Download as pdf or txt
You might also like
- Full Ebook of Pizzo Poplack S Pediatric Oncology Eighth Edition Susan M Blaney Lee J Helman Peter C Adamson Online PDF All ChapterDocument69 pagesFull Ebook of Pizzo Poplack S Pediatric Oncology Eighth Edition Susan M Blaney Lee J Helman Peter C Adamson Online PDF All Chapterffancinetefn100% (5)
- Calibration Procedure Crowcon Xgard Gas Detectors - 5720273 - 01Document16 pagesCalibration Procedure Crowcon Xgard Gas Detectors - 5720273 - 01Daniel Rolando Gutierrez FuentesNo ratings yet
- Chemistry Cheat SheetDocument10 pagesChemistry Cheat Sheetbrook93% (40)
- Glenmark Pharmaceuticals Limited: Analytical Research Laboratory (Formulation), TalojaDocument5 pagesGlenmark Pharmaceuticals Limited: Analytical Research Laboratory (Formulation), Talojaरोहित जोशीNo ratings yet
- Ships Electrical Standards CANADA-Sep2007Document133 pagesShips Electrical Standards CANADA-Sep2007Meleti Meleti MeletiouNo ratings yet
- Measuring Body CompositionDocument6 pagesMeasuring Body CompositionKamruzzaman Manik100% (1)
- Body Mass Index ObesityDocument8 pagesBody Mass Index ObesityReyes Falcon D. ÁngelNo ratings yet
- Predictive Validity of Handgrip Strength Vertical Jump Power and Plank Time in The Identification of Pediatric SarcopeniaDocument11 pagesPredictive Validity of Handgrip Strength Vertical Jump Power and Plank Time in The Identification of Pediatric SarcopeniaMessias FilhoNo ratings yet
- Implications of Low Muscle Mass Across The Continuum of Care A Narrative ReviewDocument20 pagesImplications of Low Muscle Mass Across The Continuum of Care A Narrative ReviewAngelica GarciaNo ratings yet
- Calf Circumference Cutoff Values From The NHANES 1999 A 2006Document9 pagesCalf Circumference Cutoff Values From The NHANES 1999 A 2006anthropometricaNo ratings yet
- 2021 - Predictive Validity of Handgrip Strength, Vertical Jump Power, and Plank Time in The Identification of Pediatric SarcopeniaDocument11 pages2021 - Predictive Validity of Handgrip Strength, Vertical Jump Power, and Plank Time in The Identification of Pediatric SarcopeniaAlex LimaNo ratings yet
- Anthropometric Measurement To Identify Undernutrition in Cerabral PalsyDocument8 pagesAnthropometric Measurement To Identify Undernutrition in Cerabral PalsyPam Travezani MiyazakiNo ratings yet
- Artículo 5 - Sumatorio de Pliegues Subcutáneos Valores de Referencia para Atletas de ÉliteDocument8 pagesArtículo 5 - Sumatorio de Pliegues Subcutáneos Valores de Referencia para Atletas de ÉliteEdward LozanoNo ratings yet
- 2013 - Relationship Between BMI and Physical Performance Among Older AdultsDocument4 pages2013 - Relationship Between BMI and Physical Performance Among Older AdultsAlex LimaNo ratings yet
- De Fining Cutoffs To Diagnose Obesity Using The Relative Fat Mass (RFM) : Association With Mortality in NHANES 1999 - 2014Document10 pagesDe Fining Cutoffs To Diagnose Obesity Using The Relative Fat Mass (RFM) : Association With Mortality in NHANES 1999 - 2014Domenico FeleppaNo ratings yet
- 1 s2.0 S2405457723000517 MainDocument10 pages1 s2.0 S2405457723000517 Mainozlemyilmaz1820No ratings yet
- J Parenter Enteral Nutr - 2019 - Sheean - American Society For Parenteral and Enteral Nutrition Clinical Guidelines TheDocument32 pagesJ Parenter Enteral Nutr - 2019 - Sheean - American Society For Parenteral and Enteral Nutrition Clinical Guidelines ThePabloNo ratings yet
- Ej CN 2014213Document3 pagesEj CN 2014213Gustavo NunesNo ratings yet
