Download as pdf or txt
You might also like
- Chem 28 SyllabusDocument11 pagesChem 28 SyllabusDianne TorrecampoNo ratings yet
- 2019 Article 1596Document9 pages2019 Article 1596Arina FitrianiNo ratings yet
- Clinical Epidemiology and Global Health: Original ArticleDocument4 pagesClinical Epidemiology and Global Health: Original Articleinnani wildaniaNo ratings yet
- Effects of A Free Water Protocol On Inpatients inDocument7 pagesEffects of A Free Water Protocol On Inpatients inCamila Jaque RamosNo ratings yet
- Graziella Allana Serra Alves de Oliveira Olle 2018Document12 pagesGraziella Allana Serra Alves de Oliveira Olle 2018Anindya Laksmi LarasatiNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka BangaloreDocument13 pagesRajiv Gandhi University of Health Sciences, Karnataka BangaloreFebri SuryoNo ratings yet
- GROUP 4 EBP On Renal NursingDocument7 pagesGROUP 4 EBP On Renal Nursingczeremar chanNo ratings yet
- Marie Antonette D.O. TanDocument159 pagesMarie Antonette D.O. TanJeffreydanceljr100% (5)
- Preference Dry WeightDocument8 pagesPreference Dry WeightdharmaNo ratings yet
- Contributing Factors To Hemodialysis Adherence in Aceh, Indonesia - ScienceDirectDocument6 pagesContributing Factors To Hemodialysis Adherence in Aceh, Indonesia - ScienceDirectlaamaghfirohNo ratings yet
- Association Between Hemodialysis Adequacy, Family Support, and Quality of Life in Chronic Renal Failure PatientsDocument10 pagesAssociation Between Hemodialysis Adequacy, Family Support, and Quality of Life in Chronic Renal Failure PatientsJelisaaNo ratings yet
- Jurnal 5Document8 pagesJurnal 5innani wildaniaNo ratings yet
- Albumin in aSAH NeuroCrit2023Document11 pagesAlbumin in aSAH NeuroCrit2023Ahida VelazquezNo ratings yet
- The Compliance Chronic Renal Failure Patient On Restrictions Liquids in Hemodialysis TherapyDocument7 pagesThe Compliance Chronic Renal Failure Patient On Restrictions Liquids in Hemodialysis TherapyJurnal Ners UNAIRNo ratings yet
- Fluid and Dietary Restriction's Effi Cacy On Chronic Kidney Disease Patients in HemodialysisDocument9 pagesFluid and Dietary Restriction's Effi Cacy On Chronic Kidney Disease Patients in HemodialysisfitriNo ratings yet
- The Association Between High Volume Intraoperative Fluid Administration and Outcomes Among Pediatric Patients Undergoing Large Bowel ResectionDocument7 pagesThe Association Between High Volume Intraoperative Fluid Administration and Outcomes Among Pediatric Patients Undergoing Large Bowel ResectionPablo Segales BautistaNo ratings yet
- Improving Adherence and Biomedical Markers in Hemodialysis Patients: The Effects of Relaxation TherapyDocument9 pagesImproving Adherence and Biomedical Markers in Hemodialysis Patients: The Effects of Relaxation TherapyheriNo ratings yet
- Resume Jurnal ADocument11 pagesResume Jurnal AannisaNo ratings yet
- MousaDocument12 pagesMousaGiriNo ratings yet
- The Relationship Between Social Support With Dietary and Fluids Restrictions Adherence Among Hemodialysis Patients in IndonesiaDocument5 pagesThe Relationship Between Social Support With Dietary and Fluids Restrictions Adherence Among Hemodialysis Patients in IndonesiaIndah Ayu KustianingsihNo ratings yet
- Acta Anaesthesiol Scand - 2022 - JessenDocument10 pagesActa Anaesthesiol Scand - 2022 - Jessenนิ่ม มมNo ratings yet
