Download as pdf or txt
You might also like
- Safe Work Permit FormDocument1 pageSafe Work Permit FormAbdulah Asagi33% (3)
- Automatic Sprinkler Systems Acceptance Test Checklist NFPA 13Document3 pagesAutomatic Sprinkler Systems Acceptance Test Checklist NFPA 13duchoang5000100% (1)
- Genset Startup and Commissioning Checklist C 175Document3 pagesGenset Startup and Commissioning Checklist C 175Dwi Mulyanti Dwimulyantishop100% (1)
- Fire Alarm Isolation Permit - Form ADocument1 pageFire Alarm Isolation Permit - Form AMuhammad Azam0% (1)
- Electrical Work Permit: Smg1 Flowline ProjectDocument2 pagesElectrical Work Permit: Smg1 Flowline Projectghazi kallel33% (3)
- Automatic Sprinkler Systems Acceptance Test Checklist NFPA 13 PDFDocument3 pagesAutomatic Sprinkler Systems Acceptance Test Checklist NFPA 13 PDFanon_299280009No ratings yet
- Industrial Applications of Infrared Thermography: How Infrared Analysis Can be Used to Improve Equipment InspectionFrom EverandIndustrial Applications of Infrared Thermography: How Infrared Analysis Can be Used to Improve Equipment InspectionRating: 4.5 out of 5 stars4.5/5 (3)
- Ansi Bhma A156.40 2015 PDFDocument34 pagesAnsi Bhma A156.40 2015 PDFShawn DeolNo ratings yet
- Hot PermitDocument2 pagesHot Permitmohamed esmailNo ratings yet
- Contractor Permit To WorkDocument1 pageContractor Permit To WorkChetan patilNo ratings yet
- General Work Permit S3-F7: Start Date: End Date: Start Time: End TimeDocument1 pageGeneral Work Permit S3-F7: Start Date: End Date: Start Time: End TimeHareekirishnan LrkNo ratings yet
- Emergency, Drill Reporting FormDocument2 pagesEmergency, Drill Reporting FormJakeer hussain ShaikNo ratings yet
- Fire Safety Plan FormatDocument14 pagesFire Safety Plan FormatAlam TarequeNo ratings yet
- Contractor'S Material and Test Certificate Fire Alarm and Fire Detection SystemsDocument3 pagesContractor'S Material and Test Certificate Fire Alarm and Fire Detection SystemsMuhammadsarwar AbubakarNo ratings yet
- Cold Work Permit: Smg1 Flowline ProjectDocument2 pagesCold Work Permit: Smg1 Flowline Projectghazi kallelNo ratings yet
- S 9.32C - High Voltage PermitDocument2 pagesS 9.32C - High Voltage PermitWILLIAMNo ratings yet
- Hot Work PermitDocument1 pageHot Work PermitVijayakumar KarunanidhiNo ratings yet
- Fire Safety & Evacuation PlanDocument20 pagesFire Safety & Evacuation PlanazozinlcNo ratings yet
- UNC Fire Protection System Impairment Procedures 6 17Document7 pagesUNC Fire Protection System Impairment Procedures 6 17Sigit MahardikaNo ratings yet
- UNC Fire Protection System Impairment Procedures 6 17 PDFDocument7 pagesUNC Fire Protection System Impairment Procedures 6 17 PDFmonica dwimandhaNo ratings yet
- Permis de TravailDocument48 pagesPermis de TravailMohamed Wolf75% (8)
- Laporan KomisioningDocument3 pagesLaporan KomisioningEko PratamaNo ratings yet
- Cold Work PermitDocument3 pagesCold Work Permitnakul kushwahaNo ratings yet
- Confined Space Entry Permit Rev 01Document3 pagesConfined Space Entry Permit Rev 01Neel Vadera100% (1)
- Coldworkpermitformhseq Cwprev2 230424064127 3aee7c75Document2 pagesColdworkpermitformhseq Cwprev2 230424064127 3aee7c75egorgrigorjev5No ratings yet
- Child Care Facility Maintenance ChecklistDocument6 pagesChild Care Facility Maintenance ChecklisttmamputsiNo ratings yet
- System Test Report - Fire PumpDocument4 pagesSystem Test Report - Fire Pumpsyamsul bahriNo ratings yet
- Work PermitDocument3 pagesWork PermitMadhu Babu KancharlaNo ratings yet
