
Employment Verification Form T-122, 2022-23
Employment Verification Form T-122, 2022-23
You might also like
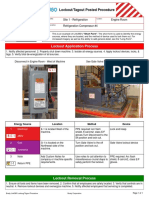
- Brady Link360 Lockout Tagout Short FormDocument2 pagesBrady Link360 Lockout Tagout Short FormReynaldo GrantNo ratings yet
- Preparing For The WorkKeys AssessmentsDocument68 pagesPreparing For The WorkKeys Assessmentszon-x50% (2)
- 2020 Application For Deferral of Tuition Fee PaymentDocument2 pages2020 Application For Deferral of Tuition Fee PaymentBao Phong TranNo ratings yet
- 2a WINDALCO Local Scholarship Application Form 2021Document4 pages2a WINDALCO Local Scholarship Application Form 2021CHRISTOPHER SCALE100% (1)
- Planning Forms FM SGO PLA 001Document2 pagesPlanning Forms FM SGO PLA 001Venilyn April Barrientos100% (2)
- Licensing & Registration Rules - Engineering - Philippines - CCS 44Document30 pagesLicensing & Registration Rules - Engineering - Philippines - CCS 44welwelNo ratings yet
- All About ToastmastersDocument2 pagesAll About ToastmastersDebashis MajumdarNo ratings yet
- Program Withdrawal Form 2021-Digital Naresh ShresthaDocument1 pageProgram Withdrawal Form 2021-Digital Naresh ShresthagantadaiNo ratings yet
- Sussex County Superintendent Roundtable Association Scholarship ApplicationDocument3 pagesSussex County Superintendent Roundtable Association Scholarship ApplicationdjdmdnNo ratings yet
- Education Experience Verification FormDocument2 pagesEducation Experience Verification FormROCKNo ratings yet
- Extension in Payment of FeeDocument3 pagesExtension in Payment of FeeAmrit Pal SinghNo ratings yet
- 710 James Robertson Parkway - Andrew Johnson Tower, 12 Floor - Nashville, TN 37243Document2 pages710 James Robertson Parkway - Andrew Johnson Tower, 12 Floor - Nashville, TN 37243nagu323No ratings yet
- Description: Tags: DLB0341AttDocument1 pageDescription: Tags: DLB0341Attanon-404473No ratings yet
- Description: Tags: DLB0341AttDocument1 pageDescription: Tags: DLB0341Attanon-952530No ratings yet
- Instructions:: Part 1-Personal InformationDocument7 pagesInstructions:: Part 1-Personal InformationISLAND NATANYANo ratings yet
- EDSP Application FormDocument4 pagesEDSP Application FormDave MillaresNo ratings yet
- SSS ApplicationDocument4 pagesSSS ApplicationPamela ComerNo ratings yet
- F 3LE Personal History Statement1.2021Document17 pagesF 3LE Personal History Statement1.2021James LewisNo ratings yet
- Vivian Scott Student Application FormDocument3 pagesVivian Scott Student Application Formapi-337237932No ratings yet
- Application For Admission FormDocument2 pagesApplication For Admission Formzacksr34No ratings yet
- 20200228-2020 GESP Application Form PDFDocument2 pages20200228-2020 GESP Application Form PDFMaria MacelNo ratings yet
- Employee Personal Profile 1Document2 pagesEmployee Personal Profile 1zagham.berksNo ratings yet
- Permit To StudyDocument2 pagesPermit To StudyJaidee Ann PerezNo ratings yet
- Limited Special Admission Application 04212013Document3 pagesLimited Special Admission Application 04212013jemccourt7129No ratings yet
- Undocuscholarhip 2014Document5 pagesUndocuscholarhip 2014api-251764893No ratings yet
- Application FormDocument6 pagesApplication FormAkshay SharmaNo ratings yet
- Department of Education: Request Permit To StudyDocument1 pageDepartment of Education: Request Permit To Studydolly kate cagadasNo ratings yet
- Private School M & E Report Form - NEWDocument4 pagesPrivate School M & E Report Form - NEWNer Mangaron100% (1)
- Application Form - Entrance ExamDocument1 pageApplication Form - Entrance Examlovely bless ardonNo ratings yet
