
The Inflammatory Process by BSolok
The Inflammatory Process by BSolok
You might also like
- Robbins Pathology - Chapter 3 TransDocument18 pagesRobbins Pathology - Chapter 3 Transnath nath100% (7)
- Teves, J. Owen NCP Risk For Infection R:T Episiotomy WoundDocument3 pagesTeves, J. Owen NCP Risk For Infection R:T Episiotomy WoundJoi Owen Teves100% (2)
- Nursing Care Plan-AguilarDocument3 pagesNursing Care Plan-AguilarphearlieNo ratings yet
- NCP Template W InferenceDocument5 pagesNCP Template W InferenceVannesa TarifaNo ratings yet
- Chapter 03 Inflammation and RepairDocument17 pagesChapter 03 Inflammation and RepairLe Nu Huyen TrangNo ratings yet
- Inflammation - SPC MLS 2B - Histopath LecDocument4 pagesInflammation - SPC MLS 2B - Histopath LecMa. Erikah CancioNo ratings yet
- Presentasi Traumatic Wound Management - A Comprehensive Wound Management Forum Discussion & Hands-On ModelsDocument57 pagesPresentasi Traumatic Wound Management - A Comprehensive Wound Management Forum Discussion & Hands-On ModelsDadek PradnyanaNo ratings yet
- BurnsDocument3 pagesBurnsCharmaine PilacNo ratings yet
- Wound Care LengkapDocument49 pagesWound Care LengkapintanNo ratings yet
- Management of Lower Limb Trauma Open Wounds and FracturesDocument44 pagesManagement of Lower Limb Trauma Open Wounds and FracturesRumaicha ChachaNo ratings yet
- NCP 1 CSDocument2 pagesNCP 1 CSjuliechan_17mjNo ratings yet
- Burn Wound CareDocument53 pagesBurn Wound Carenikinikko100% (1)
- 1.02 Sugical Conditions of The Skin and Subcutaneous Tissue (Part2)Document6 pages1.02 Sugical Conditions of The Skin and Subcutaneous Tissue (Part2)Klyn Agagon GayodanNo ratings yet
- SJS NCPDocument4 pagesSJS NCPAira Alaro50% (2)
- Wound Classification and ManagementDocument50 pagesWound Classification and ManagementAlex HoNo ratings yet
- 3.inflammation & Wound HealingDocument78 pages3.inflammation & Wound HealingEsaias ChanieNo ratings yet
- Drug NameDocument4 pagesDrug Namecheanne003No ratings yet
- Case ScenarioDocument7 pagesCase ScenarioReann LeeNo ratings yet
- CPAT3201 2020 Inflammation Lecture 1 NOTESDocument50 pagesCPAT3201 2020 Inflammation Lecture 1 NOTESJoshua KaoNo ratings yet
- Case ReportDocument19 pagesCase ReportHK FreeNo ratings yet
- Ncp-Case Pre Impaired Tissue Integrity-1Document2 pagesNcp-Case Pre Impaired Tissue Integrity-1Jade HemmingsNo ratings yet
- Electrical Burn: Xantipphy Mae IbrahimDocument32 pagesElectrical Burn: Xantipphy Mae IbrahimMinette EmmanuelNo ratings yet
- Pulpal and Periapical PathologyDocument101 pagesPulpal and Periapical Pathologyammara100% (1)
- Wound Healing and Its DisordersDocument39 pagesWound Healing and Its Disordersmahdi aljamalNo ratings yet
- Histopath Lec - Week 3 - Topic 4Document2 pagesHistopath Lec - Week 3 - Topic 4Juren LasagaNo ratings yet
- Lesi Rongga Mulut Diagnosis Dan Penanganannya PDFDocument35 pagesLesi Rongga Mulut Diagnosis Dan Penanganannya PDFFhaNo ratings yet
- Odontogenic Infection - 4 PDFDocument10 pagesOdontogenic Infection - 4 PDFTanjir 247No ratings yet
- Appendectomy NCPDocument2 pagesAppendectomy NCPMyra AtuleNo ratings yet
- Pulp Diseases in ChildrenDocument50 pagesPulp Diseases in ChildrenهجرسNo ratings yet
- ImpetigoDocument3 pagesImpetigoLynṅNo ratings yet
- Adobe Scan 21 Jan 2024Document14 pagesAdobe Scan 21 Jan 2024pandapriyanka565No ratings yet
- Subjective: Independent:: Nursing Care PlanDocument2 pagesSubjective: Independent:: Nursing Care PlanJade HemmingsNo ratings yet
