
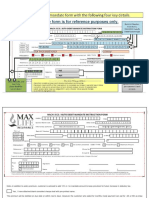
Alternate Mode Mandate Form - 21012023
Alternate Mode Mandate Form - 21012023
You might also like
- NACH FormDocument1 pageNACH FormPrem Singh Mehta75% (4)
- Auto-Debit Arrangement Enrollment FormDocument1 pageAuto-Debit Arrangement Enrollment FormDiana Sia VillamorNo ratings yet
- FWD Life Insurance Corp.: Expresslink Automatic Debit ArrangementDocument1 pageFWD Life Insurance Corp.: Expresslink Automatic Debit ArrangementMatteo Messina DenaroNo ratings yet
- Macasiano v. Diokno (PubCorp Case Digest4)Document2 pagesMacasiano v. Diokno (PubCorp Case Digest4)Robert Lavina100% (1)
- Renewal Ecs Latest Form - 8.9.2017Document1 pageRenewal Ecs Latest Form - 8.9.2017Priya SelvarajNo ratings yet
- FOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherDocument2 pagesFOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherAnithaNo ratings yet
- ABSLIC - NACH, ECS, Auto Direct Debit FormDocument2 pagesABSLIC - NACH, ECS, Auto Direct Debit FormBHARAT PRAKASH MAHANT0% (2)
- FOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherDocument2 pagesFOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherVIkashNo ratings yet
- Sbi New Ecs FormDocument1 pageSbi New Ecs FormzampakNo ratings yet
- Customer Declaration FormDocument2 pagesCustomer Declaration FormAbhinanth Mj90% (10)
- Security Bank ADA Enrollment FormDocument1 pageSecurity Bank ADA Enrollment FormNoknik OllirecNo ratings yet
- Auto Debit Instruction For Nach/Dd: Cc/Branchops/Mandate Form/002Document2 pagesAuto Debit Instruction For Nach/Dd: Cc/Branchops/Mandate Form/002Dhruv SekhriNo ratings yet
- Ada Form DownloadDocument1 pageAda Form DownloadDona DolorzoNo ratings yet
- Auto Debit Arrangement - 20190804 - 020707 PDFDocument4 pagesAuto Debit Arrangement - 20190804 - 020707 PDFKim Josashiwa BergulaNo ratings yet
- NACH ModifiedDocument1 pageNACH ModifiederbgawdweNo ratings yet
- Es Direct Debit MandateDocument4 pagesEs Direct Debit Mandatecatherinecastillo914No ratings yet
- Customer Acknowledgment Form: Applicant InformationDocument2 pagesCustomer Acknowledgment Form: Applicant InformationKamlesh SonareNo ratings yet
- Auto Debit Arrangement - 20201019 - 095034 PDFDocument3 pagesAuto Debit Arrangement - 20201019 - 095034 PDFRobert Adrian De RuedaNo ratings yet
- FIP Mandate FormDocument2 pagesFIP Mandate FormRajiv KumarNo ratings yet
- Annexure - To - Connect - Life - Proposals v3.0 PDFDocument1 pageAnnexure - To - Connect - Life - Proposals v3.0 PDFmahboob aliNo ratings yet
- Loan Restructuring App FormDocument3 pagesLoan Restructuring App FormLilibeth Allosada LapathaNo ratings yet
- BPI Automatic Debit ArrangementDocument2 pagesBPI Automatic Debit ArrangementJackophiliNo ratings yet
- Mandate Form For Electronic Transfer of Claim/Refund/Commission/Other PaymentsDocument2 pagesMandate Form For Electronic Transfer of Claim/Refund/Commission/Other Paymentsjoshua francisNo ratings yet
- NACH V1.3 - 29122017 - For Preferred DateDocument2 pagesNACH V1.3 - 29122017 - For Preferred DateMadhumita DuttaNo ratings yet
- Annexure To Connect Life Proposal v6.0Document1 pageAnnexure To Connect Life Proposal v6.0Aryan AgarwalNo ratings yet