- CamScanner 03-22-2023 07.44Document2 pagesCamScanner 03-22-2023 07.44Umar AliNo ratings yet
- Line Break, Equip Opening PermitDocument6 pagesLine Break, Equip Opening PermitSyed Mustafa HussainNo ratings yet
- Report Form of Detailed Inspection For Fire ProDocument35 pagesReport Form of Detailed Inspection For Fire Proraul m tuscanoNo ratings yet
- General PermitDocument1 pageGeneral PermitArmando AballeNo ratings yet
- Inquiry Data / Equipment InformationDocument2 pagesInquiry Data / Equipment InformationAmmar BaigNo ratings yet
- Machinery Breakdown Claim FormDocument1 pageMachinery Breakdown Claim FormSeema BhattNo ratings yet
- Renewable Systems RebateDocument4 pagesRenewable Systems RebatesandyolkowskiNo ratings yet
- 02 - Electrical Work PermitDocument1 page02 - Electrical Work Permitwinston11No ratings yet
- Annual Fire Alarm Service ReportDocument10 pagesAnnual Fire Alarm Service ReportrisnaidiNo ratings yet
- Compair Dryer - Commissioning ReportDocument3 pagesCompair Dryer - Commissioning Reportandy habibiNo ratings yet
- PTW General Work - 2020, FilledDocument4 pagesPTW General Work - 2020, FilledPalaniappan SolaiyanNo ratings yet
- General Work PermitDocument2 pagesGeneral Work PermitJareem PeesNo ratings yet
- Line Break, Equip Opening PermitDocument1 pageLine Break, Equip Opening PermitSyed Mustafa HussainNo ratings yet
- AXA Affin Impairment FormDocument2 pagesAXA Affin Impairment FormZubaidi OthmanNo ratings yet
- Breaker Driving Machine InspectionDocument2 pagesBreaker Driving Machine InspectionMochammad AriefNo ratings yet
- Null 5Document2 pagesNull 5Ashish SinghNo ratings yet
- General Work PermitDocument2 pagesGeneral Work PermitAde Mazmur SilabanNo ratings yet
- Work PermitDocument2 pagesWork PermitC P TiwariNo ratings yet
- WP-HSE-010 (Bored Pile)Document1 pageWP-HSE-010 (Bored Pile)Armando AballeNo ratings yet
- Fire Impairment Permit Unit: Department:: Page: X of Y W.P.No. FI........Document2 pagesFire Impairment Permit Unit: Department:: Page: X of Y W.P.No. FI........Chaitanya MyneniNo ratings yet
- Hot Work PermitDocument2 pagesHot Work PermitRex UrbiztondoNo ratings yet
- LAWA Basic Commissioning Forms - CompleteDocument53 pagesLAWA Basic Commissioning Forms - Completemohammed_hatem0% (1)
- Revised - FIRE RISK INSPECTION FORMAT 26Document2 pagesRevised - FIRE RISK INSPECTION FORMAT 26Rupesh SinghNo ratings yet
- Fire Protection System Impairment Procedure: October 2020Document7 pagesFire Protection System Impairment Procedure: October 2020abi_ezerNo ratings yet
- Fire Alarm InspectionDocument3 pagesFire Alarm InspectionAbu TalebNo ratings yet
- Spill FormDocument5 pagesSpill FormFrank OhiriNo ratings yet
- 300.91F - Fire Alarm - Report of InspectionDocument7 pages300.91F - Fire Alarm - Report of InspectionRiski SuhardinataNo ratings yet
- Fire Incident Report: Complete and and Fax One Copy To The Appropriate Agency Field Office (See Fax Numbers At: HTTPDocument2 pagesFire Incident Report: Complete and and Fax One Copy To The Appropriate Agency Field Office (See Fax Numbers At: HTTPbenonNo ratings yet
- Work Approval (PTW) : Initiator'S ChecklistDocument2 pagesWork Approval (PTW) : Initiator'S ChecklistC&I REGLNo ratings yet
- Hot Work Permit (Supplementary Permit)Document1 pageHot Work Permit (Supplementary Permit)skskNo ratings yet
- Ochid Hot-Work-PermitDocument3 pagesOchid Hot-Work-PermitRehan AbbasiNo ratings yet
- Procédure Des Permis de TravailDocument48 pagesProcédure Des Permis de TravailMed Hillel Elarouci67% (3)