- Inflammation and WOund HealingDocument122 pagesInflammation and WOund HealingDeb SNo ratings yet
- Cannulation of The AVF Ch5Document4 pagesCannulation of The AVF Ch5En RasNo ratings yet
- McAlinden Hordeolum PDFDocument3 pagesMcAlinden Hordeolum PDFNur Rakhma AkmaliaNo ratings yet
- Nursing Care Plan - RabiesDocument2 pagesNursing Care Plan - Rabiesderic89% (9)
- NCP Impaired Skin IntegrityDocument2 pagesNCP Impaired Skin IntegrityEden Marie Francisco100% (2)
- Odontogenic Infections of The Head & NeckDocument76 pagesOdontogenic Infections of The Head & NeckKhalid TahaNo ratings yet
- Wound-TypesDocument1 pageWound-TypesJamie W.No ratings yet
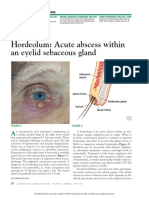
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Wound Care, Suture Materials & Suturing TechniquesDocument80 pagesWound Care, Suture Materials & Suturing TechniquesAlwin PrasetyaNo ratings yet
- Actinomycosis and NOMADocument10 pagesActinomycosis and NOMASOUMYA A DR, DEPT.OF DENTAL SCIENCES,SRIHERNo ratings yet
- Saint Paul University Dumaguete College of Nursing Nursing Care Plan FormDocument9 pagesSaint Paul University Dumaguete College of Nursing Nursing Care Plan FormManuel Jacob YradNo ratings yet
- Classification of Wounds: Definition: It Is A Bruise, Usually Produced by AnDocument3 pagesClassification of Wounds: Definition: It Is A Bruise, Usually Produced by AnIvyLove CatalanNo ratings yet
- Pascua NCPDocument2 pagesPascua NCPLawrene Landingin IralNo ratings yet
- Nursing CS Wound-Types 01Document1 pageNursing CS Wound-Types 01Jazzmine GuraNo ratings yet
- Bu VonnyDocument41 pagesBu VonnyZola IsmuNo ratings yet
- Pulpal Disease: Dr. Mohamed El-Saeed Lecturer of EndodonticsDocument10 pagesPulpal Disease: Dr. Mohamed El-Saeed Lecturer of EndodonticsAbdelrhman AdelNo ratings yet
- Nursing Care Plan FormDocument3 pagesNursing Care Plan FormHanniel MontecalboNo ratings yet
- 2 Cytopathologic Changes in DiseaseDocument10 pages2 Cytopathologic Changes in DiseaseSandy GorricetaNo ratings yet
- Introduction To Reconstructive and Aesthetic Plastic SurgeryDocument15 pagesIntroduction To Reconstructive and Aesthetic Plastic SurgeryAllene PaderangaNo ratings yet
- 2018 KLWC Hansen's RevisedDocument1 page2018 KLWC Hansen's RevisedLinda Luckstead BenskinNo ratings yet
- Acute InflammationDocument20 pagesAcute Inflammationbpt20% (2)
- Oxytetracycline - Casimero (Group41)Document2 pagesOxytetracycline - Casimero (Group41)Hannah Angela CasimeroNo ratings yet
- Group 2Document6 pagesGroup 2VIVIEN CONSIGNANo ratings yet
- Nursing Assessment S - O Pt. May ManifestDocument4 pagesNursing Assessment S - O Pt. May Manifestk_a1990No ratings yet
- (From The Departme, U of of The Johns Hopkins University) : Culin Used. UsingDocument24 pages(From The Departme, U of of The Johns Hopkins University) : Culin Used. UsingAlexNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Reproduction in PlantsDocument12 pagesReproduction in PlantsAnand Philip PrasadNo ratings yet
- DETERMINANTS OF DEVIANT BEHAVIOUR AMONG ADOLESCENTS - Full PaperDocument5 pagesDETERMINANTS OF DEVIANT BEHAVIOUR AMONG ADOLESCENTS - Full PaperAdina CipariuNo ratings yet
- Drug InteractionsDocument43 pagesDrug Interactionstry_dinaa100% (1)
- In-Vitro and In-Vivo Anti-In Ammatory Activity of Andrographis Serpyllifolia (Rottl. Ex Vahl.) WTDocument7 pagesIn-Vitro and In-Vivo Anti-In Ammatory Activity of Andrographis Serpyllifolia (Rottl. Ex Vahl.) WTRamling PatrakarNo ratings yet
