Download as pdf or txt
You might also like
- Aqa A Level Biology p1 QPDocument36 pagesAqa A Level Biology p1 QPJaden MistryNo ratings yet
- Histology Krok 1Document103 pagesHistology Krok 1Ridhan SinghNo ratings yet
- Rapid Diagnostic Tests For Covid-19Document4 pagesRapid Diagnostic Tests For Covid-19Febri RirinNo ratings yet
- ImmunoSeroLab M4Document3 pagesImmunoSeroLab M4ela kikayNo ratings yet
- Additional Notes Nature of Clinical LaboratoryDocument4 pagesAdditional Notes Nature of Clinical LaboratorySheriffCaitlynNo ratings yet
- Pmls MidtermsDocument11 pagesPmls MidtermsErnest VincentNo ratings yet
- 7.0 Antiboby Detection 1Document5 pages7.0 Antiboby Detection 1Sherwin BumanglagNo ratings yet
- 2-Syphilis Congenital PKEL FinalDocument24 pages2-Syphilis Congenital PKEL FinalGilang KusdinarNo ratings yet
- Antibody Screening and Identification ObjectivesDocument3 pagesAntibody Screening and Identification ObjectivesApril SudarioNo ratings yet
- Module 1 Introduction To rHIVdaDocument49 pagesModule 1 Introduction To rHIVdaRaki Dallas100% (1)
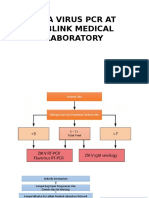
- Zika Virus PCR at Lablink Medical LaboratoryDocument13 pagesZika Virus PCR at Lablink Medical LaboratoryAmrit SoniaNo ratings yet
- Laboratory Testing For COVID-19 - Dr. Trilis Yulianti, M.kesDocument20 pagesLaboratory Testing For COVID-19 - Dr. Trilis Yulianti, M.kesYayax RakhmanNo ratings yet
- Lab Topic 14 QA & QC in The Molecular LaboratoryDocument6 pagesLab Topic 14 QA & QC in The Molecular LaboratoryNatasha MendozaNo ratings yet
- Concept MapDocument10 pagesConcept MapStephen YorNo ratings yet
- Elecsys® Anti-HAV IgM Immunoassay For The Qualitative Detection of IgM Antibodies Against HAVDocument4 pagesElecsys® Anti-HAV IgM Immunoassay For The Qualitative Detection of IgM Antibodies Against HAVLAMA LAMANo ratings yet
- The Use of The Cobas Liat System ForDocument15 pagesThe Use of The Cobas Liat System ForAmirah AliNo ratings yet
- Syphilis Screening Testing and TreatmentDocument2 pagesSyphilis Screening Testing and TreatmentMoeed Iqbal100% (1)
- COVID19 Module 1 Section C Diagnostics Ramos-NinoDocument32 pagesCOVID19 Module 1 Section C Diagnostics Ramos-NinoReggieNo ratings yet
- Bosch Vivalytic Sti Cartiladge and QC IFU Update 17-3 Last UpdateDocument7 pagesBosch Vivalytic Sti Cartiladge and QC IFU Update 17-3 Last UpdateMohammed AlshnqityNo ratings yet
- Ag Ab DetectionDocument43 pagesAg Ab DetectionMaaz AlwaliNo ratings yet
- Frilasita Aisyah Yudhaputri, MbiomedscDocument21 pagesFrilasita Aisyah Yudhaputri, MbiomedscDwoyo GiyatmokoNo ratings yet
- Serocheck TP DevicekkkkDocument4 pagesSerocheck TP DevicekkkkMatibar RahmanNo ratings yet
- BB - Detection and Identification of AntibodiesDocument10 pagesBB - Detection and Identification of AntibodiesWayne VillalunaNo ratings yet
- NacoDocument7 pagesNacoqk5jh5bwgmNo ratings yet
- BB - BLOOD COMPONENT PREPARATION (Part 2)Document10 pagesBB - BLOOD COMPONENT PREPARATION (Part 2)Wayne VillalunaNo ratings yet
- LabreportDocument3 pagesLabreportr.sakthivelmuruganNo ratings yet
- Chapter 41 - LEH Function TestDocument6 pagesChapter 41 - LEH Function TestCha GuingabNo ratings yet
- Enterochek WBDocument4 pagesEnterochek WBTehMarianNo ratings yet
- Is FinalsDocument78 pagesIs FinalsMarissa CordovaNo ratings yet
- ELISA Test - Principle, Materials, Procedure Results - Microbe OnlineDocument5 pagesELISA Test - Principle, Materials, Procedure Results - Microbe OnlineAll in oneNo ratings yet
