Download as pdf or txt
You might also like
- Agriculture at A Glance: Daya Publishing HouseDocument7 pagesAgriculture at A Glance: Daya Publishing HousePan Smith57% (7)
- ZCS300 ManualDocument24 pagesZCS300 ManualFabricio BorgattaNo ratings yet
- Índice Guild of American Lutherie BooksDocument283 pagesÍndice Guild of American Lutherie BooksDaniel AndradeNo ratings yet
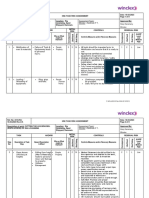
- 2318-RA 18.03.2023-REV 0A Cutting The Leg Bracing - RIG Rig LovansingDocument9 pages2318-RA 18.03.2023-REV 0A Cutting The Leg Bracing - RIG Rig LovansingHafeez AliNo ratings yet
- Natuzza Evolo Mother Natuzza and Her Gifts Given by GodDocument7 pagesNatuzza Evolo Mother Natuzza and Her Gifts Given by GodNurli Girsang100% (1)
- Bone Density - MischDocument16 pagesBone Density - MischMahmood E.100% (1)
- Drone Study PDFDocument54 pagesDrone Study PDFMihaela Azamfirei100% (1)
- El Destino de La Tabla Osea Alrededor Implantes, Despues 12 Meses Carga COIRDocument6 pagesEl Destino de La Tabla Osea Alrededor Implantes, Despues 12 Meses Carga COIRmarioNo ratings yet
- Articulo 13Document6 pagesArticulo 13Daniela NarváezNo ratings yet
- Reposicionamiento DiscalDocument11 pagesReposicionamiento DiscalJuliana ÁlvarezNo ratings yet
- Mobility of The Osteotomy Site Following Le Fort I Osteo Tomy Stabilized by Titanium Plate 0s Teosyn ThesisDocument7 pagesMobility of The Osteotomy Site Following Le Fort I Osteo Tomy Stabilized by Titanium Plate 0s Teosyn Thesisمحمد عبدالرحمنNo ratings yet
- Bilateral Sagittal Split Osteotomy For Correction of Mandibular Prognathism: Long-Term ResultsDocument9 pagesBilateral Sagittal Split Osteotomy For Correction of Mandibular Prognathism: Long-Term ResultsdrescobedocomfNo ratings yet
- Factors Contributing To Relapse in Rigidly Fixed Mandibular SetbacksDocument6 pagesFactors Contributing To Relapse in Rigidly Fixed Mandibular Setbacksabhishekjha0082No ratings yet
- Histological and Histomorphometric Evaluation of Inmediate Implant Placement On A Dog Model With A New Implant Surface TreatmentDocument8 pagesHistological and Histomorphometric Evaluation of Inmediate Implant Placement On A Dog Model With A New Implant Surface TreatmentfranciscosciancaNo ratings yet
- Does Altering The Occlusal Vertical Dimension Produce Temporomandibular Disorders? A Literature ReviewDocument8 pagesDoes Altering The Occlusal Vertical Dimension Produce Temporomandibular Disorders? A Literature ReviewSTEPHANIE JARAMILLONo ratings yet
- OSRM ProximalDocument9 pagesOSRM ProximalÂngelo Rosso LlantadaNo ratings yet
- 1 s2.0 S0022391323002810 MainDocument11 pages1 s2.0 S0022391323002810 MainDANTE DELEGUERYNo ratings yet
- JPM 12 00508 PDFDocument9 pagesJPM 12 00508 PDFMans TvNo ratings yet
- Ortodoncia 2Document9 pagesOrtodoncia 2soisosoisNo ratings yet
- Jossjoralmaxillofacsurg20106812601269 PDFDocument10 pagesJossjoralmaxillofacsurg20106812601269 PDFSaurabh SatheNo ratings yet
- Young KyunDocument6 pagesYoung Kyunodontologia uvNo ratings yet
- Park 2012Document6 pagesPark 2012Yassin SalahNo ratings yet
