
Dexamethasone Suppression Tests
Dexamethasone Suppression Tests
You might also like
- CASINO by Nicholas PileggiDocument238 pagesCASINO by Nicholas PileggiPutipufNo ratings yet
- Tanner Whitehouse TestDocument25 pagesTanner Whitehouse TestCota Ancuta0% (1)
- 4Z4TJDocument16 pages4Z4TJBimal Chutia100% (1)
- ENDOCRINOLOGY Handbook of Obesity 2003 PDFDocument1,056 pagesENDOCRINOLOGY Handbook of Obesity 2003 PDFCota AncutaNo ratings yet
- Elm04 10solutions - Doc 0Document13 pagesElm04 10solutions - Doc 0venkatvarsha100% (2)
- Drug Use in Renal and Hepatic Disorders.: Chapter-VDocument30 pagesDrug Use in Renal and Hepatic Disorders.: Chapter-VBandameedi RamuNo ratings yet
- Dexamethasone Suppression TestDocument3 pagesDexamethasone Suppression TestMelisa MalikNo ratings yet
- Diagnostic Tests For Cushing'sDocument6 pagesDiagnostic Tests For Cushing'sChristine ParrillaNo ratings yet
- Case Pre.. Cushing SyndromeDocument11 pagesCase Pre.. Cushing Syndromedee_day_8No ratings yet
- Pharmacokinetic of Simvastatin Study in Malaysian SubjectsDocument6 pagesPharmacokinetic of Simvastatin Study in Malaysian SubjectsNur Ilham SaputraNo ratings yet
- Anti-Diabetic DrugsDocument14 pagesAnti-Diabetic DrugsHossam Elden Helmy HaridyNo ratings yet
- Adrenocortical HyperfunctionDocument132 pagesAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- The Plasma Sugar, Free Fatty Acid, Cortisol, and Growth Hormone Response Insulin. I. in Control SubjectsDocument8 pagesThe Plasma Sugar, Free Fatty Acid, Cortisol, and Growth Hormone Response Insulin. I. in Control SubjectsYng TangNo ratings yet
- Medicine DescriptionDocument16 pagesMedicine DescriptionMichele SanchezNo ratings yet
- EJDEXDocument11 pagesEJDEXAirene ZulfikarNo ratings yet
- REGLAN Injection (Metoclopramide Injection, USP) RX OnlyDocument15 pagesREGLAN Injection (Metoclopramide Injection, USP) RX OnlydpkkrsterNo ratings yet
- Lamotrigine Therapeutic Drug Monitoring in A TertiaryDocument7 pagesLamotrigine Therapeutic Drug Monitoring in A TertiarydanielguerinNo ratings yet
- CLC 4960230910Document7 pagesCLC 4960230910walnut21No ratings yet
- Pier Vincenzo Piazza Et Al - Glucocorticoids Have State-Dependent Stimulant Effects On The Mesencephalic Dopaminergic TransmissionDocument5 pagesPier Vincenzo Piazza Et Al - Glucocorticoids Have State-Dependent Stimulant Effects On The Mesencephalic Dopaminergic TransmissionSour60No ratings yet
- 10-Disease State PharmacokineticsDocument44 pages10-Disease State PharmacokineticsKerolus Joseph AminNo ratings yet
- 2008 - Plasma Amantadine Concentrations in Patients With Parkinson's DiseaseDocument3 pages2008 - Plasma Amantadine Concentrations in Patients With Parkinson's DiseaseniltonfrazaoNo ratings yet
- PIII-74 Pro-76: Society For Clinical Pharmacology and TherapeuticsDocument1 pagePIII-74 Pro-76: Society For Clinical Pharmacology and Therapeuticsdev darma karinggaNo ratings yet
- DESOXIMETASONE-desoximetasone Cream Padagis Israel Pharmaceuticals LTDDocument7 pagesDESOXIMETASONE-desoximetasone Cream Padagis Israel Pharmaceuticals LTDRizky Akbar LatifNo ratings yet
- Analysis of Plasm LipoproteinDocument10 pagesAnalysis of Plasm LipoproteinWilson KhawNo ratings yet
- Interaction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionDocument5 pagesInteraction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionDianWindiAmaliaNo ratings yet
- AMPT-induced Monoamine Depletion in Humans: Evaluation of Two Alternative (123I) IBZM SPECT ProceduresDocument7 pagesAMPT-induced Monoamine Depletion in Humans: Evaluation of Two Alternative (123I) IBZM SPECT ProceduresMihaela ToaderNo ratings yet
- Definition/Description: Rheumatoid Arthritis Asthma Multiple SclerosisDocument8 pagesDefinition/Description: Rheumatoid Arthritis Asthma Multiple SclerosisJhuRise Ann ManganaNo ratings yet
- Jama 269 17 035Document8 pagesJama 269 17 035Marcelo AlvesNo ratings yet
- TegretolDocument23 pagesTegretoldoniaNo ratings yet
- ch3 2019 PDFDocument15 pagesch3 2019 PDFMohammed AbdNo ratings yet
- Arora 2009Document6 pagesArora 2009ece142No ratings yet
- Cushing's Decision App - Glossary of Terms 2Document3 pagesCushing's Decision App - Glossary of Terms 2Erhan ErtuçNo ratings yet
- Ketoconazole in Cushing's Syndrome - Abrupt StopDocument10 pagesKetoconazole in Cushing's Syndrome - Abrupt Stopadrew1086No ratings yet
- 1 Handouts Clinical Microscopy Prof Gerard RamosDocument50 pages1 Handouts Clinical Microscopy Prof Gerard RamosNajifah DaudNo ratings yet
- Tegretol: RX Only Prescribing InformationDocument24 pagesTegretol: RX Only Prescribing InformationffffffNo ratings yet
- Farmako PDFDocument16 pagesFarmako PDFIsney HanindyaNo ratings yet
- Dexamethasone Suppression Tests - VCA Animal HospitalDocument5 pagesDexamethasone Suppression Tests - VCA Animal HospitaldmantsioNo ratings yet
- qt753782f6 NosplashDocument4 pagesqt753782f6 NosplashGeorge E. FergusonNo ratings yet
- Data Sheet ProfalganDocument18 pagesData Sheet Profalganhansen-jcNo ratings yet
- Antibiotik For Renal FailureDocument6 pagesAntibiotik For Renal FailureWidhy Joss BangetzNo ratings yet
- CreatinineDocument5 pagesCreatininefathiyyahnurulNo ratings yet
- For Cushing's Syndrome Caused by Long-Term Corticosteroid Medicine UseDocument6 pagesFor Cushing's Syndrome Caused by Long-Term Corticosteroid Medicine UseErico OoiNo ratings yet
- Interaction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionDocument5 pagesInteraction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionEGA HPNo ratings yet
- Objective: This Study Was Undertaken To Compare The Efficacy and TolerabilityDocument3 pagesObjective: This Study Was Undertaken To Compare The Efficacy and Tolerabilitydini hanifaNo ratings yet
- SPEG DFT Handbook v1.0Document25 pagesSPEG DFT Handbook v1.0bassam alharaziNo ratings yet
- HAC63162 C 0009039003 Session28956 200323112824 PDFDocument3 pagesHAC63162 C 0009039003 Session28956 200323112824 PDFDidien LatareNo ratings yet
- CxuchingDocument4 pagesCxuchingMussme DelgadoNo ratings yet
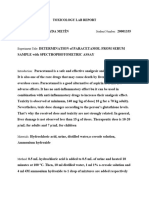
- Toxicology Lab Report ParacetamolDocument2 pagesToxicology Lab Report Paracetamolİlayda MetinNo ratings yet
- Volumetric Analysis of Some Hypoglycemic DsrugsDocument10 pagesVolumetric Analysis of Some Hypoglycemic Dsrugscyper zoonNo ratings yet
- Paracetamol Drug StudyDocument33 pagesParacetamol Drug Studycgmartelino.sbcmNo ratings yet
- Congenital Adrenal HyperplasiaDocument29 pagesCongenital Adrenal HyperplasiaMohan RaoNo ratings yet
- Mot Ilium TabDocument11 pagesMot Ilium TabChandra FatmaNo ratings yet
- The Cushing Syndrome: An Update On Diagnostic Tests: Determining CauseDocument12 pagesThe Cushing Syndrome: An Update On Diagnostic Tests: Determining CauseRay Erick RamosNo ratings yet