- Seattle Schools Service-Learning Form and ReflectionDocument2 pagesSeattle Schools Service-Learning Form and Reflectionsilas StatenNo ratings yet
- EQUIVALENT RECORD FORM ERF Revised 2023Document3 pagesEQUIVALENT RECORD FORM ERF Revised 2023JUNEI LIZA SAMPANINo ratings yet
- StlouisDocument2 pagesStlouisr0kimNo ratings yet
- 3 - SOE Data and VerificationDocument1 page3 - SOE Data and VerificationWhitney DunlapNo ratings yet
- Title I Grant Request For Services v5 12 15 092Document8 pagesTitle I Grant Request For Services v5 12 15 092api-134134588No ratings yet
- Volunteer Form SampleDocument2 pagesVolunteer Form SampleJeffrey BlissiNo ratings yet
- 02 - Youth COMEA Editable EnclosuresDocument7 pages02 - Youth COMEA Editable EnclosuresPrincess Lynn PaduaNo ratings yet
- Last Day Request Form 6.2017Document2 pagesLast Day Request Form 6.2017Raphael AndradeNo ratings yet
- Eskwela Davao Application Form (Blank)Document2 pagesEskwela Davao Application Form (Blank)Aljeania Marie M. MolialNo ratings yet
- Eskwela Davao Application Form (Blank)Document2 pagesEskwela Davao Application Form (Blank)no one33% (3)
- Usc Recommendation FormDocument3 pagesUsc Recommendation FormEARL JOHN A BESARIONo ratings yet
- Tampa Foreign Language Center: 9309 N Florida Ave Suite 109 Tampa, FL 33612 PH (813) 988-7900 FAX (813) 980-3751Document3 pagesTampa Foreign Language Center: 9309 N Florida Ave Suite 109 Tampa, FL 33612 PH (813) 988-7900 FAX (813) 980-3751Jt DouglassNo ratings yet
- Independent Contractor ChecklistDocument2 pagesIndependent Contractor ChecklistwellhellotheresexxayNo ratings yet
- GSIS Educational Subsidy 2021-2022Document2 pagesGSIS Educational Subsidy 2021-2022Noe Carillo CabusaoNo ratings yet
- TA FormDocument2 pagesTA FormEdwin Lopez100% (1)
- South Dakota Board of Regents Undergraduate Student Readmission FormDocument1 pageSouth Dakota Board of Regents Undergraduate Student Readmission FormanttenehNo ratings yet
- Permit To Study NewDocument2 pagesPermit To Study Newailene banuelosNo ratings yet
- Honors Program: Florida State College at JacksonvilleDocument3 pagesHonors Program: Florida State College at JacksonvillemortensenkNo ratings yet
- Staff Recruitment FormDocument3 pagesStaff Recruitment FormArmie FisherNo ratings yet
- KwaZulu Natal Department of Transport Bursary Application FormDocument8 pagesKwaZulu Natal Department of Transport Bursary Application FormMandisa ZibulaNo ratings yet
- Application FormDocument2 pagesApplication Formemmanuel musundireNo ratings yet
- Board Member Application November 2020Document3 pagesBoard Member Application November 2020Graham FilesNo ratings yet
- CCSD Acceleration Request FormDocument1 pageCCSD Acceleration Request Formapi-637800717No ratings yet
- MKU Internal Scholarship Application Form 2023Document9 pagesMKU Internal Scholarship Application Form 2023mugambioscar47No ratings yet
- Memorial Go-Kart Inc.: 5308 Hwy 175 Hartford, WI 53027 262-644-8375Document5 pagesMemorial Go-Kart Inc.: 5308 Hwy 175 Hartford, WI 53027 262-644-8375Hafiezul HassanNo ratings yet
- Consent To TestDocument2 pagesConsent To Testapi-260986714No ratings yet
- Student Academic Appointment Application FormDocument2 pagesStudent Academic Appointment Application FormSais AlasNo ratings yet
- Graduate Information FormDocument1 pageGraduate Information Formapi-290603068No ratings yet
- ME Tools For Mid Year BreakDocument3 pagesME Tools For Mid Year BreakLoidaCarameNo ratings yet
- Permit To StudyDocument2 pagesPermit To StudyJerome SalasNo ratings yet
