Download as pdf or txt
You might also like
- Birth-Certificate Form B3 & B4Document2 pagesBirth-Certificate Form B3 & B4presslink77% (217)
- Legal Tech and The Future of Civil Justice-Cambridge University Press (2023)Document398 pagesLegal Tech and The Future of Civil Justice-Cambridge University Press (2023)CesarNo ratings yet
- Manish Yadav V State of Up Criminal Misc Anticipatory Bail Application Us 438 CRPC No 4645 of 2022 Allahabad High Court 426374 PDFDocument9 pagesManish Yadav V State of Up Criminal Misc Anticipatory Bail Application Us 438 CRPC No 4645 of 2022 Allahabad High Court 426374 PDFArmaan SidNo ratings yet
- E104 Englisch enDocument3 pagesE104 Englisch enSirghi DavidNo ratings yet
- Individual Identification Information Record - OrEA 630 BlankDocument4 pagesIndividual Identification Information Record - OrEA 630 BlankDavid PylypNo ratings yet
- Syed Mohammad Raza Vs Abbas Bandi Bibi On 12 April, 1932Document5 pagesSyed Mohammad Raza Vs Abbas Bandi Bibi On 12 April, 1932samiaNo ratings yet
- Claim FormDocument3 pagesClaim Forma.a.wiratamaNo ratings yet
- బీమా - natural Claim FormDocument2 pagesబీమా - natural Claim FormGouse MohiddinNo ratings yet
- SD 1 & 2 - JV PartnerDocument3 pagesSD 1 & 2 - JV PartnerJunaid RazaNo ratings yet
- Applicability, Goals, and RequirementsDocument2 pagesApplicability, Goals, and RequirementsSagar BabarNo ratings yet
- Application For Information Under Section 42B of The Wealth-Tax Act, 1957Document1 pageApplication For Information Under Section 42B of The Wealth-Tax Act, 1957Amit BhatiNo ratings yet
- Heard About What Happened From SomeoneDocument6 pagesHeard About What Happened From Someoneapi-2606993No ratings yet
- I.M.E. Life Insurance Company LTD.: Physician'S Statement For Critical IllnessDocument2 pagesI.M.E. Life Insurance Company LTD.: Physician'S Statement For Critical IllnessMystic MilanNo ratings yet
- India Patent Form 15Document1 pageIndia Patent Form 15adityakochharNo ratings yet
- PPF FORM Application Form.Document3 pagesPPF FORM Application Form.agni08rahulNo ratings yet
- Enrollment Form For JW and SWDocument4 pagesEnrollment Form For JW and SWNoyingbeni MurryNo ratings yet
- 65 F 9327 F 17797Document3 pages65 F 9327 F 17797sasithNo ratings yet
- 2018 +Generali+Claim+form EN+ (Legal+rev) +-+171017Document2 pages2018 +Generali+Claim+form EN+ (Legal+rev) +-+171017Femi EvalnesNo ratings yet
- Microsoft Word Etb Life Medical Claim Bi 010312Document4 pagesMicrosoft Word Etb Life Medical Claim Bi 010312Fathi TahirNo ratings yet
- Form 18 - To Register As A Voter For Graduates Constituency ElectionDocument2 pagesForm 18 - To Register As A Voter For Graduates Constituency ElectionApnaComplexNo ratings yet
- AP6 Amendment of A Strata Plan by Adding or Removing LandDocument6 pagesAP6 Amendment of A Strata Plan by Adding or Removing LandConveyancers DirectoryNo ratings yet
- EncodedDocument13 pagesEncodedleahparker857No ratings yet
- Guarantors FORM - Doc BADocument3 pagesGuarantors FORM - Doc BAagbaipissNo ratings yet
- Formats For Medico-Legal CertificationDocument84 pagesFormats For Medico-Legal CertificationJoshua D. ALARBANo ratings yet
- Form 15Document2 pagesForm 15anon-91246No ratings yet
- India Patent Form 8Document2 pagesIndia Patent Form 8adityakochharNo ratings yet
- Both TL and WC ApplicationDocument4 pagesBoth TL and WC ApplicationSitharaman PrabhuramNo ratings yet
- ACT Application For Deposit of A Community PlanDocument6 pagesACT Application For Deposit of A Community PlanConveyancers DirectoryNo ratings yet
- Guarantors and Undertaking LettersDocument5 pagesGuarantors and Undertaking LettersDaniel Eleojo JoshuaNo ratings yet
- Background FormDocument3 pagesBackground FormTerenz World IIINo ratings yet
- Claim Application Form (Death)Document11 pagesClaim Application Form (Death)shehan senevirathnaNo ratings yet