- NEFT Mandate Form RevisedDocument2 pagesNEFT Mandate Form Revisedaadi06gameNo ratings yet
- Bank Authorization (BA) FormDocument4 pagesBank Authorization (BA) FormAilec FinancesNo ratings yet
- revalidation-of-redemption-or-dividend-warrant-(with-change-of-bank-details)Document2 pagesrevalidation-of-redemption-or-dividend-warrant-(with-change-of-bank-details)rousanmirzaNo ratings yet
- Ada Form DownloadDocument1 pageAda Form DownloadVergie PovadoraNo ratings yet
- NEFT Mandate FormDocument2 pagesNEFT Mandate FormSupriya KandukuriNo ratings yet
- Standing Instruction Form Through IndusInd Bank Account-2Document1 pageStanding Instruction Form Through IndusInd Bank Account-2SonuNo ratings yet
- Pay-Out Request Form Ver1.1Document2 pagesPay-Out Request Form Ver1.1Mahendra AsawaleNo ratings yet
- Forms Payout Others Web 23 AprilDocument2 pagesForms Payout Others Web 23 AprilYo PaisaNo ratings yet
- Personal Advantage Loan Form 1Document4 pagesPersonal Advantage Loan Form 1JOSEPHINE MAGBUTAYNo ratings yet
- Mandate Form For Auto Debit HDFC ElifeDocument2 pagesMandate Form For Auto Debit HDFC ElifeRaj Herg100% (1)
- New Personal Salary Loan Application: (Last Name) (First Name) (Middle Initial) (Suffix)Document2 pagesNew Personal Salary Loan Application: (Last Name) (First Name) (Middle Initial) (Suffix)En-en FrioNo ratings yet
- EcsdebitDocument1 pageEcsdebitvalakrishnanraviNo ratings yet
- Final Application Form - Restructuring 2.0 - RevisedDocument5 pagesFinal Application Form - Restructuring 2.0 - RevisedShabin ShabiNo ratings yet
- Customer Declaration and ECS FormDocument1 pageCustomer Declaration and ECS FormJanakiRamanNo ratings yet
- Nach ECS Direct Debit Mandate Instruction FormDocument2 pagesNach ECS Direct Debit Mandate Instruction Formsiva nunnaNo ratings yet
- Primary Account Holder Joint Account Holder 1 Joint Account Holder 2Document1 pagePrimary Account Holder Joint Account Holder 1 Joint Account Holder 2Varun NagpalNo ratings yet
- Policy Surrender FormDocument2 pagesPolicy Surrender Formaife.ocubilloNo ratings yet
- Ada Enrollment FormDocument2 pagesAda Enrollment FormLira del RosarioNo ratings yet
- Ecs Nach Si Mandate FormDocument2 pagesEcs Nach Si Mandate FormSachinNo ratings yet
- Bosa Loan FormDocument4 pagesBosa Loan FormIsaac OkotNo ratings yet
- Maturity Form: Policy InformationDocument2 pagesMaturity Form: Policy Informationroodra singh ranawatNo ratings yet
- BPI Autodebit Arrangement FormDocument1 pageBPI Autodebit Arrangement FormKane Arvin ChingNo ratings yet
- CDF For Ecs Direct Debit Form BANCA With NO Option Ver 5.0.2 LatestDocument1 pageCDF For Ecs Direct Debit Form BANCA With NO Option Ver 5.0.2 LatestRaju kumar kushwahaNo ratings yet
- Credit Cash Line FormDocument2 pagesCredit Cash Line FormTommy Dela CruzNo ratings yet
- New ACA Direct Credit Facility Form Rev4 - FinalDocument1 pageNew ACA Direct Credit Facility Form Rev4 - FinalRomeo G TibubosNo ratings yet
- Mid PioneerDocument1 pageMid PioneerVishnu VNo ratings yet
- ECS Direct Debit Mandate FormDocument3 pagesECS Direct Debit Mandate FormManish KumarNo ratings yet
- Helpful Tips For Quick Activation:: Electronic Clearing Service (Debit) Clearing / Direct DebitDocument1 pageHelpful Tips For Quick Activation:: Electronic Clearing Service (Debit) Clearing / Direct DebitArka MitraNo ratings yet