- Prepared By: Catherine Dela Rosa RamosDocument17 pagesPrepared By: Catherine Dela Rosa RamosOliver NaragNo ratings yet
- CONSULTATION On An EU Action Plan For Sharks Response: Scottish Sea Angling Conservation Network (SSACN)Document4 pagesCONSULTATION On An EU Action Plan For Sharks Response: Scottish Sea Angling Conservation Network (SSACN)The Scottish Sea Angling Conservation NetworkNo ratings yet
- Science and Ethical Dilemmas in The BlogosphereDocument26 pagesScience and Ethical Dilemmas in The BlogosphereFranck MarchisNo ratings yet
- Jurnal Paliatif 1Document10 pagesJurnal Paliatif 1Anisa SilviaNo ratings yet
- Aakash Home Assignment 3 SolutionsDocument7 pagesAakash Home Assignment 3 SolutionsPranav KapadiaNo ratings yet
- Compilation of Let QuestionsDocument17 pagesCompilation of Let QuestionsSharon Rose TayactacNo ratings yet
- Learning Activity 3 / Actividad de Aprendizaje 3 Evidence: I Can't Believe It! / Evidencia: ¡No Puedo Creerlo!Document3 pagesLearning Activity 3 / Actividad de Aprendizaje 3 Evidence: I Can't Believe It! / Evidencia: ¡No Puedo Creerlo!Daniel Felipe DuqueNo ratings yet
- Lazer Friedman The Network Structure of Exploration and Exploitation ASQDocument28 pagesLazer Friedman The Network Structure of Exploration and Exploitation ASQTime HenlyNo ratings yet
- Chapter 1 (1) .PPTX Micro-ParaDocument36 pagesChapter 1 (1) .PPTX Micro-ParaLorelie AsisNo ratings yet
- MDR Tecnical Sheet With Digital SignatureDocument103 pagesMDR Tecnical Sheet With Digital SignatureMamdouhNo ratings yet
- Extra Worksheet 2Document2 pagesExtra Worksheet 2Manar KanawatyNo ratings yet
- قائمة بأسماء خريجين الدكتوراة من عام 1964-2005مDocument346 pagesقائمة بأسماء خريجين الدكتوراة من عام 1964-2005مSaaNo ratings yet
- Sample Mid-Term Test For IELTSDocument6 pagesSample Mid-Term Test For IELTSGia BảooNo ratings yet
- Guder Et Al Recommendations of The Working Group On Preanalytical Quality of The German Society For Clinical Chemistry and Lab Medecine EnglishDocument41 pagesGuder Et Al Recommendations of The Working Group On Preanalytical Quality of The German Society For Clinical Chemistry and Lab Medecine Englishrild278111100% (1)
- NOUN 2019 2 POP Final Exam TimetableDocument18 pagesNOUN 2019 2 POP Final Exam TimetableAlade AyodeleNo ratings yet
- Phosphate DeterminationDocument5 pagesPhosphate DeterminationCaryl FrancheteNo ratings yet
- Integrated Science NotesDocument17 pagesIntegrated Science NotesannmarieNo ratings yet
- Biopharmaceutics Classification SystemDocument3 pagesBiopharmaceutics Classification SystemAnti MariantiNo ratings yet
- Transport System in PlantDocument16 pagesTransport System in PlantAbu-Omar50% (4)
- Experiment No. 2 CarbohydratesDocument2 pagesExperiment No. 2 CarbohydratesYellow100% (1)
- Unicellular Organisms Multicellular OrganismsDocument5 pagesUnicellular Organisms Multicellular OrganismsDeasserei TatelNo ratings yet
- GCSE PracticalsDocument4 pagesGCSE PracticalsprakashvcNo ratings yet
- MCB 150L Problem Set 4Document2 pagesMCB 150L Problem Set 4John SmithNo ratings yet
- MedicDocument5 pagesMedicJoao Vitor StuchiNo ratings yet
- Number Answer Notes MarksDocument7 pagesNumber Answer Notes MarksMeenakshie Chaudrie100% (1)
- Importance of Biological Museum To Biology Students: A Study of Kaduna State College of EducationDocument36 pagesImportance of Biological Museum To Biology Students: A Study of Kaduna State College of EducationGODSWILL EMMANUELNo ratings yet























































































