Download as pdf or txt
You might also like
- Strongholds of HeritageDocument9 pagesStrongholds of Heritageusman zafarNo ratings yet
- Official History of 86th DivisionDocument344 pagesOfficial History of 86th DivisionFilipNo ratings yet
- ECG-EKG Presentation - Gunda GDocument21 pagesECG-EKG Presentation - Gunda GGadzikaNo ratings yet
- Electro Cardiogram & DysrythmiasDocument40 pagesElectro Cardiogram & DysrythmiasshobharamkrishnaNo ratings yet
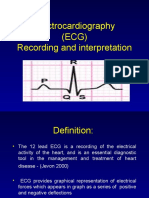
- Electrocardiography (ECG) Recording and InterpretationDocument59 pagesElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- Diagnostic Investigations of Cardiovascular System: A Presentation by Tejaswini MDocument70 pagesDiagnostic Investigations of Cardiovascular System: A Presentation by Tejaswini MDea Amelia YolandaNo ratings yet
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocument50 pagesCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNo ratings yet
- N12 Cardiac DysrhythmiasDocument68 pagesN12 Cardiac Dysrhythmiaskathbondoc03No ratings yet
- Ekg PsikDocument69 pagesEkg PsikZEISVA APRILIANINGRUMNo ratings yet
- Tomasz WikarekDocument95 pagesTomasz Wikareknamar13766No ratings yet
- Kuliah EKG Blok Kegawatdaruratan September 2018Document122 pagesKuliah EKG Blok Kegawatdaruratan September 2018khanzaisdiharanaNo ratings yet
- Electrocardiogram: By: Keverne Jhay P. Colas, RN, MANDocument72 pagesElectrocardiogram: By: Keverne Jhay P. Colas, RN, MANGaras AnnaBerniceNo ratings yet
- Electrocardiogram: Electrocardiogram EKG Heart Heart's Electrical Activity DiagnosisDocument38 pagesElectrocardiogram: Electrocardiogram EKG Heart Heart's Electrical Activity DiagnosislorhenzsoNo ratings yet
- Basic of ECG: Prepared By: Zahid HussainDocument38 pagesBasic of ECG: Prepared By: Zahid HussainZahid Hussain100% (1)
- ECG InterpretationDocument95 pagesECG InterpretationShiela Mae Lopez100% (11)
- ECG ArrythemiaDocument79 pagesECG ArrythemiaMahadevNo ratings yet
- ECGs The Basics (Part 1) LectureDocument32 pagesECGs The Basics (Part 1) Lectureliudmyla zakordonetsNo ratings yet
- ECGs The Basics (Part 1) LectureDocument33 pagesECGs The Basics (Part 1) Lectureliudmyla zakordonetsNo ratings yet
- Ecg Treadmill and Holter TestDocument77 pagesEcg Treadmill and Holter TestRiteka Singh100% (1)
- Atrial FlutterDocument16 pagesAtrial Flutterapi-527603714100% (1)
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
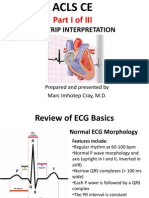
- ACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalDocument80 pagesACLS CE-Part I of III - ECG Strip Interpretation W Case Scenarios SupplementalMarc Imhotep Cray, M.D.100% (2)
- NUR207 Lecture3 CVS 07012021Document197 pagesNUR207 Lecture3 CVS 07012021Ashley TsoiNo ratings yet
- Arrhythmia Clinical PracticeDocument12 pagesArrhythmia Clinical PracticeSaba ElmahadiNo ratings yet
- EKG 12 Leads: Internal Medicine 2010Document59 pagesEKG 12 Leads: Internal Medicine 2010M Lukman HakimNo ratings yet
- Ecg in ExDocument70 pagesEcg in ExLakshmi PrasannaNo ratings yet
- ECG UpdatedDocument115 pagesECG Updatedmominarasool7No ratings yet
- Electrocardiography (Ecg) : Presented By: Fahad I. HussienDocument102 pagesElectrocardiography (Ecg) : Presented By: Fahad I. HussienMustafa A. DawoodNo ratings yet
- Electrical Impulse Viewed: Interpretation of The ElectrocardiogramDocument41 pagesElectrical Impulse Viewed: Interpretation of The ElectrocardiogramNesru Ahmed AkkichuNo ratings yet