- High Dose Vs Low DoseDocument6 pagesHigh Dose Vs Low DosenivethitaNo ratings yet
- Glucose KitDocument2 pagesGlucose KitJuan Enrique Ramón OrellanaNo ratings yet
- 6.23.08 Dancel Endocrine BD RevDocument32 pages6.23.08 Dancel Endocrine BD Revkhaled_71111No ratings yet
- ENG Au - PI - PERFALGAN - V2.0 - 04sep2009Document20 pagesENG Au - PI - PERFALGAN - V2.0 - 04sep2009Amina TsunNo ratings yet
- 906 FullDocument14 pages906 FullMula Al-maNo ratings yet
- Adrenal Gland: Biochemistry by ZonesDocument12 pagesAdrenal Gland: Biochemistry by ZonesWael AlkhatibNo ratings yet
- Therapeutic Drug Monitoring of Levetiracetam in Daily Clinical Practice: High-Performance Liquid Chromatography Versus ImmunoassayDocument5 pagesTherapeutic Drug Monitoring of Levetiracetam in Daily Clinical Practice: High-Performance Liquid Chromatography Versus ImmunoassayMaria MendozaNo ratings yet
- Jfda 27 01 323Document9 pagesJfda 27 01 323Mohamed Medhat AliNo ratings yet
- Bioavailability and Bioequivalence. Therapeutic Drug MonitoringDocument3 pagesBioavailability and Bioequivalence. Therapeutic Drug MonitoringJoel MathewNo ratings yet
- Pharmaceutics 11 00336Document17 pagesPharmaceutics 11 00336Tyas PardedeNo ratings yet
- GentamiciniDocument11 pagesGentamiciniBenjie SisonNo ratings yet
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysFrom EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysNo ratings yet
- Insulin Autoimmune SyndromeDocument5 pagesInsulin Autoimmune SyndromeCota AncutaNo ratings yet
- Acromegalie Protocol Apr 2014Document13 pagesAcromegalie Protocol Apr 2014Cota AncutaNo ratings yet
- Primary Therapy of Cushing's Disease - Transsphenoidal Surgery and Pituitary IrradiationDocument10 pagesPrimary Therapy of Cushing's Disease - Transsphenoidal Surgery and Pituitary IrradiationCota AncutaNo ratings yet
- Conses Acromegalie 2012Document8 pagesConses Acromegalie 2012Cota AncutaNo ratings yet
- 10 1089@thy 2018 0198Document32 pages10 1089@thy 2018 0198Cota AncutaNo ratings yet
- Zan Ella 2018Document8 pagesZan Ella 2018Cota AncutaNo ratings yet
- 10 1089@thy 2017 0572Document10 pages10 1089@thy 2017 0572Cota AncutaNo ratings yet
- Daniels 2018Document14 pagesDaniels 2018Cota AncutaNo ratings yet
- InfertilityDocument224 pagesInfertilityCota AncutaNo ratings yet
- Kim 2017Document14 pagesKim 2017Cota AncutaNo ratings yet
- BRAF Gene Mutation TestsDocument5 pagesBRAF Gene Mutation TestsCota AncutaNo ratings yet
- PituitaryIncident FinalA-2Document24 pagesPituitaryIncident FinalA-2Cota AncutaNo ratings yet
- What Is Hypopara PDFDocument2 pagesWhat Is Hypopara PDFCota AncutaNo ratings yet
- IGF Generation TestDocument7 pagesIGF Generation TestCota AncutaNo ratings yet
- FINAL Standalone CAH GuidelineDocument48 pagesFINAL Standalone CAH GuidelineCota AncutaNo ratings yet
- A Quick Guide To HypoparathyroidismDocument24 pagesA Quick Guide To HypoparathyroidismCota AncutaNo ratings yet
- Guias para El Diagnostico y Tratamiento de Acromegalia AACE 2011Document44 pagesGuias para El Diagnostico y Tratamiento de Acromegalia AACE 2011Ricardo HemurNo ratings yet
- Surbir Singh Negi: Surbir99 - Negi@yahoo - Co.in, Surbir - Negi1@yahoo - Co.inDocument3 pagesSurbir Singh Negi: Surbir99 - Negi@yahoo - Co.in, Surbir - Negi1@yahoo - Co.insurbir_negi1100% (2)