- Protein Energy Malnutrition in CKD PatientsDocument4 pagesProtein Energy Malnutrition in CKD PatientsEditor IJTSRDNo ratings yet
- Japan Journal Nursing Sci - 2014 - Efe - Adherence To Diet and Fluid Restriction of Individuals On Hemodialysis TreatmentDocument11 pagesJapan Journal Nursing Sci - 2014 - Efe - Adherence To Diet and Fluid Restriction of Individuals On Hemodialysis TreatmentCacaNo ratings yet
- Early TIPS Versus Endoscopic Therapy For Secondary Prophylaxis After Management of Acute Esophageal Variceal Bleeding in Cirrhotic Patients: A Meta-Analysis of Randomized Controlled TrialsDocument26 pagesEarly TIPS Versus Endoscopic Therapy For Secondary Prophylaxis After Management of Acute Esophageal Variceal Bleeding in Cirrhotic Patients: A Meta-Analysis of Randomized Controlled Trialsray liNo ratings yet
- Original Article: Saudi Journal of Kidney Diseases and TransplantationDocument5 pagesOriginal Article: Saudi Journal of Kidney Diseases and TransplantationNiponis ChunchunNo ratings yet
- Four Phases of Intravenous Fluid Therapy: A Conceptual ModelDocument8 pagesFour Phases of Intravenous Fluid Therapy: A Conceptual ModelriahtakarinaNo ratings yet
- Effect of Comprehensive Nursing Strategies On Thirst Distress Management Among The Patients With Chronic Kidney Disease (CKD)Document6 pagesEffect of Comprehensive Nursing Strategies On Thirst Distress Management Among The Patients With Chronic Kidney Disease (CKD)yanuar esthoNo ratings yet
- Manajemen Cairan Pada Pasien Hemodialisis Untuk Meningkatkan Kualitas Hidup Di RSUD Dr. Harjono PonorogoDocument11 pagesManajemen Cairan Pada Pasien Hemodialisis Untuk Meningkatkan Kualitas Hidup Di RSUD Dr. Harjono PonorogonikaNo ratings yet
- Prob 2Document12 pagesProb 2jinsi georgeNo ratings yet
- Tips For Dialysis Patients With Fluid Restrictions: Melanie Wong, BS, Parianna Ghebleh, BS, and Stacey Phillips, MS, RDDocument4 pagesTips For Dialysis Patients With Fluid Restrictions: Melanie Wong, BS, Parianna Ghebleh, BS, and Stacey Phillips, MS, RDanarosli251No ratings yet
- PIIS2213398416300380Document6 pagesPIIS2213398416300380LiliNurmawatiNo ratings yet
- Noninvasive Monitoring 2016Document6 pagesNoninvasive Monitoring 2016Maria LaiaNo ratings yet
- Acta Anaesthesiol Scand - 2022 - Jessen - Fluid Management of Emergency Department Patients With Sepsis A Survey of FluidDocument10 pagesActa Anaesthesiol Scand - 2022 - Jessen - Fluid Management of Emergency Department Patients With Sepsis A Survey of FluidEros CastellaniNo ratings yet
- Environmental Research and Public Health: International Journal ofDocument12 pagesEnvironmental Research and Public Health: International Journal ofdarnila watiNo ratings yet
- Family Concern: Facilitating Self-Management of Patients Undergoing HemodialysisDocument4 pagesFamily Concern: Facilitating Self-Management of Patients Undergoing HemodialysisGalica GalicaNo ratings yet
- Ghimire 2016Document7 pagesGhimire 2016john markNo ratings yet
- Comparison The Effect of High Flux and Low Flux Dialyzer On Quality of Life in Hemodialysis Patients A Clinical TrialDocument8 pagesComparison The Effect of High Flux and Low Flux Dialyzer On Quality of Life in Hemodialysis Patients A Clinical TrialMrQmonkNo ratings yet