- Ecg Interpretation New TemplateDocument88 pagesEcg Interpretation New TemplateJonathan NgNo ratings yet
- Basic Arrythmias: Prof. Maximin A. Pomperada, RN, MNDocument70 pagesBasic Arrythmias: Prof. Maximin A. Pomperada, RN, MNRellie CastroNo ratings yet
- ECG ECG Basics Presentation 201309101527422446 PDFDocument45 pagesECG ECG Basics Presentation 201309101527422446 PDFRamesh RajNo ratings yet
- Aritmia LetalDocument49 pagesAritmia LetalfebriyakNo ratings yet
- EcgDocument248 pagesEcgRohini SelvarajahNo ratings yet
- MUCLecture 2021 1292271Document34 pagesMUCLecture 2021 1292271Kouka MahfoudiNo ratings yet
- ElectrocardiogramDocument29 pagesElectrocardiogrammahnoorNo ratings yet
- Acute Coronary SyndromeDocument79 pagesAcute Coronary SyndromeMuhammad Yufimar Rizza FadilahNo ratings yet
- Workshop Pit IV THN 2017Document57 pagesWorkshop Pit IV THN 2017anettepardedeNo ratings yet
- Lec7 Sem2 CVSWK3 20140920 PDFDocument12 pagesLec7 Sem2 CVSWK3 20140920 PDFAprina RosyadahNo ratings yet
- Basics ECGDocument102 pagesBasics ECGAnnie KhanNo ratings yet
- Module 1.ECG BasicDocument11 pagesModule 1.ECG BasicFerry SofyanriNo ratings yet
- Cardiac Arrhythmia & Basics ECGDocument79 pagesCardiac Arrhythmia & Basics ECGMazhar UllahNo ratings yet
- Cardiovascular DisordersDocument9 pagesCardiovascular Disordersdlneisha6175% (4)
- Basic EKG InterpretationDocument48 pagesBasic EKG InterpretationAimee Ann Pauco MacaraegNo ratings yet
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- Prof. Maila Claire A. Lichauco, RN, MANDocument86 pagesProf. Maila Claire A. Lichauco, RN, MANCedie GomezNo ratings yet
- Normal Sinus RhythmDocument48 pagesNormal Sinus RhythmStella mNo ratings yet
- No VideoDocument47 pagesNo VideoTimothy John BautistaNo ratings yet
- ACLS SubhankarDocument87 pagesACLS SubhankarMarc Andreo MalalaNo ratings yet
- ECG Rhythm InterpretationDocument200 pagesECG Rhythm InterpretationabramNo ratings yet
- ECG3Document58 pagesECG3Plzstudylav SyedNo ratings yet
- 3881 - Prosedur Pendaftaran Internship Per November 2016Document57 pages3881 - Prosedur Pendaftaran Internship Per November 2016Munawir_Syam91No ratings yet
- APEC 611 Scientific and Industrial Instrumentation: Electrocardiogram (ECG)Document22 pagesAPEC 611 Scientific and Industrial Instrumentation: Electrocardiogram (ECG)Faisal Bin KashemNo ratings yet
- Ecg Reading PresntDocument101 pagesEcg Reading PresntbasilielnasirNo ratings yet
- Diagnostic Investigations of Cardiovascular System: A Presentation by Tejaswini MDocument70 pagesDiagnostic Investigations of Cardiovascular System: A Presentation by Tejaswini MKusum RoyNo ratings yet
- ECG MonitoringDocument96 pagesECG MonitoringJey BautistaNo ratings yet
- Ecg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HDocument69 pagesEcg Interpretation: Presented by:-ROHINI RAI M SC Nursing Part I, C.O.N, N.B.M.C.HRohini RaiNo ratings yet
- ECG (Unit3)Document34 pagesECG (Unit3)Komal DagarNo ratings yet
- ECG Complete LectureDocument33 pagesECG Complete LectureDr. SUVA NATHNo ratings yet
- Cardio AssessmentDocument104 pagesCardio Assessmentlowell.cerezo.ihsNo ratings yet
- D_4_heart__2_Document22 pagesD_4_heart__2_Jyoti singhNo ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- MIl-C-70508 Municion Cal. 9 MMDocument17 pagesMIl-C-70508 Municion Cal. 9 MMDavid BasanteNo ratings yet