- Signals and System PDFDocument38 pagesSignals and System PDFdeepakNo ratings yet
- PDF PMP Exam Quick Reference GuideDocument8 pagesPDF PMP Exam Quick Reference GuideNantha KumarNo ratings yet
- Employer BrandingDocument34 pagesEmployer BrandingTrinimafia100% (2)
- Hardtimes Analysis PDFDocument30 pagesHardtimes Analysis PDFV LkvNo ratings yet
- EXP-LG-080251 - 0 - SuportDocument2 pagesEXP-LG-080251 - 0 - SuportRazvan PanaNo ratings yet
- Numerical Methods For Partial Differential Equations: CAAM 452 Spring 2005 Instructor: Tim WarburtonDocument26 pagesNumerical Methods For Partial Differential Equations: CAAM 452 Spring 2005 Instructor: Tim WarburtonAqib SiddiqueNo ratings yet
- Instruction Book Manual de Instrucciones Livre D'InstructionsDocument79 pagesInstruction Book Manual de Instrucciones Livre D'InstructionsWilfrido RosadoNo ratings yet
- Vaskulitisi Malih Krvnih Sudova Bubrega: Etiopatogeneza, Dijagnostika I LečenjeDocument5 pagesVaskulitisi Malih Krvnih Sudova Bubrega: Etiopatogeneza, Dijagnostika I LečenjedjpaanNo ratings yet
- 4 - 20140515034803 - 1 Coase, R.H. 1937 The Nature of The FirmDocument24 pages4 - 20140515034803 - 1 Coase, R.H. 1937 The Nature of The FirmFelicia AprilianiNo ratings yet
- Pressure Relief Valve Scenario Summary: General Job DataDocument6 pagesPressure Relief Valve Scenario Summary: General Job DatajorgekarlosprNo ratings yet
- FCTM Chapter13 Abnormal-Emergency Operation BriefingDocument76 pagesFCTM Chapter13 Abnormal-Emergency Operation BriefingPunthep PunnotokNo ratings yet
- UntitledDocument22 pagesUntitledMoniNo ratings yet
- HashingDocument1,668 pagesHashingDinesh Reddy KommeraNo ratings yet
- Free Batchography: The Art of Batch Files Programming PDF DownloadDocument2 pagesFree Batchography: The Art of Batch Files Programming PDF Downloadgeorge capozziNo ratings yet
- CS2106 Lec1 IntroDocument97 pagesCS2106 Lec1 IntroweitsangNo ratings yet
- Sri Chaitanya IIT Academy, India: Grand Test-5Document31 pagesSri Chaitanya IIT Academy, India: Grand Test-5ashrithNo ratings yet
- Partial Differential Equations PDFDocument126 pagesPartial Differential Equations PDFManoj Bisht100% (1)
- UntitledDocument15 pagesUntitledAfiq AimanNo ratings yet
- Historical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaDocument15 pagesHistorical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaSonjce Marceva100% (2)
- 1st Quarter Exam in Math9Document3 pages1st Quarter Exam in Math9Robert Jay Mejorada100% (4)
- Trophy Urban Core Property: Houston, TexasDocument25 pagesTrophy Urban Core Property: Houston, Texasbella grandeNo ratings yet
- CV - Nicolas - Barabasqui Berlin - 230109 - 170104Document4 pagesCV - Nicolas - Barabasqui Berlin - 230109 - 170104Ricardo MelaNo ratings yet
- Chapter-1 Introduction of The Study: A Study On Financial Performance by Ratio AnalysisDocument47 pagesChapter-1 Introduction of The Study: A Study On Financial Performance by Ratio Analysisjayan panangadanNo ratings yet
- Training Day-1 V5Document85 pagesTraining Day-1 V5Wazabi MooNo ratings yet
- Siliporite Opx Pellets Revision 11 - 2017Document2 pagesSiliporite Opx Pellets Revision 11 - 2017Juan Victor Sulvaran Arellano100% (2)
- Monumentalizing Identities North SyrianDocument637 pagesMonumentalizing Identities North Syrianarheo111No ratings yet











































































































