Download as pdf or txt
You might also like
- Glen Johnson - Sciatica SOS EbookDocument84 pagesGlen Johnson - Sciatica SOS EbookRodrigo Lima0% (2)
- Self - Care Deficit Theory of NursingDocument20 pagesSelf - Care Deficit Theory of NursingAudi Kyle Saydoven100% (2)
- Disaster Nursing PowerpointDocument199 pagesDisaster Nursing PowerpointJustine Jake L. Ella100% (2)
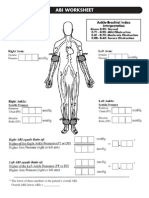
- Abi SheetsDocument2 pagesAbi Sheetszaky soewandi0% (1)
- MCQ Continuum Stroke 2Document10 pagesMCQ Continuum Stroke 2Vita Kusuma RahmawatiNo ratings yet
- Triage SystemDocument39 pagesTriage SystemfitawijamariNo ratings yet
- Chn-Home VisitDocument3 pagesChn-Home VisitjolibeecaldonaNo ratings yet
- L2 Triage PrinciplesDocument38 pagesL2 Triage PrinciplesCrystal CHAN (FABULOUS)No ratings yet
- Critical Incident ReportingDocument44 pagesCritical Incident Reportingsushil@irdNo ratings yet
- Educating Your Staff SlidesDocument12 pagesEducating Your Staff SlidesBrian BoyceNo ratings yet
- Part I: Emergency Department (ED) : SKINNY ReasoningDocument6 pagesPart I: Emergency Department (ED) : SKINNY ReasoningUzumaki KNo ratings yet
- 7 Steps Patient Safety PDFDocument58 pages7 Steps Patient Safety PDFDanissa Fidia PuteriNo ratings yet
- Triage AkhirDocument40 pagesTriage AkhirputuNo ratings yet
- Review of Triage and DocumentationDocument68 pagesReview of Triage and DocumentationVhyta Nounha RespectNo ratings yet
- Surveillance: Fufa Hunduma (MD, MPH in Field EP) SPHMMCDocument72 pagesSurveillance: Fufa Hunduma (MD, MPH in Field EP) SPHMMCbiniam yohannesNo ratings yet
- Chapter 12 NCM103Document22 pagesChapter 12 NCM103CyeonjNo ratings yet
- Nursing ResearchDocument5 pagesNursing Researchprokuno89% (9)
- Servillance and Out BreakDocument79 pagesServillance and Out BreakruthNo ratings yet
- Lesson 3 Scene Assessment and Primary AssessmentDocument28 pagesLesson 3 Scene Assessment and Primary AssessmentReinaldi BoletimiNo ratings yet
- 2013 ED Conference - Triage - Kim FuzzardDocument26 pages2013 ED Conference - Triage - Kim Fuzzardbagus100% (1)
- Pentagon Professional Adjustment, Legal Management, Ethics & Research in NursingDocument19 pagesPentagon Professional Adjustment, Legal Management, Ethics & Research in NursingJen Plazuela100% (1)
- The Work of The National Patient Safety Agency: Joan Russell Safer Practice Lead-Emergency CareDocument43 pagesThe Work of The National Patient Safety Agency: Joan Russell Safer Practice Lead-Emergency CaremuchtarNo ratings yet
- Problem Oriented Approach Bali 2018Document69 pagesProblem Oriented Approach Bali 2018dendikomalaNo ratings yet
- Climate Change and Health 2Document66 pagesClimate Change and Health 2AngellaNo ratings yet
- Outbreak InvestigationDocument55 pagesOutbreak InvestigationSumit KarnNo ratings yet
- The Work of The National Patient Safety Agency: Joan Russell Safer Practice Lead-Emergency CareDocument43 pagesThe Work of The National Patient Safety Agency: Joan Russell Safer Practice Lead-Emergency CareMohammed HammedNo ratings yet
- Digital Notes On Nursing ResearchDocument18 pagesDigital Notes On Nursing ResearchEnna EstrellaNo ratings yet
- Emergency Department Triage System: Ns. Risna Yekti Mumpuni, M. KepDocument33 pagesEmergency Department Triage System: Ns. Risna Yekti Mumpuni, M. KepMaster BrownNo ratings yet
- Assess PDFDocument5 pagesAssess PDFLouis UranoNo ratings yet
- 6disaster Nursing SAS Session 6Document6 pages6disaster Nursing SAS Session 6Beverly Mae Castillo JaymeNo ratings yet