- Malocclusion As A Common Occurrence in Temporomandibular Joint Arthroscopic Disc Repositioning - Outcomes at 49 Days After Surgery 2Document7 pagesMalocclusion As A Common Occurrence in Temporomandibular Joint Arthroscopic Disc Repositioning - Outcomes at 49 Days After Surgery 2Ario LovellyNo ratings yet
- Liebregts 2019Document9 pagesLiebregts 2019Lorena PaulaNo ratings yet
- Tiempo y FracturaDocument7 pagesTiempo y FracturaPedro TorresNo ratings yet
- A Comparative Study On Complete and ImDocument8 pagesA Comparative Study On Complete and ImAbraham Gomez BautistaNo ratings yet
- Softandhardtissuechangesin Class IIIpatientstreatedbybimaxillarysurgeryDocument10 pagesSoftandhardtissuechangesin Class IIIpatientstreatedbybimaxillarysurgeryFaridah RisnawatiNo ratings yet
- Delir 2013Document7 pagesDelir 2013Karam EidNo ratings yet
- 2002 Bone SPECT Imaging of Patients With Internal Derangement of TMJ Before and After Splint TherapyDocument5 pages2002 Bone SPECT Imaging of Patients With Internal Derangement of TMJ Before and After Splint TherapyNaysha CalleNo ratings yet
- Distraction Vs OGSxDocument13 pagesDistraction Vs OGSxjaslinshalinNo ratings yet
- The Positive Effect of Tenting Screws For Primary Horizontal Guided Bone Regeneration - A Retrospective Study Based On Cone-Beam Computed Tomography Data - Hämmerle 2020Document10 pagesThe Positive Effect of Tenting Screws For Primary Horizontal Guided Bone Regeneration - A Retrospective Study Based On Cone-Beam Computed Tomography Data - Hämmerle 2020LEONARDO ALBERTO CRESPIN ZEPEDANo ratings yet
- Growth Relativity Theory With Cover Page v2Document21 pagesGrowth Relativity Theory With Cover Page v2Shubham khandkeNo ratings yet
- Overcoming Temporomandibular Joint Clicking and PainDocument4 pagesOvercoming Temporomandibular Joint Clicking and PainNatalie SalazarNo ratings yet
- A4 Distaliation of Maxillary Molars With The Bone Supported Pendulum A Clinical Study Ajodo 200793Document5 pagesA4 Distaliation of Maxillary Molars With The Bone Supported Pendulum A Clinical Study Ajodo 200793cesarNo ratings yet
- Admin,+Journal+Manager,+56 AJPCR 20808 O 20171102Document5 pagesAdmin,+Journal+Manager,+56 AJPCR 20808 O 20171102bhushan adhariNo ratings yet
- Articulo 9Document7 pagesArticulo 9Daniela NarváezNo ratings yet
- Park 2012Document9 pagesPark 2012abhishekjha0082No ratings yet
- Growth Relativity Theory PDFDocument20 pagesGrowth Relativity Theory PDFMonojit DuttaNo ratings yet
- Bone Joint J 2013 23-30Document8 pagesBone Joint J 2013 23-30babac88No ratings yet
- Conunterclock WiseDocument5 pagesConunterclock WiseEduardo HernándezNo ratings yet
- 10 1016@j Jcms 2020 09 007Document6 pages10 1016@j Jcms 2020 09 007Sathyla Lander SelomNo ratings yet
- OdontologiaDocument10 pagesOdontologiaDebora Pereira CastroNo ratings yet
- ART - EXP.MAND.7.Postretention Changes in Mandibular CrowdingDocument11 pagesART - EXP.MAND.7.Postretention Changes in Mandibular CrowdingDiana Paola FontechaNo ratings yet
- 1548-1336 (2004) 030 0030 Aocarc 2 0 Co 2Document10 pages1548-1336 (2004) 030 0030 Aocarc 2 0 Co 2waf51No ratings yet
- Eross 2015Document9 pagesEross 2015serahNo ratings yet