- Human Immunodeficiency Virus: Laboratory Diagnosis of (HIV)Document42 pagesHuman Immunodeficiency Virus: Laboratory Diagnosis of (HIV)Dr.Mustafa Al-massadNo ratings yet
- Herpetic Mucocutaneous Infections: HSV (HSV 1 & 2) & VZVDocument32 pagesHerpetic Mucocutaneous Infections: HSV (HSV 1 & 2) & VZVJaneNo ratings yet
- Instrumentation and Quality Control in HemostasisDocument5 pagesInstrumentation and Quality Control in HemostasisGerly MaglangitNo ratings yet
- Specimen Collection (HEMA)Document11 pagesSpecimen Collection (HEMA)April Lady Faith P. PaundogNo ratings yet
- Antibody PanelDocument5 pagesAntibody PanelCarl Dominic GasconNo ratings yet
- Ensuring QPCR Data Reliability - Controlling For ContaminationDocument10 pagesEnsuring QPCR Data Reliability - Controlling For ContaminationSyarifHidayatNo ratings yet
- Fana TrainingDocument174 pagesFana TrainingHaidee SaavedraNo ratings yet
- Recent Trends in The Serologic Diagnosis of Syphilis: Muhammad G. Morshed, Ameeta E. SinghDocument21 pagesRecent Trends in The Serologic Diagnosis of Syphilis: Muhammad G. Morshed, Ameeta E. SinghNana ArthetaNo ratings yet
- (MT 6322 - MYCO VIRO LAB) Unit 8 Lab Diagnosis For Arboviruses, Roboviruses, dsRNADocument3 pages(MT 6322 - MYCO VIRO LAB) Unit 8 Lab Diagnosis For Arboviruses, Roboviruses, dsRNAAbbas MaghazehiNo ratings yet
- Selection of Incubation Phase: TABLE 6-2Document10 pagesSelection of Incubation Phase: TABLE 6-2Karen Flores BartoloNo ratings yet
- Serological Test PrinciplesDocument15 pagesSerological Test PrinciplesDiana Kate GalleroNo ratings yet
- Neu - Präsentation Englisch - Ohne ZertifikatDocument18 pagesNeu - Präsentation Englisch - Ohne ZertifikatWagner SanchezNo ratings yet
- 1.IMEI SyphilisDocument3 pages1.IMEI Syphilistran leNo ratings yet
- Blood Test - LFTDocument4 pagesBlood Test - LFTAbhi NikamNo ratings yet
- Serological TestsDocument2 pagesSerological TestsKimberly EspaldonNo ratings yet
- Chem LecDocument11 pagesChem LecBeautyand ThebeastNo ratings yet
- Immunohematology Handouts UpdatedDocument15 pagesImmunohematology Handouts UpdateddmclmllNo ratings yet
- 2023 NRL EQAS CatalogueDocument24 pages2023 NRL EQAS CatalogueQFCarlosCQNo ratings yet
- Mtap - Immunohema Transfusion MedicineDocument9 pagesMtap - Immunohema Transfusion MedicineMoira Pauline LibroraniaNo ratings yet
- HIV1-2 AgAb Combo PI2Document10 pagesHIV1-2 AgAb Combo PI2JamilNo ratings yet
- Wang TB Case PresentationDocument11 pagesWang TB Case Presentationtahiranawab246No ratings yet
- HCV (Cassette)Document1 pageHCV (Cassette)عائش العموديNo ratings yet
- Coronavirus CaseteDocument1 pageCoronavirus CaseteLidia NarbNo ratings yet
- Combo Dengue KitDocument24 pagesCombo Dengue KitQlife KlinikNo ratings yet
- Post Analytical Phase of Laboratory TestingDocument7 pagesPost Analytical Phase of Laboratory TestingClarisse De Guzman100% (1)
- SysmexDocument51 pagesSysmexGregorio De Las CasasNo ratings yet
- Specimen ConsiderationsDocument17 pagesSpecimen ConsiderationsRace MendezNo ratings yet
- Publicationsohpsyphilis Testing and Lab InterpretationDocument4 pagesPublicationsohpsyphilis Testing and Lab InterpretationQusai & MOHAMMEDNo ratings yet
- Tes Lab Penyakit Infeksi Dan Tropis (April 2011)Document143 pagesTes Lab Penyakit Infeksi Dan Tropis (April 2011)Fajrul AnsarNo ratings yet
- Sops HivDocument48 pagesSops Hivahmed alghrablyNo ratings yet
- Understanding Laboratory Investigations: A Guide for Nurses, Midwives and Health ProfessionalsFrom EverandUnderstanding Laboratory Investigations: A Guide for Nurses, Midwives and Health ProfessionalsNo ratings yet
