Download as pdf or txt
You might also like
- NCP Hydrocephalus With RationaleDocument42 pagesNCP Hydrocephalus With RationaleJulienne Sanchez-Salazar80% (15)
- Inotropes and VasopressorsDocument63 pagesInotropes and VasopressorsCraig DuHaney50% (2)
- Makali Waswa Student - Heritagehs - Furlough-U3l6 Student GuideDocument7 pagesMakali Waswa Student - Heritagehs - Furlough-U3l6 Student Guideapi-536237767No ratings yet
- INOTROPESDocument28 pagesINOTROPESsinghal297% (30)
- Cardio Tonic DrugDocument25 pagesCardio Tonic DrugNistha MudgilNo ratings yet
- Congestive Cardiac FailureDocument21 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Pharmacology Lecture - 15 Inotropic DrugsDocument3 pagesPharmacology Lecture - 15 Inotropic DrugsChris Queiklin100% (1)
- Medicinal Chemistry 2 IMP QUESTION ANSWER @DBATUPHARMDocument25 pagesMedicinal Chemistry 2 IMP QUESTION ANSWER @DBATUPHARMgautampatil305No ratings yet
- 2 Pharmacodynamics FinalDocument31 pages2 Pharmacodynamics FinalTanvir FahimNo ratings yet
- 1.CVS DrugsDocument98 pages1.CVS DrugsHarshika KDGNo ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- L5 Heart Failure-Dr. Yagub S SalehDocument7 pagesL5 Heart Failure-Dr. Yagub S Salehnusaiba.alobaidyNo ratings yet
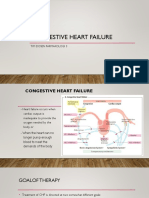
- CONGESTIVE HEART FAILURE - New-1Document32 pagesCONGESTIVE HEART FAILURE - New-1Agus SuprionoNo ratings yet
- Heat Failure DrugsDocument8 pagesHeat Failure DrugsDaniel MwiluNo ratings yet
- Pharmacology MnemonicsDocument17 pagesPharmacology MnemonicsIk-ik MiralNo ratings yet
- Congestive Cardiac FailureDocument27 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Helping Material For PrometricDocument48 pagesHelping Material For PrometricRPh FarhatainNo ratings yet
- Pharmacology Nursing MnemonicsDocument23 pagesPharmacology Nursing MnemonicsJoanne Bernadette Aguilar100% (1)
- Chapter - 024 Heart Failure DrugsDocument7 pagesChapter - 024 Heart Failure DrugsthubtendrolmaNo ratings yet
- Modul Drugs Used in Congestive Heart Failure 11 Nov 2010Document12 pagesModul Drugs Used in Congestive Heart Failure 11 Nov 2010Dian NugraNo ratings yet
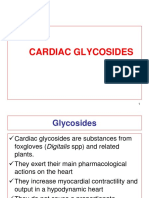
- Cardiac GlycosidesDocument30 pagesCardiac GlycosidesFrancisNo ratings yet
- Lesson 1 Cardiac Glycosides, Antianginals, and Antidysrhythmics - AntiarrhythmmicsDocument40 pagesLesson 1 Cardiac Glycosides, Antianginals, and Antidysrhythmics - AntiarrhythmmicsXiamen Magsino NolascoNo ratings yet
- Pharmacology Nursing Mnemonics Amp TipsDocument15 pagesPharmacology Nursing Mnemonics Amp TipsHenrie Angelie TamNo ratings yet
- Drugs Acting On CVS-2014Document36 pagesDrugs Acting On CVS-2014كسلان اكتب اسميNo ratings yet
- Agentes CardiovascularesDocument47 pagesAgentes CardiovascularesSUSANA RAQUEL GUARDADO GOMEZNo ratings yet
- 5-Heart FailureDocument12 pages5-Heart FailureJericho De GuzmanNo ratings yet
- Review and Update On VasopressorsDocument9 pagesReview and Update On VasopressorspunkgatitNo ratings yet
- Pharmacology Notes: By: Khurram AbbasDocument48 pagesPharmacology Notes: By: Khurram AbbasAsma AnjumNo ratings yet
- 3 DrugsforHeartFailureDocument60 pages3 DrugsforHeartFailureJov CelNo ratings yet
- Pharmacology ReviersDocument5 pagesPharmacology ReviersNeisha Halil VillarealNo ratings yet
- Antihypertensive AgentsDocument52 pagesAntihypertensive Agentssameena ramzanNo ratings yet
- Pharmacodynamics (How The Drugs Affect The Body) : PharmacologyDocument35 pagesPharmacodynamics (How The Drugs Affect The Body) : PharmacologyNat Lynne Distor TrondilloNo ratings yet
- PharmaDocument53 pagesPharmaOluwafeyikemi WilliamsNo ratings yet
- LECTURE 9 Positive InotropicDocument5 pagesLECTURE 9 Positive InotropicanaNo ratings yet
- Pharma 2016Document48 pagesPharma 2016backupuoload85No ratings yet
- ART Rugs and Nfusions: A. PolicyDocument7 pagesART Rugs and Nfusions: A. PolicyZoelNo ratings yet