- MP CTA Instruction Form - 07222021Document2 pagesMP CTA Instruction Form - 07222021Jasmine NgoNo ratings yet
- New Agency Salary Loan FormDocument3 pagesNew Agency Salary Loan FormTheo Mastix VlogNo ratings yet
- Surrender FormDocument2 pagesSurrender FormpghoshNo ratings yet
- Policy Service Request FormDocument3 pagesPolicy Service Request FormAaru RizwanNo ratings yet
- New Salary Apds Dep-Ed Loan Application: (Last Name) (First Name) (Middle Initial) (Suffix)Document6 pagesNew Salary Apds Dep-Ed Loan Application: (Last Name) (First Name) (Middle Initial) (Suffix)En-en FrioNo ratings yet
- Agent Banking Uganda Handbook: A simple guide to starting and running a profitable agent banking business in UgandaFrom EverandAgent Banking Uganda Handbook: A simple guide to starting and running a profitable agent banking business in UgandaNo ratings yet
- Credit Secrets: Learn the concepts of Credit Scores, How to Boost them and Take Advantages from Your Credit CardsFrom EverandCredit Secrets: Learn the concepts of Credit Scores, How to Boost them and Take Advantages from Your Credit CardsNo ratings yet
- LM DeclarationDocument1 pageLM Declarationsuccessinvestment2005No ratings yet
- Thiruvannamalai Emp 2023 24 1Document11 pagesThiruvannamalai Emp 2023 24 1successinvestment2005No ratings yet
- Undertaken FormDocument1 pageUndertaken Formsuccessinvestment2005No ratings yet
- Batch List of MBBS Pdy & Karaikal VIII Semester Students - March To Aug 2021 - 0Document10 pagesBatch List of MBBS Pdy & Karaikal VIII Semester Students - March To Aug 2021 - 0successinvestment2005No ratings yet
- TN Neet Ug 2020 Samples 2Document10 pagesTN Neet Ug 2020 Samples 2successinvestment2005No ratings yet
- Prestige Induction PurchaseDocument1 pagePrestige Induction Purchasesuccessinvestment2005No ratings yet
- Account Opening Form SbiDocument8 pagesAccount Opening Form Sbisuccessinvestment2005No ratings yet
- SKM C45822071313041Document1 pageSKM C45822071313041successinvestment2005No ratings yet
- Kim Booklet 1 Aug 23Document524 pagesKim Booklet 1 Aug 23successinvestment2005No ratings yet
- Dataxlsx 5 PDF FreeDocument1,074 pagesDataxlsx 5 PDF Freesuccessinvestment2005No ratings yet
- ACE Memebers ListDocument80 pagesACE Memebers Listsuccessinvestment2005No ratings yet
- HDFC Large and Mid Cap Fund Regular PlanDocument1 pageHDFC Large and Mid Cap Fund Regular Plansuccessinvestment2005No ratings yet
- Request For Change in Policy Details Form EnglishDocument3 pagesRequest For Change in Policy Details Form Englishsuccessinvestment2005No ratings yet
- SBI Life ULIP News Letter January 2024Document35 pagesSBI Life ULIP News Letter January 2024successinvestment2005No ratings yet
- Succession Midterms Magic Notes PDFDocument45 pagesSuccession Midterms Magic Notes PDFAdrian CanlasNo ratings yet
- Rubrico v. Macapagal-Arroyo DigestDocument3 pagesRubrico v. Macapagal-Arroyo Digestjadeanna2250% (2)
- Fra 2014 Vaw Survey Main Results Apr14 - en PDFDocument200 pagesFra 2014 Vaw Survey Main Results Apr14 - en PDFmarpiwebNo ratings yet
- United States v. Hahn, 1st Cir. (1994)Document30 pagesUnited States v. Hahn, 1st Cir. (1994)Scribd Government DocsNo ratings yet