- Potential Use of Probiotics: Ekachai ChukeatiroteDocument8 pagesPotential Use of Probiotics: Ekachai ChukeatiroteDanu EffendiNo ratings yet
- OKK EDIT Marty Jopson - The Science of Being Human - Why We Behave, Think and Feel The Way We Do-Michael O'Mara (2019) - PagenumberDocument157 pagesOKK EDIT Marty Jopson - The Science of Being Human - Why We Behave, Think and Feel The Way We Do-Michael O'Mara (2019) - Pagenumberhome improvement books100% (1)
- IGCSE Biology P43 May2020 QPDocument17 pagesIGCSE Biology P43 May2020 QPPakorn WinayanuwattikunNo ratings yet
- Ref Paczosa TatedaDocument33 pagesRef Paczosa TatedaJuan Martín VargasNo ratings yet
- Guide Biomedical Treatment 101Document12 pagesGuide Biomedical Treatment 101wrestlerloverNo ratings yet
- Addressing Patient Specificity in The Engineering of Tumor ModelsDocument36 pagesAddressing Patient Specificity in The Engineering of Tumor ModelsNadia Al RefaieNo ratings yet
- Mechanism of TranspositionDocument16 pagesMechanism of TranspositionBandook Gamers100% (3)
- Staphylococcus EpidermidisDocument4 pagesStaphylococcus Epidermidisemanuel santiago triana rujanaNo ratings yet
- 8 - Rheumatology Passmedicine Q. Bank PART I 2017 PDFDocument283 pages8 - Rheumatology Passmedicine Q. Bank PART I 2017 PDFSiva Raman100% (1)
- Diagnostic Considerations in Uveitis: AAO Reading Section 9Document43 pagesDiagnostic Considerations in Uveitis: AAO Reading Section 9evaNo ratings yet
- Biology (044) - Practical Lab Manual (Term - 1)Document24 pagesBiology (044) - Practical Lab Manual (Term - 1)Tejeswar MajhiNo ratings yet
- Microbiology and Parasitology-ScDocument23 pagesMicrobiology and Parasitology-ScSelena MoonNo ratings yet
- Medical Terminology and PhrasesDocument60 pagesMedical Terminology and Phrasesapi-3743320No ratings yet
- 2-Autoimmune DiseasesDocument29 pages2-Autoimmune DiseasessoniaNo ratings yet
- Topic 1.1 Test (Science 10) : Relevance Extending Proficient Developing EmergingDocument2 pagesTopic 1.1 Test (Science 10) : Relevance Extending Proficient Developing EmergingJeffrey PiggottNo ratings yet
- FatimaDocument2 pagesFatimamstoomeNo ratings yet
- Effect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialDocument8 pagesEffect of Clarithromycin in Patients With Suspected Gram-Negative Sepsis: Results of A Randomized Controlled TrialH Yudi IriantoNo ratings yet
- D0685 Biology Paper2Document9 pagesD0685 Biology Paper2Aryan SinghNo ratings yet
- AnaplasmosisDocument1 pageAnaplasmosisDumapis RichardNo ratings yet
- Pancreas: Cole Barthel Adrienne Blount Jason Liu Becca WiluszDocument42 pagesPancreas: Cole Barthel Adrienne Blount Jason Liu Becca WiluszPriyanka TrivediNo ratings yet
- Cmb-Ppt-5-Endoplasmic Reticulum-Borja, Jayven CDocument11 pagesCmb-Ppt-5-Endoplasmic Reticulum-Borja, Jayven CJboar TbenecdiNo ratings yet
- Chromosomal AberrationDocument7 pagesChromosomal AberrationANSA PRIYADARSHINI0% (1)
- Aipmt 2009 Full PaperDocument38 pagesAipmt 2009 Full PaperIshanshu Bajpai100% (1)
- Mpmi 05 23 0073 HHDocument8 pagesMpmi 05 23 0073 HHRoden Carlo LizardoNo ratings yet
- Long Case JaundiceDocument5 pagesLong Case JaundiceNadia SalwaniNo ratings yet
- General Biology 1 Gas GeneticsDocument39 pagesGeneral Biology 1 Gas GeneticsDary SobrecareyNo ratings yet
- Adipose Tissue Expandability, Lipotoxicity and The Metabolic SyndromeDocument12 pagesAdipose Tissue Expandability, Lipotoxicity and The Metabolic SyndromePsicología del SerNo ratings yet
- GeneticDocument117 pagesGeneticFiza RizviNo ratings yet