- Gender Identity and Expression: Week 8Document21 pagesGender Identity and Expression: Week 8gonzalezpedro774No ratings yet
- Unit 2: Components of AssessmentDocument16 pagesUnit 2: Components of AssessmentVibhasri GurjalNo ratings yet
- Nursing ProcessDocument3 pagesNursing ProcessErica AbellanosaNo ratings yet
- Week 1Document21 pagesWeek 1Gian Carlo BenitoNo ratings yet
- Nursing ProcessDocument70 pagesNursing Processsarhang talebaniNo ratings yet
- Part 1Document31 pagesPart 1kaleabmarkos06No ratings yet
- Illness Script Formation in Diagnostic Reasoning Within Advanced Practice Nursing EducationDocument28 pagesIllness Script Formation in Diagnostic Reasoning Within Advanced Practice Nursing EducationJOSE ALBERTO KENYO RIOFRIO PALACIOSNo ratings yet
- Study Types Cohort and Case-Control Studies: Charlotte Glümer Bendix CarstensenDocument20 pagesStudy Types Cohort and Case-Control Studies: Charlotte Glümer Bendix Carstensenarun_rana_11No ratings yet
- Outbreak InvestigationDocument35 pagesOutbreak Investigationkedar karki100% (2)
- Golden Gate Colleges - Mrs. Gypsyrose Arojado: Health AssessmentDocument3 pagesGolden Gate Colleges - Mrs. Gypsyrose Arojado: Health AssessmentJaellaNo ratings yet
- Ebm Therapeutics Lecture For MsucomDocument51 pagesEbm Therapeutics Lecture For MsucomKenneth NuñezNo ratings yet
- Case Control StudyDocument41 pagesCase Control Studylinwaiaung500No ratings yet
- Epidemiologic Study Design Case - Control: Dr. Mufuta Tshimanga Professor - Public Health MedicineDocument38 pagesEpidemiologic Study Design Case - Control: Dr. Mufuta Tshimanga Professor - Public Health MedicineZvanakireni Maggie ChikashaNo ratings yet
- Disaster NursingDocument9 pagesDisaster NursingKimberly Louise LopezNo ratings yet
- Health Assessment Topic 1Document54 pagesHealth Assessment Topic 1tmmrsptlnNo ratings yet
- Trainee20doctor20handbook v7 LinkedDocument18 pagesTrainee20doctor20handbook v7 LinkedAshraf MullaNo ratings yet
- Nursing ProcessDocument68 pagesNursing ProcessSareno PJhēaNo ratings yet
- ER FINAL NOTES - CompressedDocument68 pagesER FINAL NOTES - CompressedRosaree Mae PantojaNo ratings yet
- Outbreak Investigation: Best Practice/Methods Practical Reference PointsDocument48 pagesOutbreak Investigation: Best Practice/Methods Practical Reference Pointsorangegirl002No ratings yet
- Nursing Process: - Assess - Determine Nsg. Dx. - Plan - Implement - EvaluateDocument31 pagesNursing Process: - Assess - Determine Nsg. Dx. - Plan - Implement - EvaluategireeshsachinNo ratings yet
- Emergency Care in NursingDocument32 pagesEmergency Care in NursingPauline Añes100% (1)
- Epi - Study DesignsDocument60 pagesEpi - Study DesignsTofik Mohammad MuseNo ratings yet
- Chapter 08 Patient AssessmentDocument129 pagesChapter 08 Patient AssessmentNephNo ratings yet
- Ha PrelimDocument50 pagesHa Prelimlcpanaligan4175antNo ratings yet
- SISS - Diagnostic Adjuncts During Primary SurveyDocument7 pagesSISS - Diagnostic Adjuncts During Primary SurveyPrincy100% (1)
- Study Design EpidemiologyDocument35 pagesStudy Design Epidemiologyumar evans kizitoNo ratings yet
- Nursing Process 1sepDocument50 pagesNursing Process 1sepM ANo ratings yet
- Proses & Tahapan KeperawatanDocument35 pagesProses & Tahapan KeperawatanKasi KeperawatanNo ratings yet
- Communication and Optimal Resolution (CANDOR) : Grand Rounds PresentationDocument45 pagesCommunication and Optimal Resolution (CANDOR) : Grand Rounds PresentationJoel John Dela MercedNo ratings yet
