Download as docx, pdf, or txt
You might also like
- Stravinsky Oedipus RexDocument131 pagesStravinsky Oedipus Rexkantee100% (16)
- GynaecologicalCancerChemoProtocols PDFDocument7 pagesGynaecologicalCancerChemoProtocols PDFRyan IlhamNo ratings yet
- Drug StudyDocument7 pagesDrug StudyKim GalamgamNo ratings yet
- ABAP FULL MaterialDocument128 pagesABAP FULL Materialanon_417818412100% (2)
- Basic Statistics Course at COURSERADocument17 pagesBasic Statistics Course at COURSERAYash Birla0% (1)
- Urological Cancer Chemotherapy ProtocolsDocument14 pagesUrological Cancer Chemotherapy ProtocolsPutrie WulandariNo ratings yet
- Liver TransplantationDocument6 pagesLiver TransplantationPriya0% (1)
- Agents For Influenza A and Respiratory VirusesDocument10 pagesAgents For Influenza A and Respiratory VirusesTrixia RodulfaNo ratings yet
- Pediatrics MS WordDocument13 pagesPediatrics MS WordSamhitha SharmaNo ratings yet
- HAART PresentationDocument27 pagesHAART PresentationNali peterNo ratings yet
- Autoimmune HepatitisDocument34 pagesAutoimmune HepatitisFUTURE DOCTORNo ratings yet
- Case PresentationDocument26 pagesCase Presentationhamid murtazaNo ratings yet
- Rancangan Bentuk Sediaan Farmasi Compatibility ModeDocument18 pagesRancangan Bentuk Sediaan Farmasi Compatibility ModeNully Andaretha SugiantoNo ratings yet
- Gamutin Drug Study-PediatricsDocument6 pagesGamutin Drug Study-PediatricsJhulia GamutinNo ratings yet
- Case Presentation MineDocument30 pagesCase Presentation MineAshman AshNo ratings yet
- Teachng DemoDocument32 pagesTeachng DemoNom NomNo ratings yet
- 7 - Case - ParasiticDocument18 pages7 - Case - Parasitickoteshwara raoNo ratings yet
- Therapeutic Regimens in HIVDocument36 pagesTherapeutic Regimens in HIVGail HoadNo ratings yet
- UTI and STIsDocument88 pagesUTI and STIsyejunNo ratings yet
- Drug Study Clindamycin, Ipatropium BromideDocument8 pagesDrug Study Clindamycin, Ipatropium Bromidepaupaulala100% (2)
- Antineoplastic AgentsDocument14 pagesAntineoplastic AgentsKarizza Zoette Ann AlcardeNo ratings yet
- Chemotherapy ProtocolsDocument6 pagesChemotherapy ProtocolsDenny LukasNo ratings yet
- Acquired Immunodeficiency Syndrome (Aids) : DescriptionDocument10 pagesAcquired Immunodeficiency Syndrome (Aids) : DescriptiongoyaNo ratings yet
- Altretamine: Drug DosageDocument16 pagesAltretamine: Drug DosagePrincess CruzNo ratings yet
- Uti in PregnancyDocument42 pagesUti in Pregnancydeepak122No ratings yet
- Screenshot 2020-03-20 at 08.25.44 PDFDocument10 pagesScreenshot 2020-03-20 at 08.25.44 PDFMiguel Angel Palacios FloresNo ratings yet
- Unit-4 - PHARMACOLOGY IIIDocument37 pagesUnit-4 - PHARMACOLOGY IIIShantanu RewatkarNo ratings yet
- 11'. Caz 1Document22 pages11'. Caz 1Iliescu Malina DianaNo ratings yet
- Drug Study On Mesalamine MercaptopurineDocument15 pagesDrug Study On Mesalamine Mercaptopurineسوما الشمريNo ratings yet
- Anti Tubercular AgentsDocument22 pagesAnti Tubercular AgentsKakai Ablanque LopozNo ratings yet
- Pharm Lecture 16 Infectious Disease Drugs Bjs EditsDocument56 pagesPharm Lecture 16 Infectious Disease Drugs Bjs Editsapi-737466463No ratings yet
- Medical Care: "Microbiology, Epidemiology, Clinical Manifestations, and Diagnosis of Leptospirosis"Document5 pagesMedical Care: "Microbiology, Epidemiology, Clinical Manifestations, and Diagnosis of Leptospirosis"Lyra LorcaNo ratings yet
- Cleveland Clinic Journal of Medicine 2013 BARON 354 9Document6 pagesCleveland Clinic Journal of Medicine 2013 BARON 354 9Stephanie PlascenciaNo ratings yet
- Aki Post Initiere Trat Tuberculo-StaticDocument8 pagesAki Post Initiere Trat Tuberculo-StaticDenisa Carmen ColiofNo ratings yet
- Pietermaritzburg Hospitals Complex Adult Tuberculosis Policy June 2008Document7 pagesPietermaritzburg Hospitals Complex Adult Tuberculosis Policy June 2008Mitchell GowNo ratings yet