- WEAC BylawsDocument33 pagesWEAC BylawsdespaNo ratings yet
- Condo Suite Club TravelDocument1 pageCondo Suite Club TravelR.A. GregorioNo ratings yet
- Arizona v. California, 298 U.S. 558 (1936)Document11 pagesArizona v. California, 298 U.S. 558 (1936)Scribd Government DocsNo ratings yet
- ABC Contract TemplateDocument9 pagesABC Contract TemplateTMNo ratings yet
- United States v. Kalen Amanda Kennedy, 11th Cir. (2015)Document5 pagesUnited States v. Kalen Amanda Kennedy, 11th Cir. (2015)Scribd Government DocsNo ratings yet
- Assignment Law and Media (Antariksh Singh Jamwal)Document7 pagesAssignment Law and Media (Antariksh Singh Jamwal)Antariksh Singh JamwalNo ratings yet
- G.R. No. 107207Document7 pagesG.R. No. 107207KidMonkey2299No ratings yet
- A Quick Glance at The Law of Division of Matrimonial Assets in A DivorceDocument9 pagesA Quick Glance at The Law of Division of Matrimonial Assets in A DivorceDave YangNo ratings yet
- Probation and Parole in PakDocument19 pagesProbation and Parole in PakAqib TayyabNo ratings yet
- Principles and Theories of Business ManagementDocument9 pagesPrinciples and Theories of Business Managementsteven condaNo ratings yet
- Constitution of Safe Haven For Orphans Organization (I) Preamble PreambleDocument11 pagesConstitution of Safe Haven For Orphans Organization (I) Preamble PreambleSydney KafwankaNo ratings yet
- Private International Law-1Document14 pagesPrivate International Law-1Jyothsna DasNo ratings yet
- United States District Court, S.D. New York. TOP RANK, INC., Plaintiff, v. ALLERTON LOUNGE, INC. and Angel Cortes, D/b/a Bottom Line, Et Al., Defendants.Document5 pagesUnited States District Court, S.D. New York. TOP RANK, INC., Plaintiff, v. ALLERTON LOUNGE, INC. and Angel Cortes, D/b/a Bottom Line, Et Al., Defendants.JNomicsNo ratings yet
- Corruption and Central Vigilance Commission: Made By: David Cyril Babu B.A. LLB (Honours) Viii Semester Roll No. 18Document162 pagesCorruption and Central Vigilance Commission: Made By: David Cyril Babu B.A. LLB (Honours) Viii Semester Roll No. 18T M Santhosh KumarNo ratings yet
- Pan Card Application FormDocument2 pagesPan Card Application FormKaran AggarwalNo ratings yet
- Fundamentals of Criminal Investigation Part 1Document3 pagesFundamentals of Criminal Investigation Part 1johnpaulacosta0% (1)
- White PlainsDocument12 pagesWhite PlainsstevensonaguinaldoNo ratings yet
- Breach of Fiduciary Duty CitesDocument24 pagesBreach of Fiduciary Duty CitesTruthsPressNo ratings yet
- Deadly Maxims of Law To Agents of The CrownDocument10 pagesDeadly Maxims of Law To Agents of The Crownsugar marmelateNo ratings yet
- Targeted Justice - 2nd Amended Complaint - Case No. 6:23-cv-00003 USDC Southern District of Texas Victoria DivisionDocument125 pagesTargeted Justice - 2nd Amended Complaint - Case No. 6:23-cv-00003 USDC Southern District of Texas Victoria DivisionHip-hop LegalNo ratings yet
- Opo - Letter Karanam ManasaDocument5 pagesOpo - Letter Karanam Manasananjundavardhan5No ratings yet
- 52 - Puncia V Toyota Shaw - G.R. No. 214399Document3 pages52 - Puncia V Toyota Shaw - G.R. No. 214399DAblue ReyNo ratings yet
- Consideration Revision Sheet McKendrickDocument18 pagesConsideration Revision Sheet McKendrickDaniella DanjumaNo ratings yet
