Download as pdf or txt
You might also like
- A Project Report On Equity Analysis On Indian IT Sector DasdDocument101 pagesA Project Report On Equity Analysis On Indian IT Sector DasdRamawatar Tawaniya100% (1)
- Impact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesDocument8 pagesImpact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesSri HariNo ratings yet
- Window of Implantation: Natural Vs Stimulated CyclesDocument30 pagesWindow of Implantation: Natural Vs Stimulated CyclesagusnestaalbugisyNo ratings yet
- PIIS0015028213017664Document2 pagesPIIS0015028213017664Tô ThuỷNo ratings yet
- Human Reproduction Fev 23 Artigo 1Document12 pagesHuman Reproduction Fev 23 Artigo 1viviane alexandreNo ratings yet
- ijrb-16-255Document6 pagesijrb-16-255ttriayatiNo ratings yet
- PIIS00150282990060Document4 pagesPIIS00150282990060lilou.magnaboscoNo ratings yet
- Piis1472648310001264 PDFDocument8 pagesPiis1472648310001264 PDFRahma Evasari LubisNo ratings yet
- Benchaib 2007Document8 pagesBenchaib 2007Tiffany LamNo ratings yet
- Ogs 21317Document8 pagesOgs 21317Carlos ParraNo ratings yet
- Effect of Progesterone Levels On The Day of HCG Trigger On Quality of Embryos in Icsi CyclesDocument6 pagesEffect of Progesterone Levels On The Day of HCG Trigger On Quality of Embryos in Icsi CyclesHerald Scholarly Open AccessNo ratings yet
- Procedures and Techniques-Clinical: ArtDocument2 pagesProcedures and Techniques-Clinical: ArtGeos KarNo ratings yet
- Transfusions and Neurodevelopmental Outcomes in Extremely Low Gestation Neonates Enrolled in The PENUT Trial: A Randomized Clinical TrialDocument8 pagesTransfusions and Neurodevelopmental Outcomes in Extremely Low Gestation Neonates Enrolled in The PENUT Trial: A Randomized Clinical Trialdarcyelle666No ratings yet
- Piis0015028211013112 PDFDocument2 pagesPiis0015028211013112 PDFGayathriMaranNo ratings yet
- Fertility & Sterility: A A B B C A ADocument1 pageFertility & Sterility: A A B B C A ASri HariNo ratings yet
- 14 10 Neoadjuvant Therapy in CA OvaryDocument32 pages14 10 Neoadjuvant Therapy in CA OvarydrarunoncoNo ratings yet
- A22 Comparisonof GN RHagonistandantagonistDocument5 pagesA22 Comparisonof GN RHagonistandantagonistSoumya NagarajanNo ratings yet
- Randomised Controlled Trial: 2020 John Wiley & Sons LTDDocument8 pagesRandomised Controlled Trial: 2020 John Wiley & Sons LTDGuruh PanjiNo ratings yet
- PIIS0002937820311923Document3 pagesPIIS0002937820311923FebbyNo ratings yet
- Preimplantation Genetic Diagnosis For Aneuploidy Screening in Patients With Unexplained Recurrent MiscarriagesDocument5 pagesPreimplantation Genetic Diagnosis For Aneuploidy Screening in Patients With Unexplained Recurrent MiscarriagesAkmilia VeraNo ratings yet
- Volume - 41 - 4 - 97 - 3 - MacacaDocument16 pagesVolume - 41 - 4 - 97 - 3 - MacacaAnindyaMustikaNo ratings yet
- Antimullerian Hormone But Not Follicle Stimulating Hormone Reflects Decline in Ovarian Reserve Associated With Oral Cyclophosphamide Use in Wegener SDocument1 pageAntimullerian Hormone But Not Follicle Stimulating Hormone Reflects Decline in Ovarian Reserve Associated With Oral Cyclophosphamide Use in Wegener SRocky.84No ratings yet