- Where To Locate The CRN: Class Scheduling FormDocument1 pageWhere To Locate The CRN: Class Scheduling FormBen CamarenoNo ratings yet
- CFWP Waiver BeneficiaryDocument1 pageCFWP Waiver BeneficiaryDominador M. Mejia IIINo ratings yet
- Grade 12Document3 pagesGrade 12browntayan61No ratings yet
- Service Hours Log-Volunteer Approval FormDocument2 pagesService Hours Log-Volunteer Approval FormkylikatzNo ratings yet
- Types of RisksDocument3 pagesTypes of RisksayushdixitNo ratings yet
- How To Run Kalonga MillingDocument11 pagesHow To Run Kalonga MillingDerickMwansa100% (1)
- Summer Training Report On LT Foods Bharat Sachdeva (3) YearDocument81 pagesSummer Training Report On LT Foods Bharat Sachdeva (3) Yearbharat sachdeva50% (2)
- Layoffs, Coping, and Commitment: Impact of Layoffs On Employees and Strategies Used in Coping With LayoffsDocument6 pagesLayoffs, Coping, and Commitment: Impact of Layoffs On Employees and Strategies Used in Coping With LayoffsMohammad MansourNo ratings yet
- BSBDIV501 Aus Accountancy Set For Skilling Program Documents.v1.0Document6 pagesBSBDIV501 Aus Accountancy Set For Skilling Program Documents.v1.0Aakash SharmaNo ratings yet
- Study Guide: Chapter 3: Stakeholders and Corporate Social ResponsibilityDocument2 pagesStudy Guide: Chapter 3: Stakeholders and Corporate Social ResponsibilityChitose HarukiNo ratings yet
- 09 Social Science Key Notes Eco Ch1 People As ResourcesDocument3 pages09 Social Science Key Notes Eco Ch1 People As ResourcesSACHIN TAAK50% (2)
- Mayank Mani - SAP SD - Project Implementation Experience 4.9 Yrs - BangaloreDocument3 pagesMayank Mani - SAP SD - Project Implementation Experience 4.9 Yrs - BangaloreMayank ManiNo ratings yet
- Laredo City Manager ContractDocument7 pagesLaredo City Manager ContractCarlos YNo ratings yet
- 7 DOLE Form - AEDRDocument1 page7 DOLE Form - AEDRJeford Mendaros SalagubangNo ratings yet
- Free Resume Review OnlineDocument6 pagesFree Resume Review Onlineguv0k1jemen3100% (2)
- Paper 2: Business Laws and Business Correspondence and Reporting Section A: Business LawsDocument14 pagesPaper 2: Business Laws and Business Correspondence and Reporting Section A: Business LawsNitesh PatelNo ratings yet
- Opportunities 2020Document7 pagesOpportunities 2020raj xNo ratings yet
- Bananas, Beaches AND Bases: Feminism in IRDocument11 pagesBananas, Beaches AND Bases: Feminism in IRAlyanna CabralNo ratings yet
- Chapter 8 - Understanding Individual BehaviorDocument18 pagesChapter 8 - Understanding Individual BehaviorMy KiềuNo ratings yet
- Purchasing Policy and Procedures-Knowledge How ToDocument39 pagesPurchasing Policy and Procedures-Knowledge How ToPrabhakar Chowdary Chintala100% (1)
- VibinrajDocument5 pagesVibinrajvibinrajNo ratings yet
- W 2Document6 pagesW 2prads1259No ratings yet
- Curriculum Vitae Sample College StudentDocument5 pagesCurriculum Vitae Sample College Studentzxlzszwhf100% (1)
- NRS 440 VN Week 3Document2 pagesNRS 440 VN Week 3Patrick W KagaiNo ratings yet
- MSDs at Port Wine Vines Cultivation - PTDocument8 pagesMSDs at Port Wine Vines Cultivation - PTnmmartinsaNo ratings yet
- Presentation 4Document17 pagesPresentation 4Gochi GamingNo ratings yet
- Ailet: Section Topic No. of QuestionsDocument22 pagesAilet: Section Topic No. of QuestionsabcNo ratings yet
- Economic Terms Glossary PDFDocument12 pagesEconomic Terms Glossary PDFannayaNo ratings yet
- CLFM 2 - Chapter 4 5 - DocxDocument12 pagesCLFM 2 - Chapter 4 5 - DocxKizzy Flores Victorio100% (1)
- Minimum Wages Hosiery Manufactory 2019 - 2020Document1 pageMinimum Wages Hosiery Manufactory 2019 - 2020Adhavan M AnnathuraiNo ratings yet
























































