- Himachal Pradesh University Gyan Path, Summer Hill, Shimla - 171 005 (For Private and Re-Appear Candidates)Document3 pagesHimachal Pradesh University Gyan Path, Summer Hill, Shimla - 171 005 (For Private and Re-Appear Candidates)Sunny Music Productions100% (1)
- Belisario Vs IacDocument2 pagesBelisario Vs IacArvin Guevarra100% (1)





































































































Download as pdf or txt
You might also like
- NACH FormDocument1 pageNACH FormPrem Singh Mehta75% (4)
- Auto-Debit Arrangement Enrollment FormDocument1 pageAuto-Debit Arrangement Enrollment FormDiana Sia VillamorNo ratings yet
- FWD Life Insurance Corp.: Expresslink Automatic Debit ArrangementDocument1 pageFWD Life Insurance Corp.: Expresslink Automatic Debit ArrangementMatteo Messina DenaroNo ratings yet
- Macasiano v. Diokno (PubCorp Case Digest4)Document2 pagesMacasiano v. Diokno (PubCorp Case Digest4)Robert Lavina100% (1)
- Renewal Ecs Latest Form - 8.9.2017Document1 pageRenewal Ecs Latest Form - 8.9.2017Priya SelvarajNo ratings yet
- FOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherDocument2 pagesFOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherAnithaNo ratings yet
- ABSLIC - NACH, ECS, Auto Direct Debit FormDocument2 pagesABSLIC - NACH, ECS, Auto Direct Debit FormBHARAT PRAKASH MAHANT0% (2)
- FOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherDocument2 pagesFOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherVIkashNo ratings yet
- Sbi New Ecs FormDocument1 pageSbi New Ecs FormzampakNo ratings yet
- Customer Declaration FormDocument2 pagesCustomer Declaration FormAbhinanth Mj90% (10)
- Security Bank ADA Enrollment FormDocument1 pageSecurity Bank ADA Enrollment FormNoknik OllirecNo ratings yet
- Auto Debit Instruction For Nach/Dd: Cc/Branchops/Mandate Form/002Document2 pagesAuto Debit Instruction For Nach/Dd: Cc/Branchops/Mandate Form/002Dhruv SekhriNo ratings yet
- Ada Form DownloadDocument1 pageAda Form DownloadDona DolorzoNo ratings yet
- Auto Debit Arrangement - 20190804 - 020707 PDFDocument4 pagesAuto Debit Arrangement - 20190804 - 020707 PDFKim Josashiwa BergulaNo ratings yet
- NACH ModifiedDocument1 pageNACH ModifiederbgawdweNo ratings yet
- Es Direct Debit MandateDocument4 pagesEs Direct Debit Mandatecatherinecastillo914No ratings yet
- Customer Acknowledgment Form: Applicant InformationDocument2 pagesCustomer Acknowledgment Form: Applicant InformationKamlesh SonareNo ratings yet
- Auto Debit Arrangement - 20201019 - 095034 PDFDocument3 pagesAuto Debit Arrangement - 20201019 - 095034 PDFRobert Adrian De RuedaNo ratings yet
- FIP Mandate FormDocument2 pagesFIP Mandate FormRajiv KumarNo ratings yet
- Annexure - To - Connect - Life - Proposals v3.0 PDFDocument1 pageAnnexure - To - Connect - Life - Proposals v3.0 PDFmahboob aliNo ratings yet
- Loan Restructuring App FormDocument3 pagesLoan Restructuring App FormLilibeth Allosada LapathaNo ratings yet
- BPI Automatic Debit ArrangementDocument2 pagesBPI Automatic Debit ArrangementJackophiliNo ratings yet
