiesDocument17 pagesProspective Study in A Porcine Model of Sarcoptes Scabiei Indicates The Association of Th2 and Th17 Pathways With The Clinical Severity of ScabiespunyayaNo ratings yet
- Scabies: Signs and SymptomsDocument5 pagesScabies: Signs and Symptomsputri intanNo ratings yet
- L1 - Actinomyces and NocardiaDocument45 pagesL1 - Actinomyces and Nocardiadvph2fck6qNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document38 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- Cryptococcosis ManualDocument3 pagesCryptococcosis Manualnassem54No ratings yet
- Common Intestinal ParasitesDocument16 pagesCommon Intestinal ParasitesbaliuwNo ratings yet
- Nocardia, Bordetella, HaemophilusDocument31 pagesNocardia, Bordetella, HaemophilusLourdes Cumagon BasiuangNo ratings yet
- Avsah v9 Id1091Document4 pagesAvsah v9 Id1091Azeneth CarolinaNo ratings yet
- Hookworm: Ancylostoma Duodenale and Necator AmericanusDocument18 pagesHookworm: Ancylostoma Duodenale and Necator AmericanusPutri AmandaNo ratings yet
- Chapter 56Document57 pagesChapter 56Rahmat MuliaNo ratings yet
- Document 3Document3 pagesDocument 3theresia 102018040No ratings yet
- Jurnal OM 2Document6 pagesJurnal OM 2Reiza PrabandanaNo ratings yet
- Lecture Rickettsia Chlamydia, MycoplasmaDocument49 pagesLecture Rickettsia Chlamydia, MycoplasmaHabeeb Ali Baig100% (3)
- Microbiology Assignment Malaria Group1Document19 pagesMicrobiology Assignment Malaria Group1wallacec1017No ratings yet
- ASCARIASISDocument13 pagesASCARIASISSandra MichelleNo ratings yet
- Pink Pigtail in A Skin Biopsy: ScabiesDocument12 pagesPink Pigtail in A Skin Biopsy: ScabiesDeba P SarmaNo ratings yet
- An Introduction of MalariaDocument19 pagesAn Introduction of MalariaSomesh GuptaNo ratings yet
- ChlamydiaDocument22 pagesChlamydiadelia rahmaNo ratings yet
- Diseases: Infected With Scabies Again? Focus in Management in Long-Term Care FacilitiesDocument12 pagesDiseases: Infected With Scabies Again? Focus in Management in Long-Term Care FacilitiesGede AdiNo ratings yet
- Papular UrticariaDocument10 pagesPapular UrticariaNuri Sakina SuhartoNo ratings yet
- Immunoproteomic Approach To Elucidating The Pathogenesis of Cryptococcosis Caused by Cryptococcus GattiiDocument10 pagesImmunoproteomic Approach To Elucidating The Pathogenesis of Cryptococcosis Caused by Cryptococcus GattiiGabriella FreitasNo ratings yet
- Naegleria FowleriDocument14 pagesNaegleria FowleriAya AyaNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document36 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- Coexistence of Cutaneous Tuberculosis (Scrofuloderma) and Hanseniasis-A Rare PresentationDocument2 pagesCoexistence of Cutaneous Tuberculosis (Scrofuloderma) and Hanseniasis-A Rare PresentationGesza Utama PutraNo ratings yet
- Proceedings of The 34th World Small Animal Veterinary Congress WSAVA 2009Document4 pagesProceedings of The 34th World Small Animal Veterinary Congress WSAVA 2009Fitri HeartNo ratings yet
- Unknown: Pink Pigtail in A Skin Biopsy: What Is Your Diagnosis?Document3 pagesUnknown: Pink Pigtail in A Skin Biopsy: What Is Your Diagnosis?Deba P SarmaNo ratings yet
- Disease Caused by ProtozoansDocument21 pagesDisease Caused by ProtozoansBrijesh KumarNo ratings yet
- Cell Structure of Cryptococcus FungiDocument19 pagesCell Structure of Cryptococcus FungiArshjyoti SinghNo ratings yet
- Hookworm Infection - UpToDateDocument12 pagesHookworm Infection - UpToDatedesilasarybasriNo ratings yet
- Scabies Mites Alter The Skin Microbiome and PromoteDocument13 pagesScabies Mites Alter The Skin Microbiome and Promotemohammed bouchibaNo ratings yet
- Chapter 62 The Yeasts and Yeastlike OrganismsDocument33 pagesChapter 62 The Yeasts and Yeastlike OrganismsbartsnewNo ratings yet
- Groupone MycologyDocument14 pagesGroupone MycologyTilahun TesemaNo ratings yet
- Overview of Infectious Coryza in Chickens: Veterinary ManualDocument4 pagesOverview of Infectious Coryza in Chickens: Veterinary ManualSamapanNo ratings yet
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- Ilham Maulana CVDocument3 pagesIlham Maulana CVYusran FachryNo ratings yet
- Gambar 6 1. Diagram Alir Produksi DMDocument3 pagesGambar 6 1. Diagram Alir Produksi DMYusran FachryNo ratings yet
- 1.4 Product Distribution: Table 1.5 Percentage Distribution To 5 AreaDocument3 pages1.4 Product Distribution: Table 1.5 Percentage Distribution To 5 AreaYusran FachryNo ratings yet