Download as pdf or txt
You might also like
- Brady Link360 Lockout Tagout Short FormDocument2 pagesBrady Link360 Lockout Tagout Short FormReynaldo GrantNo ratings yet
- Preparing For The WorkKeys AssessmentsDocument68 pagesPreparing For The WorkKeys Assessmentszon-x50% (2)
- 2020 Application For Deferral of Tuition Fee PaymentDocument2 pages2020 Application For Deferral of Tuition Fee PaymentBao Phong TranNo ratings yet
- 2a WINDALCO Local Scholarship Application Form 2021Document4 pages2a WINDALCO Local Scholarship Application Form 2021CHRISTOPHER SCALE100% (1)
- Planning Forms FM SGO PLA 001Document2 pagesPlanning Forms FM SGO PLA 001Venilyn April Barrientos100% (2)
- Licensing & Registration Rules - Engineering - Philippines - CCS 44Document30 pagesLicensing & Registration Rules - Engineering - Philippines - CCS 44welwelNo ratings yet
- All About ToastmastersDocument2 pagesAll About ToastmastersDebashis MajumdarNo ratings yet
- Program Withdrawal Form 2021-Digital Naresh ShresthaDocument1 pageProgram Withdrawal Form 2021-Digital Naresh ShresthagantadaiNo ratings yet
- Sussex County Superintendent Roundtable Association Scholarship ApplicationDocument3 pagesSussex County Superintendent Roundtable Association Scholarship ApplicationdjdmdnNo ratings yet
- Education Experience Verification FormDocument2 pagesEducation Experience Verification FormROCKNo ratings yet
- Extension in Payment of FeeDocument3 pagesExtension in Payment of FeeAmrit Pal SinghNo ratings yet
- 710 James Robertson Parkway - Andrew Johnson Tower, 12 Floor - Nashville, TN 37243Document2 pages710 James Robertson Parkway - Andrew Johnson Tower, 12 Floor - Nashville, TN 37243nagu323No ratings yet
- Description: Tags: DLB0341AttDocument1 pageDescription: Tags: DLB0341Attanon-404473No ratings yet
- Description: Tags: DLB0341AttDocument1 pageDescription: Tags: DLB0341Attanon-952530No ratings yet
- Instructions:: Part 1-Personal InformationDocument7 pagesInstructions:: Part 1-Personal InformationISLAND NATANYANo ratings yet
- EDSP Application FormDocument4 pagesEDSP Application FormDave MillaresNo ratings yet
- SSS ApplicationDocument4 pagesSSS ApplicationPamela ComerNo ratings yet
- F 3LE Personal History Statement1.2021Document17 pagesF 3LE Personal History Statement1.2021James LewisNo ratings yet
- Vivian Scott Student Application FormDocument3 pagesVivian Scott Student Application Formapi-337237932No ratings yet
- Application For Admission FormDocument2 pagesApplication For Admission Formzacksr34No ratings yet
- 20200228-2020 GESP Application Form PDFDocument2 pages20200228-2020 GESP Application Form PDFMaria MacelNo ratings yet
- Employee Personal Profile 1Document2 pagesEmployee Personal Profile 1zagham.berksNo ratings yet
- Permit To StudyDocument2 pagesPermit To StudyJaidee Ann PerezNo ratings yet
- Limited Special Admission Application 04212013Document3 pagesLimited Special Admission Application 04212013jemccourt7129No ratings yet
- Undocuscholarhip 2014Document5 pagesUndocuscholarhip 2014api-251764893No ratings yet
- Application FormDocument6 pagesApplication FormAkshay SharmaNo ratings yet
- Department of Education: Request Permit To StudyDocument1 pageDepartment of Education: Request Permit To Studydolly kate cagadasNo ratings yet
- Private School M & E Report Form - NEWDocument4 pagesPrivate School M & E Report Form - NEWNer Mangaron100% (1)
- Application Form - Entrance ExamDocument1 pageApplication Form - Entrance Examlovely bless ardonNo ratings yet