- Mandate Form For Electronic Transfer of Claim/Refund/Commission/Other PaymentsDocument2 pagesMandate Form For Electronic Transfer of Claim/Refund/Commission/Other Paymentsjoshua francisNo ratings yet
- NACH V1.3 - 29122017 - For Preferred DateDocument2 pagesNACH V1.3 - 29122017 - For Preferred DateMadhumita DuttaNo ratings yet
- Annexure To Connect Life Proposal v6.0Document1 pageAnnexure To Connect Life Proposal v6.0Aryan AgarwalNo ratings yet
- NEFT Mandate Form RevisedDocument2 pagesNEFT Mandate Form Revisedaadi06gameNo ratings yet
- Bank Authorization (BA) FormDocument4 pagesBank Authorization (BA) FormAilec FinancesNo ratings yet
- revalidation-of-redemption-or-dividend-warrant-(with-change-of-bank-details)Document2 pagesrevalidation-of-redemption-or-dividend-warrant-(with-change-of-bank-details)rousanmirzaNo ratings yet
- Ada Form DownloadDocument1 pageAda Form DownloadVergie PovadoraNo ratings yet
- NEFT Mandate FormDocument2 pagesNEFT Mandate FormSupriya KandukuriNo ratings yet
- Standing Instruction Form Through IndusInd Bank Account-2Document1 pageStanding Instruction Form Through IndusInd Bank Account-2SonuNo ratings yet
- Pay-Out Request Form Ver1.1Document2 pagesPay-Out Request Form Ver1.1Mahendra AsawaleNo ratings yet
- Forms Payout Others Web 23 AprilDocument2 pagesForms Payout Others Web 23 AprilYo PaisaNo ratings yet
- Personal Advantage Loan Form 1Document4 pagesPersonal Advantage Loan Form 1JOSEPHINE MAGBUTAYNo ratings yet
- Mandate Form For Auto Debit HDFC ElifeDocument2 pagesMandate Form For Auto Debit HDFC ElifeRaj Herg100% (1)
- New Personal Salary Loan Application: (Last Name) (First Name) (Middle Initial) (Suffix)Document2 pagesNew Personal Salary Loan Application: (Last Name) (First Name) (Middle Initial) (Suffix)En-en FrioNo ratings yet
- EcsdebitDocument1 pageEcsdebitvalakrishnanraviNo ratings yet
- Final Application Form - Restructuring 2.0 - RevisedDocument5 pagesFinal Application Form - Restructuring 2.0 - RevisedShabin ShabiNo ratings yet
- Customer Declaration and ECS FormDocument1 pageCustomer Declaration and ECS FormJanakiRamanNo ratings yet
- Nach ECS Direct Debit Mandate Instruction FormDocument2 pagesNach ECS Direct Debit Mandate Instruction Formsiva nunnaNo ratings yet
- Primary Account Holder Joint Account Holder 1 Joint Account Holder 2Document1 pagePrimary Account Holder Joint Account Holder 1 Joint Account Holder 2Varun NagpalNo ratings yet
- Policy Surrender FormDocument2 pagesPolicy Surrender Formaife.ocubilloNo ratings yet
- Ada Enrollment FormDocument2 pagesAda Enrollment FormLira del RosarioNo ratings yet
- Ecs Nach Si Mandate FormDocument2 pagesEcs Nach Si Mandate FormSachinNo ratings yet
- Bosa Loan FormDocument4 pagesBosa Loan FormIsaac OkotNo ratings yet
- Maturity Form: Policy InformationDocument2 pagesMaturity Form: Policy Informationroodra singh ranawatNo ratings yet
- BPI Autodebit Arrangement FormDocument1 pageBPI Autodebit Arrangement FormKane Arvin ChingNo ratings yet
- CDF For Ecs Direct Debit Form BANCA With NO Option Ver 5.0.2 LatestDocument1 pageCDF For Ecs Direct Debit Form BANCA With NO Option Ver 5.0.2 LatestRaju kumar kushwahaNo ratings yet
- Credit Cash Line FormDocument2 pagesCredit Cash Line FormTommy Dela CruzNo ratings yet
- New ACA Direct Credit Facility Form Rev4 - FinalDocument1 pageNew ACA Direct Credit Facility Form Rev4 - FinalRomeo G TibubosNo ratings yet