- Pharmacology ReviewersDocument5 pagesPharmacology ReviewersNeisha Halil VillarealNo ratings yet
- By Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4Document4 pagesBy Duy Thai, 1997: Pharmacology Semester 1 Page 1 of 4ravi2likeNo ratings yet
- Module No. 4 Cardiovascular DrugsDocument8 pagesModule No. 4 Cardiovascular DrugsJellie An TalattagNo ratings yet
- E Kart DrugsDocument3 pagesE Kart DrugsNichole CastleNo ratings yet
- SympathomimeticDocument56 pagesSympathomimeticvarish0% (1)
- L2 Hypertension 2 - Dr. Yagub S SalehDocument4 pagesL2 Hypertension 2 - Dr. Yagub S Salehnusaiba.alobaidyNo ratings yet
- BNSC CVSDocument37 pagesBNSC CVSosewapeace14No ratings yet
- Cardiovascular Pharmacology PDFDocument20 pagesCardiovascular Pharmacology PDFMelanie PrinceNo ratings yet
- Anti Arrhythmics DrugsDocument16 pagesAnti Arrhythmics DrugsSaima ParveenNo ratings yet
- Pharmacology Nursing GuideDocument102 pagesPharmacology Nursing GuideRene Jesus T. AcostaNo ratings yet
- Heart Failure TutorialDocument1 pageHeart Failure TutorialAbdul MosheenNo ratings yet
- Obat Yang Bekerja Pada Sistem KardiovaskulerDocument18 pagesObat Yang Bekerja Pada Sistem KardiovaskulerMuhammad IkbalNo ratings yet
- Lec 2 Heart Failure, Angina and Arryth2Document19 pagesLec 2 Heart Failure, Angina and Arryth2Adel AlomarNo ratings yet
- Module 7 Pharmacology of Autocoids-1Document35 pagesModule 7 Pharmacology of Autocoids-1Cyrill sorianoNo ratings yet
- 7,8 - Antihypertensive DrugsDocument10 pages7,8 - Antihypertensive DrugsHusniya MehamedNo ratings yet
- Cardiovascular System 2Document8 pagesCardiovascular System 2محمد علي حميدNo ratings yet
- Parasympathetic Nervous System: Uptake of CholineDocument16 pagesParasympathetic Nervous System: Uptake of Cholinegksah711No ratings yet
- CHFDocument11 pagesCHFGwendolyn Talahiban LusaraNo ratings yet
- Terapi Farmakologi Gagal Jantung - Sept - 2020Document58 pagesTerapi Farmakologi Gagal Jantung - Sept - 2020FAUZAN ILHAM PRATAMANo ratings yet
- Pharma CVS LectureDocument14 pagesPharma CVS Lectureبصيص اليقينNo ratings yet
- Drugs Used in Heart FailureDocument27 pagesDrugs Used in Heart Failurealeah morenoNo ratings yet
- PharmTest3 StudyGuideDocument9 pagesPharmTest3 StudyGuideTara Bickford ManisNo ratings yet
- Pharmacology Pgi Compre Recall & Ratio December 2017: Cardiovascular DrugsDocument16 pagesPharmacology Pgi Compre Recall & Ratio December 2017: Cardiovascular DrugsSaravanan DevarajNo ratings yet
- Drugs For Treating Heart FailureDocument40 pagesDrugs For Treating Heart FailureMbah GapinbissiNo ratings yet
- 9 Drugs Affecting Angina PectorisDocument3 pages9 Drugs Affecting Angina PectoristiaraNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Organizational Life-Cycle: The Characteristics of Developmental Stages in Russian Companies Created From ScratchDocument22 pagesOrganizational Life-Cycle: The Characteristics of Developmental Stages in Russian Companies Created From Scratchsuhas.kandeNo ratings yet
- Platform ConfigurationDocument67 pagesPlatform Configurationsuhas.kandeNo ratings yet
- SAP Digital Vehicle HuDocument46 pagesSAP Digital Vehicle Husuhas.kandeNo ratings yet
- Administration Guide For Intelligent SituationDocument18 pagesAdministration Guide For Intelligent Situationsuhas.kandeNo ratings yet
- Renal Scintigraphy (Renal Radionuclide Scan) : Tc-99m DMSA Tc-99m MAG3 Tc-99m DTPADocument20 pagesRenal Scintigraphy (Renal Radionuclide Scan) : Tc-99m DMSA Tc-99m MAG3 Tc-99m DTPA黃昱睿No ratings yet
- Quiz 1 - MacromoleculesDocument2 pagesQuiz 1 - MacromoleculesEricha Palaypay EmpaynadoNo ratings yet
- Formulation and Evaluation of Herbal Sanitizer PDFDocument4 pagesFormulation and Evaluation of Herbal Sanitizer PDFWikoo ENo ratings yet
- Proton Pump Inhibitors PDFDocument4 pagesProton Pump Inhibitors PDFBintoo SharmaNo ratings yet