Download as pdf or txt
You might also like
- Robbins Pathology - Chapter 3 TransDocument18 pagesRobbins Pathology - Chapter 3 Transnath nath100% (7)
- Teves, J. Owen NCP Risk For Infection R:T Episiotomy WoundDocument3 pagesTeves, J. Owen NCP Risk For Infection R:T Episiotomy WoundJoi Owen Teves100% (2)
- Nursing Care Plan-AguilarDocument3 pagesNursing Care Plan-AguilarphearlieNo ratings yet
- NCP Template W InferenceDocument5 pagesNCP Template W InferenceVannesa TarifaNo ratings yet
- Chapter 03 Inflammation and RepairDocument17 pagesChapter 03 Inflammation and RepairLe Nu Huyen TrangNo ratings yet
- Inflammation - SPC MLS 2B - Histopath LecDocument4 pagesInflammation - SPC MLS 2B - Histopath LecMa. Erikah CancioNo ratings yet
- Presentasi Traumatic Wound Management - A Comprehensive Wound Management Forum Discussion & Hands-On ModelsDocument57 pagesPresentasi Traumatic Wound Management - A Comprehensive Wound Management Forum Discussion & Hands-On ModelsDadek PradnyanaNo ratings yet
- BurnsDocument3 pagesBurnsCharmaine PilacNo ratings yet
- Wound Care LengkapDocument49 pagesWound Care LengkapintanNo ratings yet
- Management of Lower Limb Trauma Open Wounds and FracturesDocument44 pagesManagement of Lower Limb Trauma Open Wounds and FracturesRumaicha ChachaNo ratings yet
- NCP 1 CSDocument2 pagesNCP 1 CSjuliechan_17mjNo ratings yet
- Burn Wound CareDocument53 pagesBurn Wound Carenikinikko100% (1)
- 1.02 Sugical Conditions of The Skin and Subcutaneous Tissue (Part2)Document6 pages1.02 Sugical Conditions of The Skin and Subcutaneous Tissue (Part2)Klyn Agagon GayodanNo ratings yet
- SJS NCPDocument4 pagesSJS NCPAira Alaro50% (2)
- Wound Classification and ManagementDocument50 pagesWound Classification and ManagementAlex HoNo ratings yet
- 3.inflammation & Wound HealingDocument78 pages3.inflammation & Wound HealingEsaias ChanieNo ratings yet
- Drug NameDocument4 pagesDrug Namecheanne003No ratings yet
- Case ScenarioDocument7 pagesCase ScenarioReann LeeNo ratings yet
- CPAT3201 2020 Inflammation Lecture 1 NOTESDocument50 pagesCPAT3201 2020 Inflammation Lecture 1 NOTESJoshua KaoNo ratings yet
- Case ReportDocument19 pagesCase ReportHK FreeNo ratings yet
- Ncp-Case Pre Impaired Tissue Integrity-1Document2 pagesNcp-Case Pre Impaired Tissue Integrity-1Jade HemmingsNo ratings yet
- Electrical Burn: Xantipphy Mae IbrahimDocument32 pagesElectrical Burn: Xantipphy Mae IbrahimMinette EmmanuelNo ratings yet
- Pulpal and Periapical PathologyDocument101 pagesPulpal and Periapical Pathologyammara100% (1)
- Wound Healing and Its DisordersDocument39 pagesWound Healing and Its Disordersmahdi aljamalNo ratings yet
- Histopath Lec - Week 3 - Topic 4Document2 pagesHistopath Lec - Week 3 - Topic 4Juren LasagaNo ratings yet
- Lesi Rongga Mulut Diagnosis Dan Penanganannya PDFDocument35 pagesLesi Rongga Mulut Diagnosis Dan Penanganannya PDFFhaNo ratings yet
- Odontogenic Infection - 4 PDFDocument10 pagesOdontogenic Infection - 4 PDFTanjir 247No ratings yet
- Appendectomy NCPDocument2 pagesAppendectomy NCPMyra AtuleNo ratings yet
- Pulp Diseases in ChildrenDocument50 pagesPulp Diseases in ChildrenهجرسNo ratings yet
- ImpetigoDocument3 pagesImpetigoLynṅNo ratings yet
- Adobe Scan 21 Jan 2024Document14 pagesAdobe Scan 21 Jan 2024pandapriyanka565No ratings yet
- Subjective: Independent:: Nursing Care PlanDocument2 pagesSubjective: Independent:: Nursing Care PlanJade HemmingsNo ratings yet
