Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Dolcet Drug StudyDocument1 pageDolcet Drug StudyACOB, Jamil C.No ratings yet
- Bola CommunityDocument5 pagesBola CommunityOladimeji Raphael OnibonNo ratings yet
- Greyhounds Pain ManagementDocument5 pagesGreyhounds Pain ManagementPeterNo ratings yet
- Pricelist Pharmasolindo 2018Document11 pagesPricelist Pharmasolindo 2018Niken Claudya Ecfrencylie0% (1)
- DR Preeti - Analgesics PDFDocument32 pagesDR Preeti - Analgesics PDFNajla MohammedNo ratings yet
- SUD I - Opioid-Related Disorders Cheat Sheet: by ViaDocument4 pagesSUD I - Opioid-Related Disorders Cheat Sheet: by ViaDonatella S.No ratings yet
- Pharmacology of Antipyretic DrugsDocument19 pagesPharmacology of Antipyretic DrugsPretty HiaNo ratings yet
- Antiinflamatoare NesteroidieneDocument2 pagesAntiinflamatoare NesteroidieneLore DanaNo ratings yet
- Astadol Brand PlanDocument19 pagesAstadol Brand PlanNauman AkramNo ratings yet
- Pain Card v31Document2 pagesPain Card v31srajnicNo ratings yet
- Pca Epic Order SetsDocument4 pagesPca Epic Order Setsapi-244230664No ratings yet
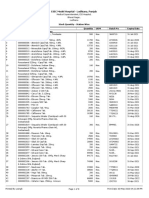
- ESIC Model Hospital - Ludhiana, PunjabDocument8 pagesESIC Model Hospital - Ludhiana, PunjabPushpinder Singh SandhuNo ratings yet
- Az Essential RX ListDocument141 pagesAz Essential RX ListAbdullah HamdanNo ratings yet
- Pharmacology - 1 Analgesics: Maram A.T. M. KhaledDocument15 pagesPharmacology - 1 Analgesics: Maram A.T. M. Khaledمحمد الاسوانيNo ratings yet
- Farmacologie PediatricaDocument4 pagesFarmacologie Pediatricarodyca5sep100% (1)
- Formularium KF 58 - EviDocument8 pagesFormularium KF 58 - EviNurul Evi kurniatiNo ratings yet
- Post-Operative Pain Management.: Murtaza Asif Ali Queen's Hospital Burton Upon TrentDocument33 pagesPost-Operative Pain Management.: Murtaza Asif Ali Queen's Hospital Burton Upon TrentM Asif AliNo ratings yet
- 2021 Synthetic Opioids Fact SheetDocument5 pages2021 Synthetic Opioids Fact SheetShannanNo ratings yet
- Max 360mg/d Codein Max 12 Tabs/d Max 4g/d Max 1.2 G 2.4g/d Max 120mg/dDocument3 pagesMax 360mg/d Codein Max 12 Tabs/d Max 4g/d Max 1.2 G 2.4g/d Max 120mg/dSamantha LuiNo ratings yet
- Tugas Obat KerasDocument34 pagesTugas Obat KerasaminnatuljannahNo ratings yet
- Nimesulide BrandsDocument1 pageNimesulide BrandsKimberly RiceNo ratings yet
- ترجمه PDFDocument4 pagesترجمه PDFAshkan Abbasi0% (1)
- Anti-Inflammatory, Anti-Arthritis, and Related AgentsDocument22 pagesAnti-Inflammatory, Anti-Arthritis, and Related AgentsMarjolene PudaderaNo ratings yet
- Arcoxia - ProspectDocument4 pagesArcoxia - ProspectIoana CorinaNo ratings yet
- K10 Opioid AnalgesicsDocument30 pagesK10 Opioid AnalgesicsLa Lydia TampubolonNo ratings yet
- ANTINYERIDocument12 pagesANTINYERINunuk HidayantiNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument45 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsNoor RamadhaniahNo ratings yet
- Ketamine For Opiate WithdrawalDocument3 pagesKetamine For Opiate WithdrawalroboNo ratings yet
- Nervous System and Neurology Assignment - AcrobatiqDocument1 pageNervous System and Neurology Assignment - Acrobatiqjose. medina9No ratings yet
- Siti Muniroh Nurul Aini (1802050215) Tugas Farmasi KomunitasDocument8 pagesSiti Muniroh Nurul Aini (1802050215) Tugas Farmasi KomunitasArroh NurulaynyNo ratings yet