- Association of Physical Functional Activity Impairment With Severity of Sarcopenic Obesity - Fndings From National Health and Nutrition Examination SurveyDocument10 pagesAssociation of Physical Functional Activity Impairment With Severity of Sarcopenic Obesity - Fndings From National Health and Nutrition Examination SurveymarianaabevicenteNo ratings yet
- Prevalencia Sarcopenia en ChileDocument6 pagesPrevalencia Sarcopenia en ChileFrancisco Mancilla LobosNo ratings yet
- 2013 - Skeletal Muscle Mass Reference Curves For Children and AdolescentsDocument11 pages2013 - Skeletal Muscle Mass Reference Curves For Children and AdolescentsAlex LimaNo ratings yet
- Artigo GenomicaDocument19 pagesArtigo GenomicaAdriano JúniorNo ratings yet
- Arth2011 580632Document6 pagesArth2011 580632hylee102594No ratings yet
- Healthy Status and Energy Balance in Pediatrics: Acta Bio-Medica: Atenei Parmensis February 2006Document8 pagesHealthy Status and Energy Balance in Pediatrics: Acta Bio-Medica: Atenei Parmensis February 2006zahfira edwardNo ratings yet
- Altura Promedio en México Estudio de CasoDocument8 pagesAltura Promedio en México Estudio de CasoEddy HarosNo ratings yet
- Ageing Research ReviewsDocument57 pagesAgeing Research ReviewsPandemic FishpondNo ratings yet
- 2021 Relation of Body Fat Mass and Fat Free Mass To Total MortalityDocument8 pages2021 Relation of Body Fat Mass and Fat Free Mass To Total MortalityLina M GarciaNo ratings yet
- Life 2022, 12, 994Document11 pagesLife 2022, 12, 994soniacsk.cuhkNo ratings yet
- Eu06 2017 Wuf Hellbardt EnglischDocument6 pagesEu06 2017 Wuf Hellbardt EnglischJulio Adan Campos BadilloNo ratings yet
- Relative Fat Mass (RFM) As A New Estimator of Whole-Body Fat Percentage A Cross-Sectional Study in American Adult IndividualsDocument11 pagesRelative Fat Mass (RFM) As A New Estimator of Whole-Body Fat Percentage A Cross-Sectional Study in American Adult IndividualsLaura Hernandez SanchezNo ratings yet
- Assessing The Relationship BetweenDocument6 pagesAssessing The Relationship BetweenTri Eka JuliantoNo ratings yet
- Life Course Socioeconomic Position and Body Composition in Adulthood: A Systematic Review and Narrative SynthesisDocument16 pagesLife Course Socioeconomic Position and Body Composition in Adulthood: A Systematic Review and Narrative SynthesisAdrián Cuenca MercadoNo ratings yet
- Body Mass Index and Body Composition Measures by Dual X-Ray Absorptiometry in Patients Aged 10 To 21 Years With Spinal Cord InjuryDocument8 pagesBody Mass Index and Body Composition Measures by Dual X-Ray Absorptiometry in Patients Aged 10 To 21 Years With Spinal Cord InjuryJoão Pedro PontesNo ratings yet
- BAI Publicacion Original 2011Document7 pagesBAI Publicacion Original 2011gaby fernandezNo ratings yet
- Lamarca 2014Document8 pagesLamarca 2014Ihdinal MuktiNo ratings yet
- Association of Body Mass Index and Waist-To-Hip Ratio With Brain StructureDocument8 pagesAssociation of Body Mass Index and Waist-To-Hip Ratio With Brain StructureBesta Arum BelaNo ratings yet
- ARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsDocument5 pagesARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsPPDS Rehab Medik UnhasNo ratings yet
- Archives of Gerontology and Geriatrics: L. Tay, B.P. Leung, S. Wee, K.S. Tay, N. Ali, M. Chan, W.S. LimDocument8 pagesArchives of Gerontology and Geriatrics: L. Tay, B.P. Leung, S. Wee, K.S. Tay, N. Ali, M. Chan, W.S. LimLIZBETH FEMMIL SAPUTRINo ratings yet
- Fat and Lean Masses in Youths With Down Syndrome: Gender DifferencesDocument9 pagesFat and Lean Masses in Youths With Down Syndrome: Gender DifferencesyenrilisnaNo ratings yet