- Emergency Nursing2Document34 pagesEmergency Nursing2Nina Oaip100% (1)
- Lesson 1 Beginning The AssessmentDocument36 pagesLesson 1 Beginning The AssessmentAlex WindsorNo ratings yet
- Mutual Prodrug Concept Fundamentals and ApplicationsDocument9 pagesMutual Prodrug Concept Fundamentals and ApplicationsUmaima faizNo ratings yet
- MSDS Benzene PDFDocument6 pagesMSDS Benzene PDFPiyu SyahputraNo ratings yet
- Skydrol 500b4 Hydraulic Fluid GallonDocument13 pagesSkydrol 500b4 Hydraulic Fluid Gallonouss18No ratings yet
- 3 Hidden Secret Eye GazeDocument9 pages3 Hidden Secret Eye GazeekoNo ratings yet
- Hyperlipidemia Self ManagementDocument27 pagesHyperlipidemia Self ManagementElizabeth HoNo ratings yet
- Components of Physical FitnessDocument42 pagesComponents of Physical FitnessAlthea Kae Gaon Tangco100% (3)
- Pub1566 WebDocument124 pagesPub1566 WebRadoi Sandina RodicaNo ratings yet
- PharmaDocument10 pagesPharmaYeng MangilitNo ratings yet
- Ami Jariwala - Regulatory Affairs PDFDocument3 pagesAmi Jariwala - Regulatory Affairs PDFAmi JariwalaNo ratings yet
- Diagnostic Approach To Chronic Constipation in Adults: Namirah Jamshed, MD Zone-En Lee, MD and Kevin W. Olden, MDDocument8 pagesDiagnostic Approach To Chronic Constipation in Adults: Namirah Jamshed, MD Zone-En Lee, MD and Kevin W. Olden, MDwilson koresNo ratings yet
- Jet Lag PDFDocument8 pagesJet Lag PDFIan FitzpatrickNo ratings yet
- MM Ous Microscan Eucast Gram Neg Ds 11 2013-01349657Document2 pagesMM Ous Microscan Eucast Gram Neg Ds 11 2013-01349657sazunaxNo ratings yet
- G1-4. Case Study 2 Ans - MI LV Failure + SepsisDocument1 pageG1-4. Case Study 2 Ans - MI LV Failure + Sepsisj.jk.jk.17No ratings yet
- ICDSDocument21 pagesICDSKrishnaveni MurugeshNo ratings yet
- Introduction 2 PDFDocument58 pagesIntroduction 2 PDFGaming ZoneNo ratings yet
- PDF Ultrasound For Interventional Pain Management An Illustrated Procedural Guide Philip Peng Ebook Full ChapterDocument53 pagesPDF Ultrasound For Interventional Pain Management An Illustrated Procedural Guide Philip Peng Ebook Full Chapteralexander.mau386100% (2)
- Your Touch Is My HealingDocument79 pagesYour Touch Is My HealingPipi PopoNo ratings yet
- Faculty List SGMCDocument20 pagesFaculty List SGMCmeymeysenpaiNo ratings yet
- Fluoride Toxicity and DefluoridationDocument91 pagesFluoride Toxicity and DefluoridationAbhijeet Kadu50% (2)
- National Health Act 61 of 2003: (English Text Signed by The President)Document33 pagesNational Health Act 61 of 2003: (English Text Signed by The President)Bhekinkosi Nifty NcubeNo ratings yet
- RCT+Appraisal+sheets. TherapyDocument2 pagesRCT+Appraisal+sheets. Therapydian_c87No ratings yet
- Apa Paper On Nursing Body MechanicsDocument6 pagesApa Paper On Nursing Body Mechanicsapi-260726761No ratings yet
- Relevance and Treatment of Coccidiosis in Domestic Pigeons (Columba Livia Forma Domestica) With Particular Emphasis On ToltrazurilDocument6 pagesRelevance and Treatment of Coccidiosis in Domestic Pigeons (Columba Livia Forma Domestica) With Particular Emphasis On ToltrazurilAnonymous tBJwSUSjNo ratings yet
- Sts - Chapter - 1 Lesson 1Document34 pagesSts - Chapter - 1 Lesson 1Rhandel John ResiduoNo ratings yet
- Approach To The Dialysis Patient Summary - Kate Wyburn FinalDocument3 pagesApproach To The Dialysis Patient Summary - Kate Wyburn Finaltnsource100% (1)
- Krok 2 2002-2003 HygieneDocument8 pagesKrok 2 2002-2003 HygieneAli ZeeshanNo ratings yet
- Arjuna in AyurvedaDocument6 pagesArjuna in AyurvedaugoNo ratings yet