- Acute Kidney Injury Case Study FinalDocument46 pagesAcute Kidney Injury Case Study FinalSalwa KaramanNo ratings yet
- JURNALDocument33 pagesJURNALrike aprilianaNo ratings yet
- JURNALDocument33 pagesJURNALrike aprilianaNo ratings yet
- Hiv Hepc PresentationDocument16 pagesHiv Hepc Presentationapi-748224285No ratings yet
- Part 2 OI 26 JUN2018Document88 pagesPart 2 OI 26 JUN2018Alimyon Abilar MontoloNo ratings yet
- Thera PresntationDocument5 pagesThera Presntationmxg3merNo ratings yet
- Systemic Lupus Erythematosus: By: DR Iqra AmjadDocument21 pagesSystemic Lupus Erythematosus: By: DR Iqra AmjadShahmeer AliNo ratings yet
- Chemical Pathology II HIV AIDSDocument33 pagesChemical Pathology II HIV AIDSSimeon AdebisiNo ratings yet
- Xi - Drug Study: Drugs Action Indication Contraindication Adverse Effect Nursing ConsiderationDocument18 pagesXi - Drug Study: Drugs Action Indication Contraindication Adverse Effect Nursing ConsiderationlicservernoidaNo ratings yet
- Indications of ICU Admission and ICU Management of COVID 19 NEWDocument27 pagesIndications of ICU Admission and ICU Management of COVID 19 NEWMidhat FatmaNo ratings yet
- Antimalarial Drugs: Presenter Basil Mupita Rgn/BscneDocument35 pagesAntimalarial Drugs: Presenter Basil Mupita Rgn/BscneTapiwaNo ratings yet
- Ziad Aro, MD Internal MedicineDocument100 pagesZiad Aro, MD Internal MedicineAli Aborges Jr.No ratings yet
- NURS360 Pyelonephritis Care MapDocument5 pagesNURS360 Pyelonephritis Care MapChristine RombawaNo ratings yet
- Ceftaroline Teflaro CefotaximeDocument3 pagesCeftaroline Teflaro CefotaximeKristi WrayNo ratings yet
- Acute Lymphoid LeukemiaDocument41 pagesAcute Lymphoid Leukemiaummi ulfahNo ratings yet
- FaciitisDocument17 pagesFaciitisdalaginding clophNo ratings yet
- Acute PancreatitisDocument66 pagesAcute PancreatitisSamina GulNo ratings yet
- D. Antiviral Antiprotozoal AntihilmenticsDocument31 pagesD. Antiviral Antiprotozoal AntihilmenticsKim Shyen BontuyanNo ratings yet
- Additional Pharma CardsDocument21 pagesAdditional Pharma CardsBrilie Karl Viray100% (1)
- Management of Adult Febrile Neutropenia: 15011500-10123 99 Street Edmonton, Alberta T5J 3H1Document4 pagesManagement of Adult Febrile Neutropenia: 15011500-10123 99 Street Edmonton, Alberta T5J 3H1Tio Prima SNo ratings yet
- Management of SepsisDocument34 pagesManagement of SepsisTamim IshtiaqueNo ratings yet
- Drugs Study, Nursing, PreoperativeDocument9 pagesDrugs Study, Nursing, PreoperativeKevin Sam AguirreNo ratings yet
- Pharmacotherapy of TuberculosisDocument31 pagesPharmacotherapy of TuberculosisjabirNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Principles in UTIDocument36 pagesPrinciples in UTIMaydhista PoetriNo ratings yet
- Nicardipine (: ClassificationDocument14 pagesNicardipine (: ClassificationWilliam CiferNo ratings yet
- Short Case TBDocument15 pagesShort Case TBLateefah TalalNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
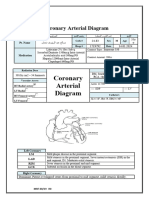
- Coronary Arterial DiagramDocument3 pagesCoronary Arterial Diagramshamaamo19No ratings yet
- Partial Embolization of Splenic ArteryDocument2 pagesPartial Embolization of Splenic Arteryshamaamo19No ratings yet
- Hamda Mohammad Sa'adeh - PCI Final ReportDocument4 pagesHamda Mohammad Sa'adeh - PCI Final Reportshamaamo19No ratings yet
- 2022 ESC VASCD Guidelines Official Slide Set - Final - ProtectedDocument23 pages2022 ESC VASCD Guidelines Official Slide Set - Final - Protectedshamaamo19No ratings yet
- Valvular Disease1Document35 pagesValvular Disease1shamaamo19No ratings yet
- AhlamDocument3 pagesAhlamshamaamo19No ratings yet
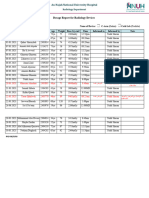
- Dosage Report For Cath Lab Patients in 03.2023Document2 pagesDosage Report For Cath Lab Patients in 03.2023shamaamo19No ratings yet