Download as pdf or txt
You might also like
- CASINO by Nicholas PileggiDocument238 pagesCASINO by Nicholas PileggiPutipufNo ratings yet
- Tanner Whitehouse TestDocument25 pagesTanner Whitehouse TestCota Ancuta0% (1)
- 4Z4TJDocument16 pages4Z4TJBimal Chutia100% (1)
- ENDOCRINOLOGY Handbook of Obesity 2003 PDFDocument1,056 pagesENDOCRINOLOGY Handbook of Obesity 2003 PDFCota AncutaNo ratings yet
- Elm04 10solutions - Doc 0Document13 pagesElm04 10solutions - Doc 0venkatvarsha100% (2)
- Drug Use in Renal and Hepatic Disorders.: Chapter-VDocument30 pagesDrug Use in Renal and Hepatic Disorders.: Chapter-VBandameedi RamuNo ratings yet
- Dexamethasone Suppression TestDocument3 pagesDexamethasone Suppression TestMelisa MalikNo ratings yet
- Diagnostic Tests For Cushing'sDocument6 pagesDiagnostic Tests For Cushing'sChristine ParrillaNo ratings yet
- Case Pre.. Cushing SyndromeDocument11 pagesCase Pre.. Cushing Syndromedee_day_8No ratings yet
- Pharmacokinetic of Simvastatin Study in Malaysian SubjectsDocument6 pagesPharmacokinetic of Simvastatin Study in Malaysian SubjectsNur Ilham SaputraNo ratings yet
- Anti-Diabetic DrugsDocument14 pagesAnti-Diabetic DrugsHossam Elden Helmy HaridyNo ratings yet
- Adrenocortical HyperfunctionDocument132 pagesAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- The Plasma Sugar, Free Fatty Acid, Cortisol, and Growth Hormone Response Insulin. I. in Control SubjectsDocument8 pagesThe Plasma Sugar, Free Fatty Acid, Cortisol, and Growth Hormone Response Insulin. I. in Control SubjectsYng TangNo ratings yet
- Medicine DescriptionDocument16 pagesMedicine DescriptionMichele SanchezNo ratings yet
- EJDEXDocument11 pagesEJDEXAirene ZulfikarNo ratings yet
- REGLAN Injection (Metoclopramide Injection, USP) RX OnlyDocument15 pagesREGLAN Injection (Metoclopramide Injection, USP) RX OnlydpkkrsterNo ratings yet
- Lamotrigine Therapeutic Drug Monitoring in A TertiaryDocument7 pagesLamotrigine Therapeutic Drug Monitoring in A TertiarydanielguerinNo ratings yet
- CLC 4960230910Document7 pagesCLC 4960230910walnut21No ratings yet
- Pier Vincenzo Piazza Et Al - Glucocorticoids Have State-Dependent Stimulant Effects On The Mesencephalic Dopaminergic TransmissionDocument5 pagesPier Vincenzo Piazza Et Al - Glucocorticoids Have State-Dependent Stimulant Effects On The Mesencephalic Dopaminergic TransmissionSour60No ratings yet
- 10-Disease State PharmacokineticsDocument44 pages10-Disease State PharmacokineticsKerolus Joseph AminNo ratings yet
- 2008 - Plasma Amantadine Concentrations in Patients With Parkinson's DiseaseDocument3 pages2008 - Plasma Amantadine Concentrations in Patients With Parkinson's DiseaseniltonfrazaoNo ratings yet
- PIII-74 Pro-76: Society For Clinical Pharmacology and TherapeuticsDocument1 pagePIII-74 Pro-76: Society For Clinical Pharmacology and Therapeuticsdev darma karinggaNo ratings yet
- DESOXIMETASONE-desoximetasone Cream Padagis Israel Pharmaceuticals LTDDocument7 pagesDESOXIMETASONE-desoximetasone Cream Padagis Israel Pharmaceuticals LTDRizky Akbar LatifNo ratings yet
- Analysis of Plasm LipoproteinDocument10 pagesAnalysis of Plasm LipoproteinWilson KhawNo ratings yet
- Interaction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionDocument5 pagesInteraction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionDianWindiAmaliaNo ratings yet
- AMPT-induced Monoamine Depletion in Humans: Evaluation of Two Alternative (123I) IBZM SPECT ProceduresDocument7 pagesAMPT-induced Monoamine Depletion in Humans: Evaluation of Two Alternative (123I) IBZM SPECT ProceduresMihaela ToaderNo ratings yet
- Definition/Description: Rheumatoid Arthritis Asthma Multiple SclerosisDocument8 pagesDefinition/Description: Rheumatoid Arthritis Asthma Multiple SclerosisJhuRise Ann ManganaNo ratings yet
- Jama 269 17 035Document8 pagesJama 269 17 035Marcelo AlvesNo ratings yet
- TegretolDocument23 pagesTegretoldoniaNo ratings yet
- ch3 2019 PDFDocument15 pagesch3 2019 PDFMohammed AbdNo ratings yet
- Arora 2009Document6 pagesArora 2009ece142No ratings yet
- Cushing's Decision App - Glossary of Terms 2Document3 pagesCushing's Decision App - Glossary of Terms 2Erhan ErtuçNo ratings yet
- Ketoconazole in Cushing's Syndrome - Abrupt StopDocument10 pagesKetoconazole in Cushing's Syndrome - Abrupt Stopadrew1086No ratings yet
- 1 Handouts Clinical Microscopy Prof Gerard RamosDocument50 pages1 Handouts Clinical Microscopy Prof Gerard RamosNajifah DaudNo ratings yet
- Tegretol: RX Only Prescribing InformationDocument24 pagesTegretol: RX Only Prescribing InformationffffffNo ratings yet
- Farmako PDFDocument16 pagesFarmako PDFIsney HanindyaNo ratings yet
- Dexamethasone Suppression Tests - VCA Animal HospitalDocument5 pagesDexamethasone Suppression Tests - VCA Animal HospitaldmantsioNo ratings yet
- qt753782f6 NosplashDocument4 pagesqt753782f6 NosplashGeorge E. FergusonNo ratings yet
- Data Sheet ProfalganDocument18 pagesData Sheet Profalganhansen-jcNo ratings yet
- Antibiotik For Renal FailureDocument6 pagesAntibiotik For Renal FailureWidhy Joss BangetzNo ratings yet
- CreatinineDocument5 pagesCreatininefathiyyahnurulNo ratings yet
- For Cushing's Syndrome Caused by Long-Term Corticosteroid Medicine UseDocument6 pagesFor Cushing's Syndrome Caused by Long-Term Corticosteroid Medicine UseErico OoiNo ratings yet
- Interaction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionDocument5 pagesInteraction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionEGA HPNo ratings yet
- Objective: This Study Was Undertaken To Compare The Efficacy and TolerabilityDocument3 pagesObjective: This Study Was Undertaken To Compare The Efficacy and Tolerabilitydini hanifaNo ratings yet
- SPEG DFT Handbook v1.0Document25 pagesSPEG DFT Handbook v1.0bassam alharaziNo ratings yet
- HAC63162 C 0009039003 Session28956 200323112824 PDFDocument3 pagesHAC63162 C 0009039003 Session28956 200323112824 PDFDidien LatareNo ratings yet
- CxuchingDocument4 pagesCxuchingMussme DelgadoNo ratings yet
- Toxicology Lab Report ParacetamolDocument2 pagesToxicology Lab Report Paracetamolİlayda MetinNo ratings yet
- Volumetric Analysis of Some Hypoglycemic DsrugsDocument10 pagesVolumetric Analysis of Some Hypoglycemic Dsrugscyper zoonNo ratings yet
- Paracetamol Drug StudyDocument33 pagesParacetamol Drug Studycgmartelino.sbcmNo ratings yet
- Congenital Adrenal HyperplasiaDocument29 pagesCongenital Adrenal HyperplasiaMohan RaoNo ratings yet
- Mot Ilium TabDocument11 pagesMot Ilium TabChandra FatmaNo ratings yet
- The Cushing Syndrome: An Update On Diagnostic Tests: Determining CauseDocument12 pagesThe Cushing Syndrome: An Update On Diagnostic Tests: Determining CauseRay Erick RamosNo ratings yet