- Note: You Have To Pay Rp..5.000,-For A Years Member of AEC. and You Will Get An IdentityDocument2 pagesNote: You Have To Pay Rp..5.000,-For A Years Member of AEC. and You Will Get An IdentityDimas VironikaNo ratings yet
- Business Name Registration Firm or Corporation 1639049602Document2 pagesBusiness Name Registration Firm or Corporation 1639049602Anthony MuhweziNo ratings yet
- CIS Application PDFDocument1 pageCIS Application PDFVictor Mirza100% (1)
- Money Lenders Renewal Application Form 2023Document2 pagesMoney Lenders Renewal Application Form 2023Donald MaasaNo ratings yet
- National Insurance Scheme Application For Compliance Certificate (Self-Employed Persons)Document1 pageNational Insurance Scheme Application For Compliance Certificate (Self-Employed Persons)DeSouza JuvitaNo ratings yet
- Application For Purchace of A House: Tema Development CorporationDocument3 pagesApplication For Purchace of A House: Tema Development CorporationJaysonn KayNo ratings yet
- Claim For Inclusion of Name in The Electoral Roll For A Graduates' ConstituencyDocument2 pagesClaim For Inclusion of Name in The Electoral Roll For A Graduates' ConstituencyashwinmjoshiNo ratings yet
- Downloadfile PDFDocument2 pagesDownloadfile PDFRatan RatanNo ratings yet
- Upsida Kya FormDocument2 pagesUpsida Kya FormAshish BansalNo ratings yet
- Final Service Provider Application Form Sample - 26.09.2019Document3 pagesFinal Service Provider Application Form Sample - 26.09.2019Keshav SoomarahNo ratings yet
- SSS Application FormDocument3 pagesSSS Application FormRaj KumarNo ratings yet
- Tenants Application Form Residential 1Document4 pagesTenants Application Form Residential 1adeola tayoNo ratings yet
- Application Form - 1.0 Final-CMCALSSDocument3 pagesApplication Form - 1.0 Final-CMCALSSNguwruw Chungpha MoyonNo ratings yet
- PPF-Account Opening FormDocument3 pagesPPF-Account Opening Formkamal godhaniya1988No ratings yet
- Form 19 EnglishDocument2 pagesForm 19 EnglishSachi SivamNo ratings yet
- Accident Report Form-UpdatedDocument4 pagesAccident Report Form-UpdatedPrince QuaysonNo ratings yet
- Form LRA 9 GENERAL APPLICATION FOR REGISTRATIONDocument3 pagesForm LRA 9 GENERAL APPLICATION FOR REGISTRATIONmoonlightphotographybungomaNo ratings yet
- Bai Tap LC Tieng AnhDocument3 pagesBai Tap LC Tieng AnhNguyễn Kỳ MinhNo ratings yet
- MBD 4 Declaration of InterestDocument3 pagesMBD 4 Declaration of InterestMichael ZakweNo ratings yet
- DIR Abutment FormDocument2 pagesDIR Abutment FormsteveNo ratings yet
- Application FormDocument1 pageApplication FormGroup AIRSNo ratings yet
- MV Registration & DL LL FormDocument2 pagesMV Registration & DL LL Formkarma wangyalNo ratings yet
- Application For Capture Import Export Re-Export Form - March 2019Document4 pagesApplication For Capture Import Export Re-Export Form - March 2019Paul Ndung'uNo ratings yet
- University of Colombo, Sri Lanka Faculty of Law Department of Private and Comparative LawDocument3 pagesUniversity of Colombo, Sri Lanka Faculty of Law Department of Private and Comparative Law22nk5yq2d9No ratings yet
- Trade Lead Bulletin Reply Form - 2 - 1Document2 pagesTrade Lead Bulletin Reply Form - 2 - 1Rokeya Roxi Valli0% (1)
- INDIVIDUAL APPLICATION FOR MEMBERSHIP August 2022Document4 pagesINDIVIDUAL APPLICATION FOR MEMBERSHIP August 2022macklean lionelNo ratings yet
- SF-HSE-ForM-2 - 01-4b COID - W.cl.3 - Notice of Accident and Claim For CompensationDocument2 pagesSF-HSE-ForM-2 - 01-4b COID - W.cl.3 - Notice of Accident and Claim For Compensationsjorgundson17No ratings yet
- American Credit Repair: Everything U Need to Know About Raising Your Credit ScoreFrom EverandAmerican Credit Repair: Everything U Need to Know About Raising Your Credit ScoreRating: 3 out of 5 stars3/5 (3)