- NstemiDocument6 pagesNstemishamaamo19No ratings yet
- ProgressNote - 2313061 - Sat Apr 13 15 - 19 - 16 IDT 2024Document5 pagesProgressNote - 2313061 - Sat Apr 13 15 - 19 - 16 IDT 2024shamaamo19No ratings yet
- unstable-angina جاهز لللعرضDocument9 pagesunstable-angina جاهز لللعرضshamaamo19No ratings yet
- جاهز للعرضDocument38 pagesجاهز للعرضshamaamo19No ratings yet
- 10.women LeadershipDocument26 pages10.women LeadershipAbhir Raj ShrivastavaNo ratings yet
- 14740x 2016 Syllabus and Reading ListDocument11 pages14740x 2016 Syllabus and Reading ListFaysal HaqueNo ratings yet
- Bacillus Subtilis Strains Isolated From Different Habitats: Amicoumacin Antibiotic Production and Genetic Diversity ofDocument7 pagesBacillus Subtilis Strains Isolated From Different Habitats: Amicoumacin Antibiotic Production and Genetic Diversity ofwisorNo ratings yet
- Cornerstones of Managerial Accounting Canadian 3rd Edition Mowen Solutions ManualDocument35 pagesCornerstones of Managerial Accounting Canadian 3rd Edition Mowen Solutions ManualElizabethMackxwps100% (48)
- Lab 9: XSS Attack Aastha Yadav (Ayadav02@syr - Edu) SUID: 831570679Document19 pagesLab 9: XSS Attack Aastha Yadav (Ayadav02@syr - Edu) SUID: 831570679smurfeuwsingedNo ratings yet
- Pelman V McDonalds SDNYDocument65 pagesPelman V McDonalds SDNYfoodfightNo ratings yet
- Marki DuvanaDocument27 pagesMarki DuvanamijpedjapedjaNo ratings yet
- Heaaven PR2Document52 pagesHeaaven PR2bobmercadowsNo ratings yet
- Bagaimana Pendalaman Keuangan Dan Cadangan Devisa Mempengaruhi Stabilitas Nilai Tukar Di NEGARA EMERGING MARKET? (Pendekatan Panel ARDL)Document9 pagesBagaimana Pendalaman Keuangan Dan Cadangan Devisa Mempengaruhi Stabilitas Nilai Tukar Di NEGARA EMERGING MARKET? (Pendekatan Panel ARDL)Yanri DayaNo ratings yet
- Manual de Instruções Marantz SR-7500 DFU - 00 - CoverDocument56 pagesManual de Instruções Marantz SR-7500 DFU - 00 - CoverAntonio VidalNo ratings yet
- Sujok Accupressure - Figures: IndexDocument14 pagesSujok Accupressure - Figures: IndexSiti latifahNo ratings yet
- Geometry CH 1 Test Review BDocument8 pagesGeometry CH 1 Test Review Balex montemayoresNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakanarulianNo ratings yet
- Air France vs. Carrascoso, 18 SCRA 155, No. L-21438 September 28, 1966Document5 pagesAir France vs. Carrascoso, 18 SCRA 155, No. L-21438 September 28, 1966Lyka Angelique CisnerosNo ratings yet
- Brand Guidelines: The Brand Book For Onedesk - 2020Document14 pagesBrand Guidelines: The Brand Book For Onedesk - 2020RacksonNo ratings yet
- FPEMDocument5 pagesFPEMJaya Chandra ReddyNo ratings yet
- District Industries Centre (DIC)Document17 pagesDistrict Industries Centre (DIC)Lionel El BarcaNo ratings yet
- Administradora de Estaciones de Servicio Sa de CV: BPJURIH 10852 76100Document1 pageAdministradora de Estaciones de Servicio Sa de CV: BPJURIH 10852 76100gordoasesinoNo ratings yet
- CFLM1 Mendoza 123Document32 pagesCFLM1 Mendoza 123ShyyNo ratings yet
- Activa Product ImprovementsDocument17 pagesActiva Product ImprovementsadityatfiNo ratings yet
- Canon Irc3200 Parts CatalogDocument313 pagesCanon Irc3200 Parts CatalogStratis SiderisNo ratings yet
- Rhonda Wells V Rachel GrahamDocument5 pagesRhonda Wells V Rachel GrahamRobert WilonskyNo ratings yet
- SLA GuideDocument205 pagesSLA GuidePeng Chiew Low100% (1)
- FoodBalt 2017 Abstract BookDocument140 pagesFoodBalt 2017 Abstract BookEngr Muhammad IrfanNo ratings yet
- Why We Need The Individual MandateDocument3 pagesWhy We Need The Individual MandateCenter for American ProgressNo ratings yet
- Constitutional InterpretationDocument13 pagesConstitutional InterpretationAndrew SekayiriNo ratings yet
- Beginners Guide To Voip WP 2016Document13 pagesBeginners Guide To Voip WP 2016sharnobyNo ratings yet