Download as pdf or txt
You might also like
- 06 237046 001 - BDDocument1 page06 237046 001 - BDcarlos yepezNo ratings yet
- Decentralized AccountingDocument10 pagesDecentralized AccountingMartin AcantiladoNo ratings yet
- Lifedirex Covid-19 RT-QPCR Detection Kit: - ProtocolDocument5 pagesLifedirex Covid-19 RT-QPCR Detection Kit: - ProtocolRadit AMSNo ratings yet
- Data Sheet: Coronavirus (Sars-Cov-2) RT-QPCR Detection KitDocument3 pagesData Sheet: Coronavirus (Sars-Cov-2) RT-QPCR Detection KitAslam MikraniNo ratings yet
- STGF CD302M IFU RUO Version2Document2 pagesSTGF CD302M IFU RUO Version2eva evaNo ratings yet
- PdfText 938Document1 pagePdfText 938Chaitanya Chowdary100% (1)
- Direct Sars-Cov-2 Realtime PCR - en - Pme103-07.20Document2 pagesDirect Sars-Cov-2 Realtime PCR - en - Pme103-07.20andi takwaNo ratings yet
- Report 2Document1 pageReport 2anshul shahNo ratings yet
- S Shardaben Kalsaria Fem: Ale / 25 YearsDocument1 pageS Shardaben Kalsaria Fem: Ale / 25 YearsMonika MotiyaniNo ratings yet
- EUA ThermoFisher Applied Biosystems TaqPath COVID 19 Combo Kit Rutgers University SummaryDocument8 pagesEUA ThermoFisher Applied Biosystems TaqPath COVID 19 Combo Kit Rutgers University SummaryAnushanNo ratings yet
- Tilapa Lake Virus One-Step ManualDocument5 pagesTilapa Lake Virus One-Step ManualCuong NguyenNo ratings yet
- COVID19 Qualitative by Real Time PCRDocument1 pageCOVID19 Qualitative by Real Time PCRAmritNo ratings yet
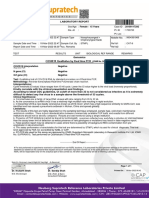
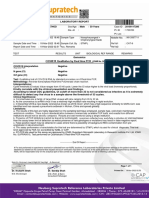
- COVID19 Qualitative by Real Time PCR: COVID19 Interpretation Positive N Gene (CT) 27 Orf Gene (CT) 24 Test: MethodologyDocument1 pageCOVID19 Qualitative by Real Time PCR: COVID19 Interpretation Positive N Gene (CT) 27 Orf Gene (CT) 24 Test: MethodologyNihar DaveNo ratings yet
- File 1434571027Document1 pageFile 1434571027Guneyden GuneydenNo ratings yet
- Bustin Mueller QPCR 2005Document15 pagesBustin Mueller QPCR 2005theyuri@tlen.plNo ratings yet
- GP Letak A4 HBV IVDD EN 5 2023Document2 pagesGP Letak A4 HBV IVDD EN 5 2023Fatima VessaliusNo ratings yet
- PDF TextDocument1 pagePDF TextPawan KalyanNo ratings yet
- Anger ManegmentDocument1 pageAnger Manegmentchetan selokarNo ratings yet
- 2020-09-23 Branson Slides FinalDocument63 pages2020-09-23 Branson Slides FinalJordan SandayanNo ratings yet
- COVID19 Qualitative by Real Time PCRDocument2 pagesCOVID19 Qualitative by Real Time PCRKirtan J. PatelNo ratings yet
- Rna ExtractionDocument40 pagesRna ExtractionyasirNo ratings yet
- ReportDocument1 pageReportDhruv RanaNo ratings yet
- Truenat SARS CoV 2 Packinsert VER 03Document4 pagesTruenat SARS CoV 2 Packinsert VER 03yousra zeidanNo ratings yet
- COVID19 Qualitative by Real Time PCRDocument1 pageCOVID19 Qualitative by Real Time PCRNikhil JoseNo ratings yet
- Kavan FDocument1 pageKavan FIMOUNT ONENo ratings yet
- Quality Control in SARS COV-2 RNA TestingDocument63 pagesQuality Control in SARS COV-2 RNA TestingNanik AndianiNo ratings yet
- RNA Extraction ProtocolDocument40 pagesRNA Extraction ProtocolyasirNo ratings yet
- 17 April NMMC - Covid-19 Laboratory - Test ReportDocument1 page17 April NMMC - Covid-19 Laboratory - Test ReportHarshada AndhereNo ratings yet
- CL 1000i Chemiluminescence Immunoassay SystemDocument6 pagesCL 1000i Chemiluminescence Immunoassay SystemOsama ElfadniNo ratings yet
- Faqs On Diagnostic Testing For Sars-Cov-2Document7 pagesFaqs On Diagnostic Testing For Sars-Cov-2indraNo ratings yet
- TestReport 203300095Document1 pageTestReport 203300095Sravan KrNo ratings yet