- The Effects of Nursing of Roy Adaptation Model On The Elderly Hypertensive: A Randomised Control StudyDocument10 pagesThe Effects of Nursing of Roy Adaptation Model On The Elderly Hypertensive: A Randomised Control Studyjinsi georgeNo ratings yet
- Questionnaire Survey On Nutritional Supplement TheDocument10 pagesQuestionnaire Survey On Nutritional Supplement Theanselma.villafrancaNo ratings yet
- Effects of Oral Intake of WateDocument11 pagesEffects of Oral Intake of WateChenNo ratings yet
- Identification of The Needs of Haemodialysis Patients Using The Concept of Maslow's Hierarchy of NeedsDocument8 pagesIdentification of The Needs of Haemodialysis Patients Using The Concept of Maslow's Hierarchy of NeedsAlyssa LeonesNo ratings yet
- Nutritional Status and Malnutrition Prevalence Among Maintenance Hemodialysis PatientsDocument8 pagesNutritional Status and Malnutrition Prevalence Among Maintenance Hemodialysis PatientsIOSRjournalNo ratings yet
- Ojsadmin, 12Document5 pagesOjsadmin, 12Yohana SimanjuntakNo ratings yet
- Dwi Arya Jurnal UjianDocument8 pagesDwi Arya Jurnal Ujianwulan nadiaNo ratings yet
- Salina Vs GlucosadaDocument10 pagesSalina Vs GlucosadaEmmanuel Guar HuaNo ratings yet
- The Most Frequent Diagnosis On Patients Undergoing HemodialysisDocument5 pagesThe Most Frequent Diagnosis On Patients Undergoing HemodialysisChristine Rose EmNo ratings yet
- Fluid Balance and Optimal Hydration Guideline For Adult InpatientsDocument6 pagesFluid Balance and Optimal Hydration Guideline For Adult InpatientsOvidiu MCNo ratings yet
- JNursMidwiferySci7294-9611226 024011Document5 pagesJNursMidwiferySci7294-9611226 024011Nurul SaufikaNo ratings yet
- s00134 022 06882 ZDocument18 pagess00134 022 06882 ZEmmanuel Hernandez SantiagoNo ratings yet
- Prevention of Dehydration in Hospital PatientsDocument6 pagesPrevention of Dehydration in Hospital PatientseatthescrollNo ratings yet
- DiabetesDocument15 pagesDiabetesJunior GonzalesNo ratings yet
- Safety ChecklistDocument8 pagesSafety ChecklistdharmaNo ratings yet
- The Effect of Intradialytic Aerobic Exercise On Dialysis Efficacy in Hemodialysis Patients: A Randomized Controlled TrialDocument5 pagesThe Effect of Intradialytic Aerobic Exercise On Dialysis Efficacy in Hemodialysis Patients: A Randomized Controlled TrialFitriatun NisaNo ratings yet
- Yuanita PanmaDocument6 pagesYuanita PanmaHagane TetsuNo ratings yet
- Advances in The Management of Pediatric Septic Shock: Old Questions, New AnswersDocument7 pagesAdvances in The Management of Pediatric Septic Shock: Old Questions, New AnswersSandip KumarNo ratings yet
- ST RD ST NDDocument25 pagesST RD ST NDdevanganduNo ratings yet
- Jurnal 16 inDocument11 pagesJurnal 16 inAn anonymousNo ratings yet
- Common Sense Approach To Managing SepsisDocument12 pagesCommon Sense Approach To Managing SepsiszepedrocorreiaNo ratings yet
- RMHP 14 1823Document9 pagesRMHP 14 1823Deny SyachputraNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Evaluation and Management of Dysphagia: An Evidence-Based ApproachFrom EverandEvaluation and Management of Dysphagia: An Evidence-Based ApproachDhyanesh A. PatelNo ratings yet
- Irctcs E-Ticketing Service Electronic Reservation Slip (Personal User)Document1 pageIrctcs E-Ticketing Service Electronic Reservation Slip (Personal User)Jay ParkheNo ratings yet