- Artículo 230222Document9 pagesArtículo 230222AnaNo ratings yet
- Gnrha Stop Protocol Versus Long Protocol in Poor Responder Ivf PatientsDocument6 pagesGnrha Stop Protocol Versus Long Protocol in Poor Responder Ivf PatientsGodha KiranaNo ratings yet
- Fendo 12 801026Document10 pagesFendo 12 801026Shilpa DuttaNo ratings yet
- Jcla 21956Document6 pagesJcla 21956Noah ZlinNo ratings yet
- Dex 367Document9 pagesDex 367Pradyumna SharmaNo ratings yet
- Lukaszuk Et Al. - 2005 - Optimization of Estradiol Supplementation During The Luteal Phase Improves The Pregnancy Rate in Women UnderDocument5 pagesLukaszuk Et Al. - 2005 - Optimization of Estradiol Supplementation During The Luteal Phase Improves The Pregnancy Rate in Women UnderKrzysztof ŁukaszukNo ratings yet
- JTaieb Clin Biochem E2 ArcDocument4 pagesJTaieb Clin Biochem E2 ArcFouad RahiouyNo ratings yet
- Original ArticleDocument26 pagesOriginal ArticleSantiago CeliNo ratings yet
- Peter Plateau - LH-HCG Effect in Human Assisted Fertility - II Simposio Reproducción Asistida QuirónDocument35 pagesPeter Plateau - LH-HCG Effect in Human Assisted Fertility - II Simposio Reproducción Asistida QuirónGrupo Hospitalario Quirón100% (1)
- Handling ComparingDocument13 pagesHandling ComparingNunik KhoirunnisaNo ratings yet
- Preterm Birth PreventionDocument10 pagesPreterm Birth PreventionEdwin Fabian Paz UrbanoNo ratings yet
- Pediatrics 2013 Penson E1897 907Document11 pagesPediatrics 2013 Penson E1897 907Hugo RoldanNo ratings yet
- Enrique Pérez de La Blanca - Las Gonadotropinas Son Intercambiables - II Simposio Reproducción Asistida QuirónDocument51 pagesEnrique Pérez de La Blanca - Las Gonadotropinas Son Intercambiables - II Simposio Reproducción Asistida QuirónGrupo Hospitalario QuirónNo ratings yet
- Natural Micronized Progesterone in IUIDocument3 pagesNatural Micronized Progesterone in IUIdrsantoshkalelearningNo ratings yet
- GNRH Agonists and Antagonists in Cyclophosphamide Induced Ovarian Damage Friend or Foe 2013 Fertility and SterilityDocument1 pageGNRH Agonists and Antagonists in Cyclophosphamide Induced Ovarian Damage Friend or Foe 2013 Fertility and SterilityRocky.84No ratings yet
- Jurnal Riza T1A-1Document17 pagesJurnal Riza T1A-1Riza RsNo ratings yet
- Poster Session I: Results: ResultsDocument2 pagesPoster Session I: Results: ResultsCoc OfclansNo ratings yet
- Expresion of GLP1 in Thyroid CarcinomaDocument9 pagesExpresion of GLP1 in Thyroid CarcinomaW Antonio Rivera MartínezNo ratings yet
- Soares Et Al., 2017 Steroid Hormones Interact With Natriuretic Peptide C ToDocument8 pagesSoares Et Al., 2017 Steroid Hormones Interact With Natriuretic Peptide C ToLudimilaNo ratings yet
- Journal Homepage: - : IntroductionDocument3 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Awwad Et Al-2015-BJOG An International Journal of Obstetrics & GynaecologyDocument9 pagesAwwad Et Al-2015-BJOG An International Journal of Obstetrics & GynaecologyHervi LaksariNo ratings yet