- Meera FDocument1 pageMeera FIMOUNT ONENo ratings yet
- EUA Quest SARS IfuDocument28 pagesEUA Quest SARS IfuBayan Abu AlrubNo ratings yet
- Mr. Haan Kanuga 3 Years 20100117282: COVID19 Qualitative by Real Time PCRDocument1 pageMr. Haan Kanuga 3 Years 20100117282: COVID19 Qualitative by Real Time PCRIMOUNT ONENo ratings yet
- WHO Global Round of Laboratory Proficiency Testing For The Detection of SARS-CoV-2 by PCR Result Entry myQAP PortalDocument2 pagesWHO Global Round of Laboratory Proficiency Testing For The Detection of SARS-CoV-2 by PCR Result Entry myQAP PortalpermencokelatNo ratings yet
- Enali FDocument1 pageEnali FIMOUNT ONENo ratings yet
- Pankajkumar FDocument1 pagePankajkumar FIMOUNT ONENo ratings yet
- 3364 AbbottDocument1 page3364 AbbottNataliia NataliaNo ratings yet
- IFU Check-Direct - CPO - BD - MAXDocument26 pagesIFU Check-Direct - CPO - BD - MAXRickettsia ProwazekiiNo ratings yet
- Bustin Mueller QPCR 2005Document15 pagesBustin Mueller QPCR 2005investbiz optionstarNo ratings yet
- Real-Time Fluorescent RT-PCR: Product PerformanceDocument5 pagesReal-Time Fluorescent RT-PCR: Product PerformanceMihail AvramovNo ratings yet
- Adams 2020Document5 pagesAdams 2020javier andres perez gomezNo ratings yet
- QuantiNova Real-Time PCR Kits PDFDocument4 pagesQuantiNova Real-Time PCR Kits PDFGIUGAB6392No ratings yet
- Mr. Jainil Patel 10 Years: COVID19 Qualitative by Real Time PCRDocument1 pageMr. Jainil Patel 10 Years: COVID19 Qualitative by Real Time PCRIMOUNT ONENo ratings yet
- Genotip-C - en (HEPATITIS C VIRUS GENOTYPING PCR KIT (RT REAGENTS AND PREP-NA INCLUDED) )Document4 pagesGenotip-C - en (HEPATITIS C VIRUS GENOTYPING PCR KIT (RT REAGENTS AND PREP-NA INCLUDED) )Mohamad ImamNo ratings yet
- 2019 nCoV Detection Kit Leaflet English PDFDocument2 pages2019 nCoV Detection Kit Leaflet English PDFCindy MangayaNo ratings yet
- COVID-19 - Real Time RNA: 50 / 100 /150 Tests (Ready To Use Kit)Document5 pagesCOVID-19 - Real Time RNA: 50 / 100 /150 Tests (Ready To Use Kit)lupibudiNo ratings yet
- Eul 0515 202 00 Covid19 Coronavirus Real Time PCR Kit IfuDocument28 pagesEul 0515 202 00 Covid19 Coronavirus Real Time PCR Kit IfuashishvaidNo ratings yet
- EUA Labcorp COVID EUAsum - 1Document28 pagesEUA Labcorp COVID EUAsum - 1ssahni9No ratings yet
- MumtazDocument1 pageMumtazSaqib Mahmood BhuttaNo ratings yet
- Monolisa HCV Ag-Ac UltraDocument4 pagesMonolisa HCV Ag-Ac UltraSantiagoAFNo ratings yet
- Aplikasi Pemeriksaan RT-PCR Sars Cov 2: Basti AndriyokoDocument25 pagesAplikasi Pemeriksaan RT-PCR Sars Cov 2: Basti AndriyokoAlif Adiyudha PratamaNo ratings yet
- EUA SDI SARS CoV 2 Assay Specialty Diagnostic Laboratories SummaryDocument7 pagesEUA SDI SARS CoV 2 Assay Specialty Diagnostic Laboratories SummaryLucasNo ratings yet
- MolBio Activity 7 - Assay Worksheet (SansureDocument4 pagesMolBio Activity 7 - Assay Worksheet (SansureAnneNo ratings yet
- Taqpath Covid 19 Ce Ivd FaqDocument4 pagesTaqpath Covid 19 Ce Ivd Faqmiguel david MarfilNo ratings yet
- HPV QUANT-21 - Form A6 - Specification of ProductDocument4 pagesHPV QUANT-21 - Form A6 - Specification of ProductLAB PCRNo ratings yet
- Overview of Real-Q 2019-Ncov Detection KitDocument2 pagesOverview of Real-Q 2019-Ncov Detection Kitbimo spNo ratings yet
- Berbagai Metoda Dan Target Gen Pada Pemeriksaan PCR: Sars-Cov-2 Covid-19Document19 pagesBerbagai Metoda Dan Target Gen Pada Pemeriksaan PCR: Sars-Cov-2 Covid-19Suherman AndiNo ratings yet