- Inflammation and WOund HealingDocument122 pagesInflammation and WOund HealingDeb SNo ratings yet
- Cannulation of The AVF Ch5Document4 pagesCannulation of The AVF Ch5En RasNo ratings yet
- McAlinden Hordeolum PDFDocument3 pagesMcAlinden Hordeolum PDFNur Rakhma AkmaliaNo ratings yet
- Nursing Care Plan - RabiesDocument2 pagesNursing Care Plan - Rabiesderic89% (9)
- NCP Impaired Skin IntegrityDocument2 pagesNCP Impaired Skin IntegrityEden Marie Francisco100% (2)
- Odontogenic Infections of The Head & NeckDocument76 pagesOdontogenic Infections of The Head & NeckKhalid TahaNo ratings yet
- Wound-TypesDocument1 pageWound-TypesJamie W.No ratings yet
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Wound Care, Suture Materials & Suturing TechniquesDocument80 pagesWound Care, Suture Materials & Suturing TechniquesAlwin PrasetyaNo ratings yet
- Actinomycosis and NOMADocument10 pagesActinomycosis and NOMASOUMYA A DR, DEPT.OF DENTAL SCIENCES,SRIHERNo ratings yet
- Saint Paul University Dumaguete College of Nursing Nursing Care Plan FormDocument9 pagesSaint Paul University Dumaguete College of Nursing Nursing Care Plan FormManuel Jacob YradNo ratings yet
- Classification of Wounds: Definition: It Is A Bruise, Usually Produced by AnDocument3 pagesClassification of Wounds: Definition: It Is A Bruise, Usually Produced by AnIvyLove CatalanNo ratings yet
- Pascua NCPDocument2 pagesPascua NCPLawrene Landingin IralNo ratings yet
- Nursing CS Wound-Types 01Document1 pageNursing CS Wound-Types 01Jazzmine GuraNo ratings yet
- Bu VonnyDocument41 pagesBu VonnyZola IsmuNo ratings yet
- Pulpal Disease: Dr. Mohamed El-Saeed Lecturer of EndodonticsDocument10 pagesPulpal Disease: Dr. Mohamed El-Saeed Lecturer of EndodonticsAbdelrhman AdelNo ratings yet
- Nursing Care Plan FormDocument3 pagesNursing Care Plan FormHanniel MontecalboNo ratings yet
- 2 Cytopathologic Changes in DiseaseDocument10 pages2 Cytopathologic Changes in DiseaseSandy GorricetaNo ratings yet
- Introduction To Reconstructive and Aesthetic Plastic SurgeryDocument15 pagesIntroduction To Reconstructive and Aesthetic Plastic SurgeryAllene PaderangaNo ratings yet
- 2018 KLWC Hansen's RevisedDocument1 page2018 KLWC Hansen's RevisedLinda Luckstead BenskinNo ratings yet
- Acute InflammationDocument20 pagesAcute Inflammationbpt20% (2)
- Oxytetracycline - Casimero (Group41)Document2 pagesOxytetracycline - Casimero (Group41)Hannah Angela CasimeroNo ratings yet
- Group 2Document6 pagesGroup 2VIVIEN CONSIGNANo ratings yet
- Nursing Assessment S - O Pt. May ManifestDocument4 pagesNursing Assessment S - O Pt. May Manifestk_a1990No ratings yet
- (From The Departme, U of of The Johns Hopkins University) : Culin Used. UsingDocument24 pages(From The Departme, U of of The Johns Hopkins University) : Culin Used. UsingAlexNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Reproduction in PlantsDocument12 pagesReproduction in PlantsAnand Philip PrasadNo ratings yet
- DETERMINANTS OF DEVIANT BEHAVIOUR AMONG ADOLESCENTS - Full PaperDocument5 pagesDETERMINANTS OF DEVIANT BEHAVIOUR AMONG ADOLESCENTS - Full PaperAdina CipariuNo ratings yet
- Drug InteractionsDocument43 pagesDrug Interactionstry_dinaa100% (1)
- In-Vitro and In-Vivo Anti-In Ammatory Activity of Andrographis Serpyllifolia (Rottl. Ex Vahl.) WTDocument7 pagesIn-Vitro and In-Vivo Anti-In Ammatory Activity of Andrographis Serpyllifolia (Rottl. Ex Vahl.) WTRamling PatrakarNo ratings yet