- High Dose Vs Low DoseDocument6 pagesHigh Dose Vs Low DosenivethitaNo ratings yet
- Glucose KitDocument2 pagesGlucose KitJuan Enrique Ramón OrellanaNo ratings yet
- 6.23.08 Dancel Endocrine BD RevDocument32 pages6.23.08 Dancel Endocrine BD Revkhaled_71111No ratings yet
- ENG Au - PI - PERFALGAN - V2.0 - 04sep2009Document20 pagesENG Au - PI - PERFALGAN - V2.0 - 04sep2009Amina TsunNo ratings yet
- 906 FullDocument14 pages906 FullMula Al-maNo ratings yet
- Adrenal Gland: Biochemistry by ZonesDocument12 pagesAdrenal Gland: Biochemistry by ZonesWael AlkhatibNo ratings yet
- Therapeutic Drug Monitoring of Levetiracetam in Daily Clinical Practice: High-Performance Liquid Chromatography Versus ImmunoassayDocument5 pagesTherapeutic Drug Monitoring of Levetiracetam in Daily Clinical Practice: High-Performance Liquid Chromatography Versus ImmunoassayMaria MendozaNo ratings yet
- Jfda 27 01 323Document9 pagesJfda 27 01 323Mohamed Medhat AliNo ratings yet
- Bioavailability and Bioequivalence. Therapeutic Drug MonitoringDocument3 pagesBioavailability and Bioequivalence. Therapeutic Drug MonitoringJoel MathewNo ratings yet
- Pharmaceutics 11 00336Document17 pagesPharmaceutics 11 00336Tyas PardedeNo ratings yet
- GentamiciniDocument11 pagesGentamiciniBenjie SisonNo ratings yet
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysFrom EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysNo ratings yet
- Insulin Autoimmune SyndromeDocument5 pagesInsulin Autoimmune SyndromeCota AncutaNo ratings yet
- Acromegalie Protocol Apr 2014Document13 pagesAcromegalie Protocol Apr 2014Cota AncutaNo ratings yet
- Primary Therapy of Cushing's Disease - Transsphenoidal Surgery and Pituitary IrradiationDocument10 pagesPrimary Therapy of Cushing's Disease - Transsphenoidal Surgery and Pituitary IrradiationCota AncutaNo ratings yet
- Conses Acromegalie 2012Document8 pagesConses Acromegalie 2012Cota AncutaNo ratings yet
- 10 1089@thy 2018 0198Document32 pages10 1089@thy 2018 0198Cota AncutaNo ratings yet
- Zan Ella 2018Document8 pagesZan Ella 2018Cota AncutaNo ratings yet
- 10 1089@thy 2017 0572Document10 pages10 1089@thy 2017 0572Cota AncutaNo ratings yet
- Daniels 2018Document14 pagesDaniels 2018Cota AncutaNo ratings yet
- InfertilityDocument224 pagesInfertilityCota AncutaNo ratings yet
- Kim 2017Document14 pagesKim 2017Cota AncutaNo ratings yet
- BRAF Gene Mutation TestsDocument5 pagesBRAF Gene Mutation TestsCota AncutaNo ratings yet
- PituitaryIncident FinalA-2Document24 pagesPituitaryIncident FinalA-2Cota AncutaNo ratings yet
- What Is Hypopara PDFDocument2 pagesWhat Is Hypopara PDFCota AncutaNo ratings yet
- IGF Generation TestDocument7 pagesIGF Generation TestCota AncutaNo ratings yet
- FINAL Standalone CAH GuidelineDocument48 pagesFINAL Standalone CAH GuidelineCota AncutaNo ratings yet
- A Quick Guide To HypoparathyroidismDocument24 pagesA Quick Guide To HypoparathyroidismCota AncutaNo ratings yet
- Guias para El Diagnostico y Tratamiento de Acromegalia AACE 2011Document44 pagesGuias para El Diagnostico y Tratamiento de Acromegalia AACE 2011Ricardo HemurNo ratings yet
- Surbir Singh Negi: Surbir99 - Negi@yahoo - Co.in, Surbir - Negi1@yahoo - Co.inDocument3 pagesSurbir Singh Negi: Surbir99 - Negi@yahoo - Co.in, Surbir - Negi1@yahoo - Co.insurbir_negi1100% (2)