- Seattle Schools Service-Learning Form and ReflectionDocument2 pagesSeattle Schools Service-Learning Form and Reflectionsilas StatenNo ratings yet
- EQUIVALENT RECORD FORM ERF Revised 2023Document3 pagesEQUIVALENT RECORD FORM ERF Revised 2023JUNEI LIZA SAMPANINo ratings yet
- StlouisDocument2 pagesStlouisr0kimNo ratings yet
- 3 - SOE Data and VerificationDocument1 page3 - SOE Data and VerificationWhitney DunlapNo ratings yet
- Title I Grant Request For Services v5 12 15 092Document8 pagesTitle I Grant Request For Services v5 12 15 092api-134134588No ratings yet
- Volunteer Form SampleDocument2 pagesVolunteer Form SampleJeffrey BlissiNo ratings yet
- 02 - Youth COMEA Editable EnclosuresDocument7 pages02 - Youth COMEA Editable EnclosuresPrincess Lynn PaduaNo ratings yet
- Last Day Request Form 6.2017Document2 pagesLast Day Request Form 6.2017Raphael AndradeNo ratings yet
- Eskwela Davao Application Form (Blank)Document2 pagesEskwela Davao Application Form (Blank)Aljeania Marie M. MolialNo ratings yet
- Eskwela Davao Application Form (Blank)Document2 pagesEskwela Davao Application Form (Blank)no one33% (3)
- Usc Recommendation FormDocument3 pagesUsc Recommendation FormEARL JOHN A BESARIONo ratings yet
- Tampa Foreign Language Center: 9309 N Florida Ave Suite 109 Tampa, FL 33612 PH (813) 988-7900 FAX (813) 980-3751Document3 pagesTampa Foreign Language Center: 9309 N Florida Ave Suite 109 Tampa, FL 33612 PH (813) 988-7900 FAX (813) 980-3751Jt DouglassNo ratings yet
- Independent Contractor ChecklistDocument2 pagesIndependent Contractor ChecklistwellhellotheresexxayNo ratings yet
- GSIS Educational Subsidy 2021-2022Document2 pagesGSIS Educational Subsidy 2021-2022Noe Carillo CabusaoNo ratings yet
- TA FormDocument2 pagesTA FormEdwin Lopez100% (1)
- South Dakota Board of Regents Undergraduate Student Readmission FormDocument1 pageSouth Dakota Board of Regents Undergraduate Student Readmission FormanttenehNo ratings yet
- Permit To Study NewDocument2 pagesPermit To Study Newailene banuelosNo ratings yet
- Honors Program: Florida State College at JacksonvilleDocument3 pagesHonors Program: Florida State College at JacksonvillemortensenkNo ratings yet
- Staff Recruitment FormDocument3 pagesStaff Recruitment FormArmie FisherNo ratings yet
- KwaZulu Natal Department of Transport Bursary Application FormDocument8 pagesKwaZulu Natal Department of Transport Bursary Application FormMandisa ZibulaNo ratings yet
- Application FormDocument2 pagesApplication Formemmanuel musundireNo ratings yet
- Board Member Application November 2020Document3 pagesBoard Member Application November 2020Graham FilesNo ratings yet
- CCSD Acceleration Request FormDocument1 pageCCSD Acceleration Request Formapi-637800717No ratings yet
- MKU Internal Scholarship Application Form 2023Document9 pagesMKU Internal Scholarship Application Form 2023mugambioscar47No ratings yet
- Memorial Go-Kart Inc.: 5308 Hwy 175 Hartford, WI 53027 262-644-8375Document5 pagesMemorial Go-Kart Inc.: 5308 Hwy 175 Hartford, WI 53027 262-644-8375Hafiezul HassanNo ratings yet
- Consent To TestDocument2 pagesConsent To Testapi-260986714No ratings yet
- Student Academic Appointment Application FormDocument2 pagesStudent Academic Appointment Application FormSais AlasNo ratings yet
- Graduate Information FormDocument1 pageGraduate Information Formapi-290603068No ratings yet
- ME Tools For Mid Year BreakDocument3 pagesME Tools For Mid Year BreakLoidaCarameNo ratings yet
- Permit To StudyDocument2 pagesPermit To StudyJerome SalasNo ratings yet