- Powerchek™ 2019-Ncov Real-Time PCR Kit: Instructions For UseDocument30 pagesPowerchek™ 2019-Ncov Real-Time PCR Kit: Instructions For Usedrestadyumna ChilspiderNo ratings yet
- DG Molecular HIV 2013Document37 pagesDG Molecular HIV 2013Dorina BoldNo ratings yet
- New York Sars-Cov-2 Real-Time Reverse Transcriptase (RT) - PCR Diagnostic PanelDocument27 pagesNew York Sars-Cov-2 Real-Time Reverse Transcriptase (RT) - PCR Diagnostic PanelcassNo ratings yet
- Di MCB DB Pricelist01!07!2018Document1 pageDi MCB DB Pricelist01!07!2018saurabhjerps231221No ratings yet
- Problems Faced in Spoken English Among Learning Disabilities StudentsDocument12 pagesProblems Faced in Spoken English Among Learning Disabilities StudentsTompok ManggisNo ratings yet
- Total Parenteral NutritionDocument59 pagesTotal Parenteral NutritionMARIAH ALEXIE GASALNo ratings yet
- Design, Calculation and Simulation 3 Dof Capacitive Force SensorDocument5 pagesDesign, Calculation and Simulation 3 Dof Capacitive Force SensorLaNo ratings yet
- Global Vaccine Action Plan: Tetanus & Difteri (TD/DPT)Document6 pagesGlobal Vaccine Action Plan: Tetanus & Difteri (TD/DPT)Gusti IndrakusumaNo ratings yet
- Raj GeographyDocument42 pagesRaj Geographyhemant.niotNo ratings yet
- 17-Stream Water Quality Analysis - F11Document12 pages17-Stream Water Quality Analysis - F11Michelle de Jesus100% (1)
- 2003 CaCO3-Panthi-2003Document16 pages2003 CaCO3-Panthi-2003Izzat W. KaziNo ratings yet
- Design For Multiple ReactionsDocument43 pagesDesign For Multiple Reactionsmuhammad shahadat awanNo ratings yet
- Chapter2 RRLDocument23 pagesChapter2 RRLJoseph DelgadoNo ratings yet
- MSDS Citronela OilDocument9 pagesMSDS Citronela OilIndra SanjayaNo ratings yet
- ReferenceDocument5 pagesReferencenikhil moreNo ratings yet
- Psychoanalytic Theory of Sigmund FreudDocument7 pagesPsychoanalytic Theory of Sigmund FreudDairel MansuetoNo ratings yet
- 1 - FLD-25 3D Printer Filament MachineDocument11 pages1 - FLD-25 3D Printer Filament MachineNitin PatilNo ratings yet
- Mpaps G 9012Document5 pagesMpaps G 9012mpedraza-1No ratings yet
- Flight Operation - WIMM QuickviewDocument2 pagesFlight Operation - WIMM QuickviewFadhlullah ReynadinNo ratings yet
- GE Healthcare Supplies CatalogDocument74 pagesGE Healthcare Supplies Catalogsneri.salud.bcs2260No ratings yet
- Pelayanan Kesehatan Peduli Remaja Menurut Perspektif Remaja Di Kota MagelangDocument9 pagesPelayanan Kesehatan Peduli Remaja Menurut Perspektif Remaja Di Kota MagelangArviera KayNo ratings yet
- Programme Fire Sprinkler International 2023 3Document4 pagesProgramme Fire Sprinkler International 2023 3Carlos_MKTRNo ratings yet
- SujoodDocument7 pagesSujoodapi-19729317No ratings yet
- Metodo Hach HierroDocument6 pagesMetodo Hach HierroJESSICA VANESSA ARISMENDI AVILEZNo ratings yet
- ACLS Practical Case Scenarios (1 June 2011)Document15 pagesACLS Practical Case Scenarios (1 June 2011)nersNo ratings yet
- Brochure - HRM ThreadDocument6 pagesBrochure - HRM ThreadPrateek KumarNo ratings yet
- Flow Controller TotalizerDocument3 pagesFlow Controller TotalizerDhiraj MistryNo ratings yet
- How Much Floor Space Needs A Broiler Chicken?: July 2011Document4 pagesHow Much Floor Space Needs A Broiler Chicken?: July 2011zohaib hafeezNo ratings yet
- List of Periodic Checks Life Saving & Fire Fighting EquipmentDocument5 pagesList of Periodic Checks Life Saving & Fire Fighting EquipmentSandro CheNo ratings yet
- 2018 Annual Review enDocument69 pages2018 Annual Review enphoenixNo ratings yet
- NCP ConstipationDocument3 pagesNCP Constipationjlucando50% (2)