- Methods-Time Measurement: MODAPTS Technique. This Technique Was Introduced in 1966 byDocument2 pagesMethods-Time Measurement: MODAPTS Technique. This Technique Was Introduced in 1966 byChisom IkengwuNo ratings yet
- Activity - 2 - (Discretel) (A1)Document1 pageActivity - 2 - (Discretel) (A1)AnkitChutaniNo ratings yet
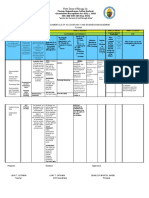
- Notre Dame of Masiag, Inc.: What Formativ e Question S Shall Lead To The Completi On of Efaa? ToDocument2 pagesNotre Dame of Masiag, Inc.: What Formativ e Question S Shall Lead To The Completi On of Efaa? ToLANY T. CATAMINNo ratings yet
- 03 Splash Park Design PDFDocument13 pages03 Splash Park Design PDFKikie Felis SilvestrisNo ratings yet
- Recruiting StrategiesDocument10 pagesRecruiting StrategiesAbhijeet PatraNo ratings yet
- Tổng Hợp Đề Thi Và Bài Mẫu IELTS Writing Năm 2021Document38 pagesTổng Hợp Đề Thi Và Bài Mẫu IELTS Writing Năm 2021Đoan Trang Trần NữNo ratings yet
- Forget No MoreDocument14 pagesForget No MoreSheeqin Mn100% (2)
- Talent Acquisition 2008 - Survey and Analysis of The Changing Recruiting Landscape PDFDocument20 pagesTalent Acquisition 2008 - Survey and Analysis of The Changing Recruiting Landscape PDFVaishnavi SivaNo ratings yet
- Expt. 8 Salivary DigestionDocument25 pagesExpt. 8 Salivary DigestionLESLIE JANE BALUYOS JALANo ratings yet
- Institutions and Regional Integration in AfricaDocument24 pagesInstitutions and Regional Integration in AfricaOrnela FabaniNo ratings yet
- Boiler WaterDocument70 pagesBoiler WaterDarius DsouzaNo ratings yet
- Full Download Elementary Statistics A Step by Step Approach Bluman 9Th Edition Solutions Manual PDFDocument49 pagesFull Download Elementary Statistics A Step by Step Approach Bluman 9Th Edition Solutions Manual PDFsteven.engelke246100% (21)
- Principles of Electricity PDFDocument371 pagesPrinciples of Electricity PDFJohn C. Stephens100% (5)
- Lewis Dot Structures #1Document3 pagesLewis Dot Structures #1Dustin MoenchNo ratings yet
- Free Bhel Transformer Book PDFDocument4 pagesFree Bhel Transformer Book PDFMilan ShahNo ratings yet
- Marketing Plan: GoldilocksDocument18 pagesMarketing Plan: GoldilocksAkhia Visitacion100% (1)
- Chapter 9 LectureDocument29 pagesChapter 9 Lectureinam vf100% (6)
- ABLRFD v1403 Summary RevisionsDocument2 pagesABLRFD v1403 Summary RevisionsMiguel AngelNo ratings yet
- Safety Grating CatalogDocument22 pagesSafety Grating CatalogzhukeeNo ratings yet
- Block 3Document17 pagesBlock 3Dianne ChristineNo ratings yet
- John Hagstrom: Philip BiggsDocument4 pagesJohn Hagstrom: Philip BiggsDarci HallNo ratings yet
- 3 2 A UnitconversionDocument6 pages3 2 A Unitconversionapi-312626334No ratings yet
- PetretecDocument8 pagesPetretecVenkatesan KrishnachariNo ratings yet
- Crane Design Guide 2Document8 pagesCrane Design Guide 2Mesfin Derbew0% (1)
- Chapter 10 - Eco LiteracyDocument15 pagesChapter 10 - Eco LiteracyMichelle Bandoquillo100% (1)
- Yealink Phone UserGuide PDFDocument2 pagesYealink Phone UserGuide PDFEric SmithNo ratings yet
- Chapter#3 - Assignmnet ProblemDocument36 pagesChapter#3 - Assignmnet ProblemHarishNo ratings yet
- Important Questions For MID I CNDocument14 pagesImportant Questions For MID I CN20H51A0540-NAKKA SREEKAR B.Tech CSE (2020-24)No ratings yet