- Tk22 Revised Midterm ReportDocument85 pagesTk22 Revised Midterm ReportYusran FachryNo ratings yet
- Insulation in LNG Storage and PipingDocument55 pagesInsulation in LNG Storage and PipingYusran FachryNo ratings yet
- Chemistry of Methyl Ester SulfonatesDocument8 pagesChemistry of Methyl Ester SulfonatesYusran FachryNo ratings yet
- TK11 Outline Assignment1 PDFDocument2 pagesTK11 Outline Assignment1 PDFYusran FachryNo ratings yet
- TK11 Outline Assignment1Document2 pagesTK11 Outline Assignment1Yusran FachryNo ratings yet
- 4horsemen PDFDocument2 pages4horsemen PDFYusran FachryNo ratings yet
- The 2 Covid-19 Wave in South Africa: Transmissibility & A 501.V2 VariantDocument12 pagesThe 2 Covid-19 Wave in South Africa: Transmissibility & A 501.V2 VariantBathandwa Malingo100% (6)
- Airway Assessment and ManagementDocument32 pagesAirway Assessment and ManagementAbishek NewbeginNo ratings yet
- Shaws-Textbook-Of-Gynaecology-17 487Document1 pageShaws-Textbook-Of-Gynaecology-17 487imran khanNo ratings yet
- 01 NGT Procedure With RationaleDocument4 pages01 NGT Procedure With RationaleAryaj SulitNo ratings yet
- Fix MAPPING AQSHA 3 SELASA, 09 NOVEMBER 2021Document10 pagesFix MAPPING AQSHA 3 SELASA, 09 NOVEMBER 2021Febbby Mutia SafiraNo ratings yet
- Ashton ManualDocument100 pagesAshton ManualAndrei BombardieruNo ratings yet
- Burkhart CVDocument6 pagesBurkhart CVapi-535300613No ratings yet
- S1 2021 409100 BibliographyDocument16 pagesS1 2021 409100 Bibliographyberliana PutriNo ratings yet
- Toxic Effects, Drug CalculationDocument185 pagesToxic Effects, Drug CalculationAntonette Africa MercadoNo ratings yet
- 14 Drug StudyDocument15 pages14 Drug StudyTricia AlvarezNo ratings yet
- PASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceDocument2 pagesPASCUAL, Jhigo V. REYES, Al Sebastian C. MEDINA, Chris Daniel J. PUSING, Daniel Joseph V. Documentation and Report Humss 11-3 Physical ScienceJhigo Villar Franco PascualNo ratings yet
- Take Away 2 - Airbus Hazard Prevention Handbook (Distribution Copy)Document41 pagesTake Away 2 - Airbus Hazard Prevention Handbook (Distribution Copy)UbernatorNo ratings yet
- Prevalence of Nematode Contracaecum and Cestode Ligula Intestinalis Parasites Infection in Two Fish Species at Lake TanaDocument8 pagesPrevalence of Nematode Contracaecum and Cestode Ligula Intestinalis Parasites Infection in Two Fish Species at Lake TanaIJARP PublicationsNo ratings yet
- Drug Study GuideDocument2 pagesDrug Study GuideAubrey SungaNo ratings yet
- 2020 Chapter Lung Cancer and Tobacco Smoking FinalDocument21 pages2020 Chapter Lung Cancer and Tobacco Smoking FinalMarco MerazNo ratings yet
- A Guide For Grandparents of Children With CancerDocument24 pagesA Guide For Grandparents of Children With CancerVanessa SilvaNo ratings yet
- Medical Mnemonics 4 PrintDocument65 pagesMedical Mnemonics 4 Printanne0521100% (1)
- Topic 3 Module 1 and 2 CombinedDocument24 pagesTopic 3 Module 1 and 2 CombinedPortia NothobileNo ratings yet
- TDI Classifications 2020Document3 pagesTDI Classifications 2020baridinoNo ratings yet
- Gram PosetiveDocument82 pagesGram Posetiveabrham sharewNo ratings yet
- Extending The Parent-Delivered Early Start Denver Model To Young Children With Fragile X SyndromeDocument17 pagesExtending The Parent-Delivered Early Start Denver Model To Young Children With Fragile X SyndromeLuis SeixasNo ratings yet
- 18 Infective EndocarditisDocument15 pages18 Infective EndocarditisCabdiNo ratings yet
- Upper Airway Obstruction: Ref.: Nelson Essentials of Pediatrics 7 - Edit. Nelson's Textbook of Pediatrics 20 - EditDocument5 pagesUpper Airway Obstruction: Ref.: Nelson Essentials of Pediatrics 7 - Edit. Nelson's Textbook of Pediatrics 20 - EditAli Abd AlrezaqNo ratings yet
- Metal AllergyDocument6 pagesMetal AllergyLinda RamadhantyNo ratings yet
- Sex Education Is A Must Learn Topic in Schools 1Document5 pagesSex Education Is A Must Learn Topic in Schools 1Sophia Mariel GonzalNo ratings yet
- PIDATO BAHASA INGGRIS Smoking DangerDocument1 pagePIDATO BAHASA INGGRIS Smoking DangerMuhammadNo ratings yet
- Multiple-Choice Questions: Biology: Food and Humans Combined Science: Chapter 6 Food and HumansDocument25 pagesMultiple-Choice Questions: Biology: Food and Humans Combined Science: Chapter 6 Food and Humans何柏濤No ratings yet