- Central Nervous System Pathology: Presented byDocument70 pagesCentral Nervous System Pathology: Presented byNicholasNo ratings yet
- Dynamic Lipidome Alterations Associated With Human Health, Disease and AgeingDocument22 pagesDynamic Lipidome Alterations Associated With Human Health, Disease and AgeingMichael ArkangyalNo ratings yet
- Part B: Multiple Choice Questions Time Limit: 20 25 Minutes To Test or Not To Test? Self-Monitoring of Blood Glucose in Patients With Type 2 DiabetesDocument7 pagesPart B: Multiple Choice Questions Time Limit: 20 25 Minutes To Test or Not To Test? Self-Monitoring of Blood Glucose in Patients With Type 2 DiabetesAnushree MPNo ratings yet
- Parenting The Difficult TemperamentDocument3 pagesParenting The Difficult Temperamentjackpot_ipNo ratings yet
- Service Manual Humaclot ProDocument8 pagesService Manual Humaclot ProHuy Trung GiápNo ratings yet
- EpistasisDocument26 pagesEpistasisy4heherNo ratings yet
- AM-783 Agricultural Machinery Design: "Problem Statement With Conceptual Design"Document6 pagesAM-783 Agricultural Machinery Design: "Problem Statement With Conceptual Design"HelenGraceP.BugnayNo ratings yet
- Schistura ThavoneiDocument9 pagesSchistura ThavoneiSubhadra LaimayumNo ratings yet
- Solute Solvent Interaction Studies of Amino Acids in Aqueous Tertiary-Butyl Alcohol SolutionsDocument6 pagesSolute Solvent Interaction Studies of Amino Acids in Aqueous Tertiary-Butyl Alcohol SolutionsNag28rajNo ratings yet
- 8.2 Transport of Oxygen and Carbon DioxideDocument13 pages8.2 Transport of Oxygen and Carbon DioxideFarista KabirNo ratings yet
- Magnesium Calcium PDFDocument3 pagesMagnesium Calcium PDFokikwmNo ratings yet
- M. Boni, V. Denaro (Auth.), Professor Pierre Kehr M.D., Priv.-Doz. Dr. Med. Andreas Weidner (Eds.) - Cervical Spine I - Strasbourg 1985-Springer-Verlag Wien (1986) PDFDocument342 pagesM. Boni, V. Denaro (Auth.), Professor Pierre Kehr M.D., Priv.-Doz. Dr. Med. Andreas Weidner (Eds.) - Cervical Spine I - Strasbourg 1985-Springer-Verlag Wien (1986) PDFLorena BurdujocNo ratings yet
- Significance of Microscopy in Cell BiologyDocument10 pagesSignificance of Microscopy in Cell BiologyAbeer FatimaNo ratings yet
- Saat 1438Document54 pagesSaat 1438Moustapha MneimnehNo ratings yet
- The World of Mangoes and TomatoesDocument12 pagesThe World of Mangoes and Tomatoesferanmi.alaraNo ratings yet
- Midlands State University Department of Applied Biosciences and BiotechnologyDocument2 pagesMidlands State University Department of Applied Biosciences and BiotechnologytanatswaNo ratings yet
- Class-10 Revision Test - NutritionDocument4 pagesClass-10 Revision Test - NutritionVarshini PeraNo ratings yet
- HHS Public Access: Origins of Glial Cell Populations in The Insect Nervous SystemDocument18 pagesHHS Public Access: Origins of Glial Cell Populations in The Insect Nervous SystemHelena QuintNo ratings yet
- Full Ebook of Living Science 7 2022Nd Edition A C Sahgal Online PDF All ChapterDocument69 pagesFull Ebook of Living Science 7 2022Nd Edition A C Sahgal Online PDF All Chapterrandallschlemmer637072100% (5)
- ASTM Page For Degradable PlasticsDocument2 pagesASTM Page For Degradable Plasticsjohnsygeorge1978No ratings yet
- Dragon Fruit Futre FruitDocument14 pagesDragon Fruit Futre FruithkNo ratings yet
- Isolation and Characterization of Bacteria From Coal Mines of Dara Adam Khel PakistanDocument10 pagesIsolation and Characterization of Bacteria From Coal Mines of Dara Adam Khel PakistanТаймурАбдуллахNo ratings yet
- Blood Gas Analysis: - Arterial Blood Gases MeasuresDocument39 pagesBlood Gas Analysis: - Arterial Blood Gases Measuresapi-19641337No ratings yet
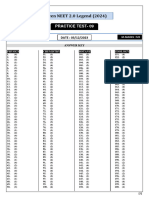
- Practice Test 09 - Hint & Solution (Legend) - Yakeen NEET 2.0 2024Document12 pagesPractice Test 09 - Hint & Solution (Legend) - Yakeen NEET 2.0 2024akhtartanveer119No ratings yet