- Siqueira Et Al-2020-Clinical Oral Implants ResearchDocument12 pagesSiqueira Et Al-2020-Clinical Oral Implants Researchsergio bernardesNo ratings yet
- Changes in Facial Form Relative To Progressive Atrophy of The Edentulous JawsDocument7 pagesChanges in Facial Form Relative To Progressive Atrophy of The Edentulous JawsshraddhaNo ratings yet
- 1 s2.0 S101051822300255X MainDocument6 pages1 s2.0 S101051822300255X MainAmanda AngelinaNo ratings yet
- 10 1016@j Ajodo 2019 01 021Document8 pages10 1016@j Ajodo 2019 01 021Alejandra NietoNo ratings yet
- Transverse Skeletal Base Adaptations With Bionator Therapy: A Pilot Implant StudyDocument6 pagesTransverse Skeletal Base Adaptations With Bionator Therapy: A Pilot Implant StudyMazhalai SelvaNo ratings yet
- Cefalo Metric ADocument5 pagesCefalo Metric AStephanie CalleNo ratings yet
- Bragger 1992 - Surgical CLDocument7 pagesBragger 1992 - Surgical CLBryan HeeNo ratings yet
- Treatment of Old Unreduced Posterior Dislocation of ElbowDocument4 pagesTreatment of Old Unreduced Posterior Dislocation of Elbowwenny hildaNo ratings yet
- Vertical Dimension Manutencao Da Altura Com Passar Do TempoDocument5 pagesVertical Dimension Manutencao Da Altura Com Passar Do TempoAllyssonNo ratings yet
- Andrade Et Al-2009-Clinical Anatomy PDFDocument7 pagesAndrade Et Al-2009-Clinical Anatomy PDFJakeCrNo ratings yet
- LeFort I Maxillary Advancement 3 Year Stability and Risk Factors For RelapseDocument8 pagesLeFort I Maxillary Advancement 3 Year Stability and Risk Factors For RelapseMargarida Maria LealNo ratings yet
- Maxillary and Mandibular Width Changes Studied Using Metallic ImplantsDocument6 pagesMaxillary and Mandibular Width Changes Studied Using Metallic ImplantsAlla MushkeyNo ratings yet
- Finite Element Method Simulation of Bone Resorption Beneath A Complete DentureDocument4 pagesFinite Element Method Simulation of Bone Resorption Beneath A Complete DentureFiru LgsNo ratings yet
- ARTICULO 5 Occlusal Plane Modification in Clear Aligners Treatment Three Dimensional Retrospective Longitudinal StudyDocument10 pagesARTICULO 5 Occlusal Plane Modification in Clear Aligners Treatment Three Dimensional Retrospective Longitudinal StudyJohanna TorresNo ratings yet
- Palaska 2014Document10 pagesPalaska 2014Marco TeixeiraNo ratings yet
- Mandibular Implat RetainedDocument6 pagesMandibular Implat RetainedMaria Fernanda Samaniego MorochoNo ratings yet
- Degala S.Document8 pagesDegala S.odontologia uvNo ratings yet
- (2008 Weng) Influence of Microgap Location and Configuration On The Periimplant Bone Morphology in Submerged Implants. An Experimental Study in DogsDocument7 pages(2008 Weng) Influence of Microgap Location and Configuration On The Periimplant Bone Morphology in Submerged Implants. An Experimental Study in Dogsyena1010No ratings yet
- Pressure Distribution in Carpometacarpal Joint Due To Step Off in 2014 InjDocument5 pagesPressure Distribution in Carpometacarpal Joint Due To Step Off in 2014 InjHenrique Paranhos FernandesNo ratings yet
- Gao 2021Document8 pagesGao 2021KATERIN TTITO MAMANINo ratings yet