- Association Between Body Composition and Bone MineDocument5 pagesAssociation Between Body Composition and Bone MineRoxana FrincuNo ratings yet
- Sedentary Behavior, Physical Inactivity, AbdominalDocument11 pagesSedentary Behavior, Physical Inactivity, AbdominalJose VasquezNo ratings yet
- Age, Sex and Ethnic Differences in The Prevalence of Underweight and Overweight, Defined by Using The CDC and IOTF Cut Points in Asian ChildrenDocument8 pagesAge, Sex and Ethnic Differences in The Prevalence of Underweight and Overweight, Defined by Using The CDC and IOTF Cut Points in Asian Childrenatleticar1No ratings yet
- Derivation of A Size-Independent Variable For Scaling of Cardiac Dimensions in A Normal Paediatric PopulationDocument6 pagesDerivation of A Size-Independent Variable For Scaling of Cardiac Dimensions in A Normal Paediatric Populationjaydoc_paed@yahoo.co.inNo ratings yet
- Artigo - AGG-S-20-01215Document29 pagesArtigo - AGG-S-20-01215vicerapNo ratings yet
- Lifetime Risk Childhood Obesity and CardiovascularDocument8 pagesLifetime Risk Childhood Obesity and CardiovascularLuis David Herrera MolinaresNo ratings yet
- Villarroya Et Al,. 2013Document9 pagesVillarroya Et Al,. 2013lauraf9908No ratings yet
- Perspective: Causes, Characteristics, and Consequences of Metabolically Unhealthy Normal Weight in HumansDocument9 pagesPerspective: Causes, Characteristics, and Consequences of Metabolically Unhealthy Normal Weight in HumansYoki VirgoNo ratings yet
- Santana 2019 - de Santana - Brasil - VAT y MortalidadDocument11 pagesSantana 2019 - de Santana - Brasil - VAT y Mortalidad2192036250No ratings yet
- 2021 Lundbad Referencd Values EuropeanDocument10 pages2021 Lundbad Referencd Values European2192036250No ratings yet
- Weiler Et Al. - 2000 - Percent Body Fat and Bone Mass in Healthy Canadian Females 10 To 19 Years of AgeDocument5 pagesWeiler Et Al. - 2000 - Percent Body Fat and Bone Mass in Healthy Canadian Females 10 To 19 Years of AgeCristian BáscoloNo ratings yet
- 24 1520325260 - 06-03-2018 PDFDocument9 pages24 1520325260 - 06-03-2018 PDFEditor IJRITCCNo ratings yet
- Physical Activity and Sarcopenic Obesity: Definition, Assessment, Prevalence and MechanismDocument19 pagesPhysical Activity and Sarcopenic Obesity: Definition, Assessment, Prevalence and MechanismCaro ArduzoNo ratings yet
- Effect of Exercise Training On Weight Loss Body CoDocument14 pagesEffect of Exercise Training On Weight Loss Body CoFabiano LacerdaNo ratings yet
- Body Weight, Health, and Longevity: Medicine and Public IssuesDocument11 pagesBody Weight, Health, and Longevity: Medicine and Public IssuesDavid WheelerNo ratings yet
- Gao Et Al.Document6 pagesGao Et Al.Dries Van ThielenNo ratings yet
- 2023 - The Association Between Sarcopenia and Functional Disability in Older AdultsDocument8 pages2023 - The Association Between Sarcopenia and Functional Disability in Older AdultsAlex LimaNo ratings yet
- Mid-Upper Arm Circumference As An Indicator of UnderweightDocument7 pagesMid-Upper Arm Circumference As An Indicator of UnderweightgianellaNo ratings yet
- Laurson 2011Document7 pagesLaurson 2011Miguel SilvazNo ratings yet
- Research Proposal ExampleDocument10 pagesResearch Proposal ExampleNurul FarhahNo ratings yet
- Ajmg 185 1023Document10 pagesAjmg 185 1023Luis Briones Lau.LiNo ratings yet
- Mpi Geri PDFDocument6 pagesMpi Geri PDFJaka SusilaNo ratings yet
- Adolescent Obesity, Joint Pain, and Hypermobility: Shortreport Open AccessDocument5 pagesAdolescent Obesity, Joint Pain, and Hypermobility: Shortreport Open AccessMCuk2606No ratings yet