- Mid PioneerDocument1 pageMid PioneerVishnu VNo ratings yet
- ECS Direct Debit Mandate FormDocument3 pagesECS Direct Debit Mandate FormManish KumarNo ratings yet
- Helpful Tips For Quick Activation:: Electronic Clearing Service (Debit) Clearing / Direct DebitDocument1 pageHelpful Tips For Quick Activation:: Electronic Clearing Service (Debit) Clearing / Direct DebitArka MitraNo ratings yet
- MP CTA Instruction Form - 07222021Document2 pagesMP CTA Instruction Form - 07222021Jasmine NgoNo ratings yet
- New Agency Salary Loan FormDocument3 pagesNew Agency Salary Loan FormTheo Mastix VlogNo ratings yet
- Surrender FormDocument2 pagesSurrender FormpghoshNo ratings yet
- Policy Service Request FormDocument3 pagesPolicy Service Request FormAaru RizwanNo ratings yet
- New Salary Apds Dep-Ed Loan Application: (Last Name) (First Name) (Middle Initial) (Suffix)Document6 pagesNew Salary Apds Dep-Ed Loan Application: (Last Name) (First Name) (Middle Initial) (Suffix)En-en FrioNo ratings yet
- Agent Banking Uganda Handbook: A simple guide to starting and running a profitable agent banking business in UgandaFrom EverandAgent Banking Uganda Handbook: A simple guide to starting and running a profitable agent banking business in UgandaNo ratings yet
- Credit Secrets: Learn the concepts of Credit Scores, How to Boost them and Take Advantages from Your Credit CardsFrom EverandCredit Secrets: Learn the concepts of Credit Scores, How to Boost them and Take Advantages from Your Credit CardsNo ratings yet
- LM DeclarationDocument1 pageLM Declarationsuccessinvestment2005No ratings yet
- Thiruvannamalai Emp 2023 24 1Document11 pagesThiruvannamalai Emp 2023 24 1successinvestment2005No ratings yet
- Undertaken FormDocument1 pageUndertaken Formsuccessinvestment2005No ratings yet
- Batch List of MBBS Pdy & Karaikal VIII Semester Students - March To Aug 2021 - 0Document10 pagesBatch List of MBBS Pdy & Karaikal VIII Semester Students - March To Aug 2021 - 0successinvestment2005No ratings yet
- TN Neet Ug 2020 Samples 2Document10 pagesTN Neet Ug 2020 Samples 2successinvestment2005No ratings yet
- Prestige Induction PurchaseDocument1 pagePrestige Induction Purchasesuccessinvestment2005No ratings yet
- Account Opening Form SbiDocument8 pagesAccount Opening Form Sbisuccessinvestment2005No ratings yet
- SKM C45822071313041Document1 pageSKM C45822071313041successinvestment2005No ratings yet
- Kim Booklet 1 Aug 23Document524 pagesKim Booklet 1 Aug 23successinvestment2005No ratings yet
- Dataxlsx 5 PDF FreeDocument1,074 pagesDataxlsx 5 PDF Freesuccessinvestment2005No ratings yet
- ACE Memebers ListDocument80 pagesACE Memebers Listsuccessinvestment2005No ratings yet
- HDFC Large and Mid Cap Fund Regular PlanDocument1 pageHDFC Large and Mid Cap Fund Regular Plansuccessinvestment2005No ratings yet
- Request For Change in Policy Details Form EnglishDocument3 pagesRequest For Change in Policy Details Form Englishsuccessinvestment2005No ratings yet
- SBI Life ULIP News Letter January 2024Document35 pagesSBI Life ULIP News Letter January 2024successinvestment2005No ratings yet
- Succession Midterms Magic Notes PDFDocument45 pagesSuccession Midterms Magic Notes PDFAdrian CanlasNo ratings yet