- Signals and System PDFDocument38 pagesSignals and System PDFdeepakNo ratings yet
- PDF PMP Exam Quick Reference GuideDocument8 pagesPDF PMP Exam Quick Reference GuideNantha KumarNo ratings yet
- Employer BrandingDocument34 pagesEmployer BrandingTrinimafia100% (2)
- Hardtimes Analysis PDFDocument30 pagesHardtimes Analysis PDFV LkvNo ratings yet
- EXP-LG-080251 - 0 - SuportDocument2 pagesEXP-LG-080251 - 0 - SuportRazvan PanaNo ratings yet
- Numerical Methods For Partial Differential Equations: CAAM 452 Spring 2005 Instructor: Tim WarburtonDocument26 pagesNumerical Methods For Partial Differential Equations: CAAM 452 Spring 2005 Instructor: Tim WarburtonAqib SiddiqueNo ratings yet
- Instruction Book Manual de Instrucciones Livre D'InstructionsDocument79 pagesInstruction Book Manual de Instrucciones Livre D'InstructionsWilfrido RosadoNo ratings yet
- Vaskulitisi Malih Krvnih Sudova Bubrega: Etiopatogeneza, Dijagnostika I LečenjeDocument5 pagesVaskulitisi Malih Krvnih Sudova Bubrega: Etiopatogeneza, Dijagnostika I LečenjedjpaanNo ratings yet
- 4 - 20140515034803 - 1 Coase, R.H. 1937 The Nature of The FirmDocument24 pages4 - 20140515034803 - 1 Coase, R.H. 1937 The Nature of The FirmFelicia AprilianiNo ratings yet
- Pressure Relief Valve Scenario Summary: General Job DataDocument6 pagesPressure Relief Valve Scenario Summary: General Job DatajorgekarlosprNo ratings yet
- FCTM Chapter13 Abnormal-Emergency Operation BriefingDocument76 pagesFCTM Chapter13 Abnormal-Emergency Operation BriefingPunthep PunnotokNo ratings yet
- UntitledDocument22 pagesUntitledMoniNo ratings yet
- HashingDocument1,668 pagesHashingDinesh Reddy KommeraNo ratings yet
- Free Batchography: The Art of Batch Files Programming PDF DownloadDocument2 pagesFree Batchography: The Art of Batch Files Programming PDF Downloadgeorge capozziNo ratings yet
- CS2106 Lec1 IntroDocument97 pagesCS2106 Lec1 IntroweitsangNo ratings yet
- Sri Chaitanya IIT Academy, India: Grand Test-5Document31 pagesSri Chaitanya IIT Academy, India: Grand Test-5ashrithNo ratings yet
- Partial Differential Equations PDFDocument126 pagesPartial Differential Equations PDFManoj Bisht100% (1)
- UntitledDocument15 pagesUntitledAfiq AimanNo ratings yet
- Historical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaDocument15 pagesHistorical Change and Ceramic Tradition: The Case of Macedonia - Zoi KotitsaSonjce Marceva100% (2)
- 1st Quarter Exam in Math9Document3 pages1st Quarter Exam in Math9Robert Jay Mejorada100% (4)
- Trophy Urban Core Property: Houston, TexasDocument25 pagesTrophy Urban Core Property: Houston, Texasbella grandeNo ratings yet
- CV - Nicolas - Barabasqui Berlin - 230109 - 170104Document4 pagesCV - Nicolas - Barabasqui Berlin - 230109 - 170104Ricardo MelaNo ratings yet
- Chapter-1 Introduction of The Study: A Study On Financial Performance by Ratio AnalysisDocument47 pagesChapter-1 Introduction of The Study: A Study On Financial Performance by Ratio Analysisjayan panangadanNo ratings yet
- Training Day-1 V5Document85 pagesTraining Day-1 V5Wazabi MooNo ratings yet
- Siliporite Opx Pellets Revision 11 - 2017Document2 pagesSiliporite Opx Pellets Revision 11 - 2017Juan Victor Sulvaran Arellano100% (2)
- Monumentalizing Identities North SyrianDocument637 pagesMonumentalizing Identities North Syrianarheo111No ratings yet