- Berkkanoglu 2019 30230393Document7 pagesBerkkanoglu 2019 30230393nathalieleclef125No ratings yet
- Middle East Fertility Society Journal: Maryam Eftekhar, Elham Naghshineh, Nosrat Neghab, Robabe HosseinisadatDocument4 pagesMiddle East Fertility Society Journal: Maryam Eftekhar, Elham Naghshineh, Nosrat Neghab, Robabe HosseinisadatM AbhiNo ratings yet
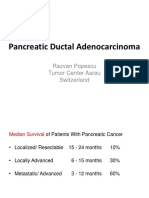
- Europe Balkan Course 2018 Systemic Management of Pancreatic Cancer PopescuDocument64 pagesEurope Balkan Course 2018 Systemic Management of Pancreatic Cancer PopescuCripto MonedeNo ratings yet
- Noãn BàoDocument1 pageNoãn Bàoinfo.linhnhuNo ratings yet
- Letter To The Editor: Serum Fibronectin and C-Reactive Protein in Prediction of Preterm DeliveryDocument5 pagesLetter To The Editor: Serum Fibronectin and C-Reactive Protein in Prediction of Preterm DeliveryCristina GaidargiNo ratings yet
- 2017 Article 141 Part6Document5 pages2017 Article 141 Part6Karina MonasaNo ratings yet
- Assisted Hatching For in Vitro Fertilization-Embryo Transfer: An UpdateDocument3 pagesAssisted Hatching For in Vitro Fertilization-Embryo Transfer: An UpdateandriNo ratings yet
- Amit Paper PublishedDocument4 pagesAmit Paper PublishedgnpobsNo ratings yet
- Comparison of in Vitro Fertilization Outcomes in ICSI Cycles After Human Sperm Preparation by Density Gradient Centrifugation and Direct Micro Swim-Up Without CentrifugationDocument5 pagesComparison of in Vitro Fertilization Outcomes in ICSI Cycles After Human Sperm Preparation by Density Gradient Centrifugation and Direct Micro Swim-Up Without Centrifugation周保亨No ratings yet
- Corea Del Sur 2019 SODIUMGLUCOSE COTRANSPORTER 2 INHIBOTOR FORDocument1 pageCorea Del Sur 2019 SODIUMGLUCOSE COTRANSPORTER 2 INHIBOTOR FORLaura GarciaNo ratings yet
- Adpkd CursDocument56 pagesAdpkd Cursplaiul mioriticNo ratings yet
- Clase EctopicoDocument24 pagesClase EctopicoJuan PicansNo ratings yet
- Progesterone CIDRbased Timed AI ProtocolsDocument18 pagesProgesterone CIDRbased Timed AI ProtocolsZavala H IrvingNo ratings yet
- Poster Session V: Study Design: ConclusionDocument1 pagePoster Session V: Study Design: ConclusionfujimeisterNo ratings yet
- R Eproductive Medicine/ Assisted R EproductionDocument9 pagesR Eproductive Medicine/ Assisted R EproductionsamiaNo ratings yet
- NEJMoa 2404656Document11 pagesNEJMoa 2404656luciaNo ratings yet
- Comparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialDocument5 pagesComparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialVindee VictoryNo ratings yet
- Executive SummaryDocument15 pagesExecutive SummaryMini SharmaNo ratings yet
- Lecture 10Document17 pagesLecture 10Carlos Aguilar RodríguezNo ratings yet
- CPS Cable Track ChainDocument1 pageCPS Cable Track ChainVijayakumar Hadron MechNo ratings yet
- Grade 6 EnglishDocument249 pagesGrade 6 Englishgetacheweyob74No ratings yet
- A New Mutuel Kerberos Authentication Protocol For Distributed SystemsDocument10 pagesA New Mutuel Kerberos Authentication Protocol For Distributed SystemsRahul prabhaNo ratings yet