- Where To Locate The CRN: Class Scheduling FormDocument1 pageWhere To Locate The CRN: Class Scheduling FormBen CamarenoNo ratings yet
- CFWP Waiver BeneficiaryDocument1 pageCFWP Waiver BeneficiaryDominador M. Mejia IIINo ratings yet
- Grade 12Document3 pagesGrade 12browntayan61No ratings yet
- Service Hours Log-Volunteer Approval FormDocument2 pagesService Hours Log-Volunteer Approval FormkylikatzNo ratings yet
- Types of RisksDocument3 pagesTypes of RisksayushdixitNo ratings yet
- How To Run Kalonga MillingDocument11 pagesHow To Run Kalonga MillingDerickMwansa100% (1)
- Summer Training Report On LT Foods Bharat Sachdeva (3) YearDocument81 pagesSummer Training Report On LT Foods Bharat Sachdeva (3) Yearbharat sachdeva50% (2)
- Layoffs, Coping, and Commitment: Impact of Layoffs On Employees and Strategies Used in Coping With LayoffsDocument6 pagesLayoffs, Coping, and Commitment: Impact of Layoffs On Employees and Strategies Used in Coping With LayoffsMohammad MansourNo ratings yet
- BSBDIV501 Aus Accountancy Set For Skilling Program Documents.v1.0Document6 pagesBSBDIV501 Aus Accountancy Set For Skilling Program Documents.v1.0Aakash SharmaNo ratings yet
- Study Guide: Chapter 3: Stakeholders and Corporate Social ResponsibilityDocument2 pagesStudy Guide: Chapter 3: Stakeholders and Corporate Social ResponsibilityChitose HarukiNo ratings yet
- 09 Social Science Key Notes Eco Ch1 People As ResourcesDocument3 pages09 Social Science Key Notes Eco Ch1 People As ResourcesSACHIN TAAK50% (2)
- Mayank Mani - SAP SD - Project Implementation Experience 4.9 Yrs - BangaloreDocument3 pagesMayank Mani - SAP SD - Project Implementation Experience 4.9 Yrs - BangaloreMayank ManiNo ratings yet
- Laredo City Manager ContractDocument7 pagesLaredo City Manager ContractCarlos YNo ratings yet
- 7 DOLE Form - AEDRDocument1 page7 DOLE Form - AEDRJeford Mendaros SalagubangNo ratings yet
- Free Resume Review OnlineDocument6 pagesFree Resume Review Onlineguv0k1jemen3100% (2)
- Paper 2: Business Laws and Business Correspondence and Reporting Section A: Business LawsDocument14 pagesPaper 2: Business Laws and Business Correspondence and Reporting Section A: Business LawsNitesh PatelNo ratings yet
- Opportunities 2020Document7 pagesOpportunities 2020raj xNo ratings yet
- Bananas, Beaches AND Bases: Feminism in IRDocument11 pagesBananas, Beaches AND Bases: Feminism in IRAlyanna CabralNo ratings yet
- Chapter 8 - Understanding Individual BehaviorDocument18 pagesChapter 8 - Understanding Individual BehaviorMy KiềuNo ratings yet
- Purchasing Policy and Procedures-Knowledge How ToDocument39 pagesPurchasing Policy and Procedures-Knowledge How ToPrabhakar Chowdary Chintala100% (1)
- VibinrajDocument5 pagesVibinrajvibinrajNo ratings yet
- W 2Document6 pagesW 2prads1259No ratings yet
- Curriculum Vitae Sample College StudentDocument5 pagesCurriculum Vitae Sample College Studentzxlzszwhf100% (1)
- NRS 440 VN Week 3Document2 pagesNRS 440 VN Week 3Patrick W KagaiNo ratings yet
- MSDs at Port Wine Vines Cultivation - PTDocument8 pagesMSDs at Port Wine Vines Cultivation - PTnmmartinsaNo ratings yet
- Presentation 4Document17 pagesPresentation 4Gochi GamingNo ratings yet
- Ailet: Section Topic No. of QuestionsDocument22 pagesAilet: Section Topic No. of QuestionsabcNo ratings yet
- Economic Terms Glossary PDFDocument12 pagesEconomic Terms Glossary PDFannayaNo ratings yet
- CLFM 2 - Chapter 4 5 - DocxDocument12 pagesCLFM 2 - Chapter 4 5 - DocxKizzy Flores Victorio100% (1)
- Minimum Wages Hosiery Manufactory 2019 - 2020Document1 pageMinimum Wages Hosiery Manufactory 2019 - 2020Adhavan M AnnathuraiNo ratings yet