- Deurenberg Formula Imc para %grasaDocument10 pagesDeurenberg Formula Imc para %grasaAna Cecilia VegaNo ratings yet
- Strengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesFrom EverandStrengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesNo ratings yet
- 29 Aharavidhi PDFDocument7 pages29 Aharavidhi PDFAjitānanda DāsaNo ratings yet
- COVID-19 SONTU Portable X Ray MachineDocument6 pagesCOVID-19 SONTU Portable X Ray MachinesaidNo ratings yet
- Asean Foundation Asean Meeting 2020 Asean Socio-Cultural Community Topic: Pandemic ControlDocument2 pagesAsean Foundation Asean Meeting 2020 Asean Socio-Cultural Community Topic: Pandemic ControlDifa FarzaniNo ratings yet
- Tracma: Trovador Ramos Consolidated Martial ArtsDocument12 pagesTracma: Trovador Ramos Consolidated Martial Artschristos koutsotasios100% (1)
- Recipes For ShabbatDocument4 pagesRecipes For ShabbatAsher BronsteinNo ratings yet
- Super CalculationsDocument12 pagesSuper CalculationsCarlos Tijerina0% (1)
- Charleston Distance Run - Charleston, WV 2012 - History UpdateDocument18 pagesCharleston Distance Run - Charleston, WV 2012 - History UpdatecharlestondistanceNo ratings yet
- Nutanix EUC Solutions Sales Enabler For PartnersDocument2 pagesNutanix EUC Solutions Sales Enabler For PartnersKevin Karl Gabutin JornacionNo ratings yet
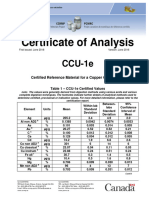
- CCU-1e Certificate enDocument6 pagesCCU-1e Certificate encencisotNo ratings yet
- 10th International Symposium On Avian InfluenzaDocument1 page10th International Symposium On Avian Influenzayos_peace86No ratings yet
- Kew Fdar1Document1 pageKew Fdar1Mariam JubelNo ratings yet
- Pipe Rupture and Fire: Group 07 Case Study ReportDocument7 pagesPipe Rupture and Fire: Group 07 Case Study Reportsukanta60No ratings yet
- Operating Limits of Steels in Hydrogen Service - From API RP 941Document1 pageOperating Limits of Steels in Hydrogen Service - From API RP 941Ajmi HmidaNo ratings yet
- 10SV10NJ4C60Document4 pages10SV10NJ4C60GIAN FRANCO ALBERTO ARENAS VARGASNo ratings yet
- Bellini's Martini MenuDocument2 pagesBellini's Martini Menusupport_local_flavorNo ratings yet
- BlackBook INDEXDocument12 pagesBlackBook INDEXDanishPawaskarNo ratings yet
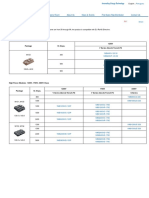
- IGBT Modules 1-Pack Fuji Electric AmericaDocument1 pageIGBT Modules 1-Pack Fuji Electric AmericaSergio MuriloNo ratings yet
- Mozzcato-July To Jun 2017Document28 pagesMozzcato-July To Jun 2017Jing JiaNo ratings yet
- BP US Pipeline Incident InvestigationDocument12 pagesBP US Pipeline Incident InvestigationSoeryanto SlametNo ratings yet
- Valency and Formulae-HandoutDocument3 pagesValency and Formulae-HandoutABHAVYA RAJNo ratings yet
- AnalogyDocument24 pagesAnalogyTrung TranNo ratings yet
- Filling The Gaps: COMMUTE and The Fight For Transit Equity in New York CityDocument20 pagesFilling The Gaps: COMMUTE and The Fight For Transit Equity in New York CityApplied Research CenterNo ratings yet
- CF8M ValvesDocument4 pagesCF8M ValvesPranav PrashantNo ratings yet
- Study Literature Review: Hubungan Tingkat Depresi: Dengan Kualitas Tidur Pada Lanjut UsiaDocument10 pagesStudy Literature Review: Hubungan Tingkat Depresi: Dengan Kualitas Tidur Pada Lanjut UsiaEla NurlaelaNo ratings yet
- Gujarati University, Ahmedabad Question Bank Subject: Alternate Energy Sources, B.E. Sem-Viii, MechanicalDocument2 pagesGujarati University, Ahmedabad Question Bank Subject: Alternate Energy Sources, B.E. Sem-Viii, MechanicalAnkit PatelNo ratings yet