- Appendix 1: I. Exercise ToleranceDocument5 pagesAppendix 1: I. Exercise Tolerancejfcule1No ratings yet
- Chapter 1 Introduction To International BusinessDocument19 pagesChapter 1 Introduction To International BusinessKushagra RathiNo ratings yet
- 01-System Devices Configuration - Rev GDocument36 pages01-System Devices Configuration - Rev GPABITRA PATRANo ratings yet
- PDF Oxford Textbook of Neuropsychiatry Niruj Agrawal Ebook Full ChapterDocument53 pagesPDF Oxford Textbook of Neuropsychiatry Niruj Agrawal Ebook Full Chapterjames.fahey314100% (1)
- Inventions and InventorsDocument26 pagesInventions and Inventorstaniaul94No ratings yet
- MATLAB-Simulink Based Analysis ofDocument4 pagesMATLAB-Simulink Based Analysis ofAmare KassawNo ratings yet
- Proposal Rev 02Document30 pagesProposal Rev 02suronocaturatmojo100% (1)
- MAC Layer Protocols For Sensor Networks: Leonardo Leiria FernandesDocument29 pagesMAC Layer Protocols For Sensor Networks: Leonardo Leiria FernandesSrinivas GopisettiNo ratings yet
- AnswersDocument8 pagesAnswersDaniyal AsifNo ratings yet
- Insight NDT Equipment LTD - ..Document2 pagesInsight NDT Equipment LTD - ..aoxoxzNo ratings yet
- EP-501, Evolution of Indian Economy Midterm: Submitted By: Prashun Pranav (CISLS)Document8 pagesEP-501, Evolution of Indian Economy Midterm: Submitted By: Prashun Pranav (CISLS)rumiNo ratings yet
- MaglevDocument10 pagesMaglevCaramihai DenisNo ratings yet
- DIYode Issue 1 July 2017Document100 pagesDIYode Issue 1 July 2017Victor Hugo Garay Saez100% (2)
- WSP India Compendium of Good Practices Rural Water Supply SchemesDocument104 pagesWSP India Compendium of Good Practices Rural Water Supply SchemesNguyen Van KienNo ratings yet
- Creative Writing Q1W1Document39 pagesCreative Writing Q1W1Jhun Ar-Ar Roa RamosNo ratings yet
- Uh - B-Eye-D Uh - Bil-Ih-Tee: Senior NESC-GE 2018 Regional Round Word List Grades 9, 10, 11, 12Document12 pagesUh - B-Eye-D Uh - Bil-Ih-Tee: Senior NESC-GE 2018 Regional Round Word List Grades 9, 10, 11, 12Tiko MakharadzeNo ratings yet
- Fire Phenomena of Rigid Polyurethane FoamsDocument22 pagesFire Phenomena of Rigid Polyurethane FoamsNicola MelaNo ratings yet
- Behavioral Neuroscience of Motivation: Eleanor H. Simpson Peter D. Balsam EditorsDocument584 pagesBehavioral Neuroscience of Motivation: Eleanor H. Simpson Peter D. Balsam EditorsKyle penzes100% (1)
- Resistors Module 01Document10 pagesResistors Module 01VinodKumarTummalurNo ratings yet
- Isotonix OPC-3 Sep 2016Document4 pagesIsotonix OPC-3 Sep 2016Pching Yong100% (1)
- Evaluation of SHMP and Advanced Scale Inhibitors For Control of and Scales in RO DesalinationDocument10 pagesEvaluation of SHMP and Advanced Scale Inhibitors For Control of and Scales in RO DesalinationKool LokeshNo ratings yet
- 1MRK002136-D: Package of Contact Sockets 20A, 100 PCSDocument1 page1MRK002136-D: Package of Contact Sockets 20A, 100 PCSWilfridoMatusSanchesNo ratings yet
- Mini Project Report On: Visvesvaraya Technological UniversityDocument8 pagesMini Project Report On: Visvesvaraya Technological UniversityTejáś ĢøwđâNo ratings yet
- Ricketts - Insurance Is PlaintiffDocument24 pagesRicketts - Insurance Is PlaintiffAnn DwyerNo ratings yet
- Leak Detector and Auto Cut OffDocument8 pagesLeak Detector and Auto Cut OffARUN CHRISTEL ANo ratings yet
- Ratio, Variation and Proportion: MATH10 AlgebraDocument19 pagesRatio, Variation and Proportion: MATH10 AlgebraEd VillNo ratings yet