- 2019 Asset Management PlanDocument162 pages2019 Asset Management PlanticoNo ratings yet
- Clarke No Clarke Yes (Clexa)Document7 pagesClarke No Clarke Yes (Clexa)mercedesmgNo ratings yet
- Biological ClasifficationDocument6 pagesBiological Clasifficationchannel of dhyanaNo ratings yet
- Ijct 1 (5) 305-307Document46 pagesIjct 1 (5) 305-307Anonymous v5uipHNo ratings yet
- SupernaturalismDocument9 pagesSupernaturalismBack upNo ratings yet
- Two Stories About Flying (The Black Aeroplane)Document19 pagesTwo Stories About Flying (The Black Aeroplane)Fathima FaseehaNo ratings yet
- RP-091353 Report RAN 45 SevilleDocument155 pagesRP-091353 Report RAN 45 SevilleDellNo ratings yet
- Reis & Helfman 2023 Fishes, Biodiversity ofDocument29 pagesReis & Helfman 2023 Fishes, Biodiversity ofhomonota7330No ratings yet
- Visit To Shivapuri Nagarjun National Park by 8001 GenialDocument4 pagesVisit To Shivapuri Nagarjun National Park by 8001 GenialGenial poudelNo ratings yet
- Ellipseregular 2Document4 pagesEllipseregular 2Nibha PandeyNo ratings yet
- Design of Sensor Less Sliding-Mode BLDC Motor Speed Regulator Using Class of Uncertain Takagi-Sugeno Nonlinear SystemsDocument5 pagesDesign of Sensor Less Sliding-Mode BLDC Motor Speed Regulator Using Class of Uncertain Takagi-Sugeno Nonlinear SystemsijcnesNo ratings yet
- Lumina Homes PDFDocument1 pageLumina Homes PDFDestre Tima-anNo ratings yet
- Pre Commiss. Check List Chilled Water PumpsDocument3 pagesPre Commiss. Check List Chilled Water PumpsARUL SANKARAN100% (1)
- Spohn Performance, Inc.: Part# D94-02-TB-DS - Adjustable Front Track BarDocument5 pagesSpohn Performance, Inc.: Part# D94-02-TB-DS - Adjustable Front Track BarJameson PowersNo ratings yet
- A Dedicated Specialist For Factory Automation: Fanuc Who We AreDocument6 pagesA Dedicated Specialist For Factory Automation: Fanuc Who We AreWazabi MooNo ratings yet
- What Is The Production Process of Inorganic Pigment PowderDocument3 pagesWhat Is The Production Process of Inorganic Pigment Powderkinley dorjeeNo ratings yet
- Daily ReportDocument3 pagesDaily ReportJoseph AbousafiNo ratings yet
- Methods of Approximation and Determination of Human Vulnerability For Offshore Major Accident Hazard AssessmentDocument55 pagesMethods of Approximation and Determination of Human Vulnerability For Offshore Major Accident Hazard AssessmenthazopmanNo ratings yet
- Citric Acid SDS PestellDocument5 pagesCitric Acid SDS PestellTrisNo ratings yet
- P1662/D8.0, March 2016 - IEEE Draft Recommended Practice For Design and Application of Power Electronics in Electrical Power SystemsDocument63 pagesP1662/D8.0, March 2016 - IEEE Draft Recommended Practice For Design and Application of Power Electronics in Electrical Power SystemsHgoglezNo ratings yet
- Changes From Rev AK To Rev AL Skyview Installation GuideDocument608 pagesChanges From Rev AK To Rev AL Skyview Installation GuideF BakımNo ratings yet
- Parad ShivlingDocument2 pagesParad ShivlingsharathVEMNo ratings yet
- If emDocument13 pagesIf emglassw380No ratings yet
- Lecture 3 - Purpose of ArtDocument46 pagesLecture 3 - Purpose of ArtGrace LabayneNo ratings yet