- Prepared By: Catherine Dela Rosa RamosDocument17 pagesPrepared By: Catherine Dela Rosa RamosOliver NaragNo ratings yet
- CONSULTATION On An EU Action Plan For Sharks Response: Scottish Sea Angling Conservation Network (SSACN)Document4 pagesCONSULTATION On An EU Action Plan For Sharks Response: Scottish Sea Angling Conservation Network (SSACN)The Scottish Sea Angling Conservation NetworkNo ratings yet
- Science and Ethical Dilemmas in The BlogosphereDocument26 pagesScience and Ethical Dilemmas in The BlogosphereFranck MarchisNo ratings yet
- Jurnal Paliatif 1Document10 pagesJurnal Paliatif 1Anisa SilviaNo ratings yet
- Aakash Home Assignment 3 SolutionsDocument7 pagesAakash Home Assignment 3 SolutionsPranav KapadiaNo ratings yet
- Compilation of Let QuestionsDocument17 pagesCompilation of Let QuestionsSharon Rose TayactacNo ratings yet
- Learning Activity 3 / Actividad de Aprendizaje 3 Evidence: I Can't Believe It! / Evidencia: ¡No Puedo Creerlo!Document3 pagesLearning Activity 3 / Actividad de Aprendizaje 3 Evidence: I Can't Believe It! / Evidencia: ¡No Puedo Creerlo!Daniel Felipe DuqueNo ratings yet
- Lazer Friedman The Network Structure of Exploration and Exploitation ASQDocument28 pagesLazer Friedman The Network Structure of Exploration and Exploitation ASQTime HenlyNo ratings yet
- Chapter 1 (1) .PPTX Micro-ParaDocument36 pagesChapter 1 (1) .PPTX Micro-ParaLorelie AsisNo ratings yet
- MDR Tecnical Sheet With Digital SignatureDocument103 pagesMDR Tecnical Sheet With Digital SignatureMamdouhNo ratings yet
- Extra Worksheet 2Document2 pagesExtra Worksheet 2Manar KanawatyNo ratings yet
- قائمة بأسماء خريجين الدكتوراة من عام 1964-2005مDocument346 pagesقائمة بأسماء خريجين الدكتوراة من عام 1964-2005مSaaNo ratings yet
- Sample Mid-Term Test For IELTSDocument6 pagesSample Mid-Term Test For IELTSGia BảooNo ratings yet
- Guder Et Al Recommendations of The Working Group On Preanalytical Quality of The German Society For Clinical Chemistry and Lab Medecine EnglishDocument41 pagesGuder Et Al Recommendations of The Working Group On Preanalytical Quality of The German Society For Clinical Chemistry and Lab Medecine Englishrild278111100% (1)
- NOUN 2019 2 POP Final Exam TimetableDocument18 pagesNOUN 2019 2 POP Final Exam TimetableAlade AyodeleNo ratings yet
- Phosphate DeterminationDocument5 pagesPhosphate DeterminationCaryl FrancheteNo ratings yet
- Integrated Science NotesDocument17 pagesIntegrated Science NotesannmarieNo ratings yet
- Biopharmaceutics Classification SystemDocument3 pagesBiopharmaceutics Classification SystemAnti MariantiNo ratings yet
- Transport System in PlantDocument16 pagesTransport System in PlantAbu-Omar50% (4)
- Experiment No. 2 CarbohydratesDocument2 pagesExperiment No. 2 CarbohydratesYellow100% (1)
- Unicellular Organisms Multicellular OrganismsDocument5 pagesUnicellular Organisms Multicellular OrganismsDeasserei TatelNo ratings yet
- GCSE PracticalsDocument4 pagesGCSE PracticalsprakashvcNo ratings yet
- MCB 150L Problem Set 4Document2 pagesMCB 150L Problem Set 4John SmithNo ratings yet
- MedicDocument5 pagesMedicJoao Vitor StuchiNo ratings yet
- Number Answer Notes MarksDocument7 pagesNumber Answer Notes MarksMeenakshie Chaudrie100% (1)
- Importance of Biological Museum To Biology Students: A Study of Kaduna State College of EducationDocument36 pagesImportance of Biological Museum To Biology Students: A Study of Kaduna State College of EducationGODSWILL EMMANUELNo ratings yet