- The Amazing Biological Revolution and The Amazing New Health CareFrom EverandThe Amazing Biological Revolution and The Amazing New Health CareNo ratings yet
- The Forensic Documentation Sourcebook: The Complete Paperwork Resource for Forensic Mental Health PracticeFrom EverandThe Forensic Documentation Sourcebook: The Complete Paperwork Resource for Forensic Mental Health PracticeRating: 1 out of 5 stars1/5 (1)
- The Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsFrom EverandThe Addiction Counselor's Documentation Sourcebook: The Complete Paperwork Resource for Treating Clients with AddictionsNo ratings yet
- Complaint - Juan Dela CruzDocument3 pagesComplaint - Juan Dela CruzLaika HernandezNo ratings yet
- 46 Virata Vs SandiganbayanDocument2 pages46 Virata Vs SandiganbayanFrancis Masiglat100% (2)
- Penolakan Pemberian Rekomendasi Pembebanan Hak Tanggungan Terhadap Hak Guna Bangunan Di Atas Hak Pengelolaan Pemerintah Kalimantan TimurDocument16 pagesPenolakan Pemberian Rekomendasi Pembebanan Hak Tanggungan Terhadap Hak Guna Bangunan Di Atas Hak Pengelolaan Pemerintah Kalimantan TimurAhmad VanheidenNo ratings yet
- Ra 11479-Terrorism Law of 2020Document25 pagesRa 11479-Terrorism Law of 2020Christian Dave Tad-awanNo ratings yet
- MAAS, HistoriaDocument16 pagesMAAS, HistoriaVale PepinoNo ratings yet
- Motion To Move Cootie Browns Lawsuit To Cicruit CourtDocument5 pagesMotion To Move Cootie Browns Lawsuit To Cicruit CourtJessica FullerNo ratings yet
- Case StudyDocument3 pagesCase StudySaira VillarNo ratings yet
- Form - P - 2-A - Register of WagesDocument3 pagesForm - P - 2-A - Register of WagesSailaja SubramanyamNo ratings yet
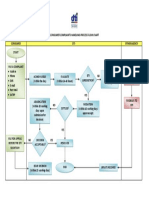
- DTI Consumer Complaints Handling Process Flow (As of 07 August 2015) FDocument1 pageDTI Consumer Complaints Handling Process Flow (As of 07 August 2015) FOna DlanorNo ratings yet
- GST Invoice: Name: Yash Prestek Invoice No: XTS18052021Document2 pagesGST Invoice: Name: Yash Prestek Invoice No: XTS18052021Harshal PatilNo ratings yet
- Ak Mentoring Day 2 Swing Trading: Starts at 7amDocument36 pagesAk Mentoring Day 2 Swing Trading: Starts at 7amAvadhesh Kumar SinghNo ratings yet
- The Standard: COVID-19Document25 pagesThe Standard: COVID-19julietNo ratings yet
- Gerbert R. Corpuz vs. Daisylyn Tirol Sto. Tomas G.R. No. 186571 August 11, 2010 Brion, J.: FactsDocument4 pagesGerbert R. Corpuz vs. Daisylyn Tirol Sto. Tomas G.R. No. 186571 August 11, 2010 Brion, J.: FactsEloisa SalitreroNo ratings yet
- CJ Admin Reviewer PDFDocument21 pagesCJ Admin Reviewer PDFSophiaFrancescaEspinosaNo ratings yet
- Reaction PaperDocument4 pagesReaction PaperVirnadette Lopez100% (1)
- River Cities Reader #1017 - January 2024Document32 pagesRiver Cities Reader #1017 - January 2024River Cities ReaderNo ratings yet
- Atty's Fees:Atty-CLient Rel. (27-30) PDFDocument3 pagesAtty's Fees:Atty-CLient Rel. (27-30) PDFJan Maxine Palomata0% (1)
- Henry Methvin Trial March 1935, in His Own WordsDocument2 pagesHenry Methvin Trial March 1935, in His Own WordsCharles Flynn100% (1)
- Practice Court ScriptDocument13 pagesPractice Court ScriptAnne VallaritNo ratings yet
- Zhange Wei, Human Peacekeeper & Paladin of The Celestial EmperorDocument7 pagesZhange Wei, Human Peacekeeper & Paladin of The Celestial EmperorKai927No ratings yet
- Sta Rosa, Laguna Building PermitDocument2 pagesSta Rosa, Laguna Building Permitjaja enciso100% (1)
- 20532D ENU TrainerHandbookDocument240 pages20532D ENU TrainerHandbookjelopezzNo ratings yet
- Lesson 52ND Q ManifestoDocument30 pagesLesson 52ND Q ManifestoLiya Mae SantiagoNo ratings yet
- Rama Telecom: Billed To: Shipped ToDocument1 pageRama Telecom: Billed To: Shipped ToLila DeviNo ratings yet
- Filename 3Document9 pagesFilename 3pporwal197No ratings yet
- ChangDocument5 pagesChangJ RohrlichNo ratings yet
- Law All Case LawsDocument91 pagesLaw All Case LawsQuestion Bank100% (4)