- English 8 Q2M3Document5 pagesEnglish 8 Q2M3Mark Jhoriz VillafuerteNo ratings yet
- Real Estate Review Sample PageDocument15 pagesReal Estate Review Sample PageNway Lay100% (1)
- DbmsDocument2 pagesDbmsbhagy finaviyaNo ratings yet
- Falsafah, Prinsip Dan Isu Dalam Kemahiran Berfikir Aras Tinggi (KBAT) Yang Berkaitan Dengan TIMSS Dan PISA Di MalaysiaDocument81 pagesFalsafah, Prinsip Dan Isu Dalam Kemahiran Berfikir Aras Tinggi (KBAT) Yang Berkaitan Dengan TIMSS Dan PISA Di Malaysiahalimi_foaedNo ratings yet
- Chocolate Chip Banana BreadDocument8 pagesChocolate Chip Banana BreadouruleNo ratings yet
- Fossil Fuels Oil and GasDocument12 pagesFossil Fuels Oil and GasCrystian Kobee EmpeynadoNo ratings yet
- Tipe / Type Vega R New 2008 Nomor Identifikasi Kendaraan / MH34D70028j903504 No. Mesin / Engine No. 4D7.903528 Nomor Plat / License No. KT 2701 KG 60Document7 pagesTipe / Type Vega R New 2008 Nomor Identifikasi Kendaraan / MH34D70028j903504 No. Mesin / Engine No. 4D7.903528 Nomor Plat / License No. KT 2701 KG 60DidinMuhtadinNo ratings yet
- Answers To Questions: MishkinDocument8 pagesAnswers To Questions: Mishkin?ᄋᄉᄋNo ratings yet
- MarineDocument16 pagesMarinehhhhhNo ratings yet
- Pengaruh Pencampuran Semen Terhadap Kuat Geser Tanah Lempung Lampoh KeudeDocument12 pagesPengaruh Pencampuran Semen Terhadap Kuat Geser Tanah Lempung Lampoh KeudeyongkihndrwnNo ratings yet
- SLP Unisa 2014 All CollegesDocument324 pagesSLP Unisa 2014 All CollegesWerner LouwNo ratings yet
- JCNP 2013/2014 SynopsisDocument16 pagesJCNP 2013/2014 SynopsisStephengay64No ratings yet
- Outsiders B1 BookletDocument82 pagesOutsiders B1 BookletKakali MallianNo ratings yet
- P2NP To Amine With NaBH4-CopperDocument281 pagesP2NP To Amine With NaBH4-CopperIo TatNo ratings yet
- Itachi - Bright Light Chapter 4Document21 pagesItachi - Bright Light Chapter 4Koji ChoqueticllaNo ratings yet
- Then Shall Ye Return: Malachi 3:18Document3 pagesThen Shall Ye Return: Malachi 3:18Paul Richard AbejuelaNo ratings yet
- Business Day - Insights - Credit Management - February 2021Document2 pagesBusiness Day - Insights - Credit Management - February 2021SundayTimesZANo ratings yet
- Apply 5S ProceduresDocument8 pagesApply 5S Proceduresdagmabay136No ratings yet
- Sep 15 Final Cpsa LetterDocument19 pagesSep 15 Final Cpsa LetterFatima Berriah CamposNo ratings yet
- The Case For Technology in Music EducationDocument12 pagesThe Case For Technology in Music EducationAndrew T. Garcia93% (15)
- IDOT 2020 Bridge Design Updates - Revised PPC Beam DetailsDocument34 pagesIDOT 2020 Bridge Design Updates - Revised PPC Beam DetailsJoe AndrewsNo ratings yet
- MetalurgiaDocument5 pagesMetalurgiaAndjelkaStankovicNo ratings yet
- Functions of MerchandiserDocument26 pagesFunctions of MerchandiseryuktiNo ratings yet
- Appendix 1 I T L C: 1 Inclining Test and Lightweight CheckDocument5 pagesAppendix 1 I T L C: 1 Inclining Test and Lightweight CheckPaúl ZambranoNo ratings yet