- Itr-Msa (Air Cooler)Document13 pagesItr-Msa (Air Cooler)mahmoudNo ratings yet
- Machine (Mechanical) - Wikipedia, The Free EncyclopediaDocument10 pagesMachine (Mechanical) - Wikipedia, The Free EncyclopediabmxengineeringNo ratings yet
- Chapter 6 Financial AssetsDocument6 pagesChapter 6 Financial AssetsJoyce Mae D. FloresNo ratings yet
- 14.3 Study GuideDocument3 pages14.3 Study Guide4b00d1No ratings yet
- AfunimawobeDocument14 pagesAfunimawobeAbdulsala100% (3)
- Individual Report 23001Document5 pagesIndividual Report 23001Ashley MartinezNo ratings yet
- Looking Back and Looking ForwardDocument6 pagesLooking Back and Looking ForwardJotham SederstromNo ratings yet
- Polarized Light MicrosDocument59 pagesPolarized Light MicrosAnonymous Ukn4LwNo ratings yet
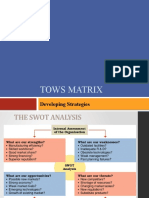
- Tows Matrix: Developing StrategiesDocument29 pagesTows Matrix: Developing StrategiesalkalkiaNo ratings yet
- Anatomy of Frontal Sinus & RecessDocument50 pagesAnatomy of Frontal Sinus & Recessanoop_aiims1No ratings yet
- 2008 Bullentin Rel. 2-DataDocument5 pages2008 Bullentin Rel. 2-DataKalai SelvanNo ratings yet
- A List of Run Commands For Windows 7: Windows Logo Key + RDocument2 pagesA List of Run Commands For Windows 7: Windows Logo Key + RDinesh KumarNo ratings yet
- 2.3 Routine, Good News and Good Will MessagesDocument20 pages2.3 Routine, Good News and Good Will MessagesSyed Zubair AliNo ratings yet
- Software Manual DPL Magic MarkerDocument148 pagesSoftware Manual DPL Magic Markerjsiai100% (1)
- CAMBODIAN Temple Designs-And Hindu Cosmology-: DR Uday DokrasDocument15 pagesCAMBODIAN Temple Designs-And Hindu Cosmology-: DR Uday DokrasUday DokrasNo ratings yet
- Missionary Recommendation Physician Dental FormDocument5 pagesMissionary Recommendation Physician Dental FormdozieojiakuNo ratings yet
- B.Sc. SEM IDocument4 pagesB.Sc. SEM IsameerNo ratings yet
- Incident Investigation Report - Fire Incedent - 04-11-2018 Swati InteriorsDocument4 pagesIncident Investigation Report - Fire Incedent - 04-11-2018 Swati InteriorsMobin Thomas AbrahamNo ratings yet
- Prospective vs. Retrospective Delay Analysis: Rohit Singhal, Shishir Kant & Adarsh KumarDocument10 pagesProspective vs. Retrospective Delay Analysis: Rohit Singhal, Shishir Kant & Adarsh KumarKevin DonNo ratings yet
- JAMB English Language Past Questions and Answers 2010 - 2018Document84 pagesJAMB English Language Past Questions and Answers 2010 - 2018Joel Adams100% (6)
- Ddpa 3092 Reaction of A Continuous BeamDocument4 pagesDdpa 3092 Reaction of A Continuous Beamnurlisa khaleedaNo ratings yet
- Bar Charts in ResearchDocument5 pagesBar Charts in ResearchPraise NehumambiNo ratings yet
- A Sophisticated and Automated Form of TLCDocument25 pagesA Sophisticated and Automated Form of TLCIshfaq AhmadNo ratings yet
- UFOs Caught in A Web of DeceptionDocument30 pagesUFOs Caught in A Web of DeceptionMarko CankarNo ratings yet
- Caspah - Kamunda 1593513704 ADocument42 pagesCaspah - Kamunda 1593513704 Ajoseph wamulumeNo ratings yet
- Scania Diagnos & Programmer 3 2xxxDocument7 pagesScania Diagnos & Programmer 3 2xxxFran Alisson SouzaNo ratings yet
- DM Unit-IvDocument134 pagesDM Unit-IvDwaarakesh RameshNo ratings yet
- Research Methodology - 9Document12 pagesResearch Methodology - 9OmeYadavNo ratings yet
- UT4000A Patient MonitorDocument5 pagesUT4000A Patient MonitorJuan Pablo MatadamazNo ratings yet
- Lesson 9 Final PDFDocument120 pagesLesson 9 Final PDFFire RobloxNo ratings yet