- Rubrico v. Macapagal-Arroyo DigestDocument3 pagesRubrico v. Macapagal-Arroyo Digestjadeanna2250% (2)
- Fra 2014 Vaw Survey Main Results Apr14 - en PDFDocument200 pagesFra 2014 Vaw Survey Main Results Apr14 - en PDFmarpiwebNo ratings yet
- United States v. Hahn, 1st Cir. (1994)Document30 pagesUnited States v. Hahn, 1st Cir. (1994)Scribd Government DocsNo ratings yet
- WEAC BylawsDocument33 pagesWEAC BylawsdespaNo ratings yet
- Condo Suite Club TravelDocument1 pageCondo Suite Club TravelR.A. GregorioNo ratings yet
- Arizona v. California, 298 U.S. 558 (1936)Document11 pagesArizona v. California, 298 U.S. 558 (1936)Scribd Government DocsNo ratings yet
- ABC Contract TemplateDocument9 pagesABC Contract TemplateTMNo ratings yet
- United States v. Kalen Amanda Kennedy, 11th Cir. (2015)Document5 pagesUnited States v. Kalen Amanda Kennedy, 11th Cir. (2015)Scribd Government DocsNo ratings yet
- Assignment Law and Media (Antariksh Singh Jamwal)Document7 pagesAssignment Law and Media (Antariksh Singh Jamwal)Antariksh Singh JamwalNo ratings yet
- G.R. No. 107207Document7 pagesG.R. No. 107207KidMonkey2299No ratings yet
- A Quick Glance at The Law of Division of Matrimonial Assets in A DivorceDocument9 pagesA Quick Glance at The Law of Division of Matrimonial Assets in A DivorceDave YangNo ratings yet
- Probation and Parole in PakDocument19 pagesProbation and Parole in PakAqib TayyabNo ratings yet
- Principles and Theories of Business ManagementDocument9 pagesPrinciples and Theories of Business Managementsteven condaNo ratings yet
- Constitution of Safe Haven For Orphans Organization (I) Preamble PreambleDocument11 pagesConstitution of Safe Haven For Orphans Organization (I) Preamble PreambleSydney KafwankaNo ratings yet
- Private International Law-1Document14 pagesPrivate International Law-1Jyothsna DasNo ratings yet
- United States District Court, S.D. New York. TOP RANK, INC., Plaintiff, v. ALLERTON LOUNGE, INC. and Angel Cortes, D/b/a Bottom Line, Et Al., Defendants.Document5 pagesUnited States District Court, S.D. New York. TOP RANK, INC., Plaintiff, v. ALLERTON LOUNGE, INC. and Angel Cortes, D/b/a Bottom Line, Et Al., Defendants.JNomicsNo ratings yet
- Corruption and Central Vigilance Commission: Made By: David Cyril Babu B.A. LLB (Honours) Viii Semester Roll No. 18Document162 pagesCorruption and Central Vigilance Commission: Made By: David Cyril Babu B.A. LLB (Honours) Viii Semester Roll No. 18T M Santhosh KumarNo ratings yet
- Pan Card Application FormDocument2 pagesPan Card Application FormKaran AggarwalNo ratings yet
- Fundamentals of Criminal Investigation Part 1Document3 pagesFundamentals of Criminal Investigation Part 1johnpaulacosta0% (1)
- White PlainsDocument12 pagesWhite PlainsstevensonaguinaldoNo ratings yet
- Breach of Fiduciary Duty CitesDocument24 pagesBreach of Fiduciary Duty CitesTruthsPressNo ratings yet
- Deadly Maxims of Law To Agents of The CrownDocument10 pagesDeadly Maxims of Law To Agents of The Crownsugar marmelateNo ratings yet
- Targeted Justice - 2nd Amended Complaint - Case No. 6:23-cv-00003 USDC Southern District of Texas Victoria DivisionDocument125 pagesTargeted Justice - 2nd Amended Complaint - Case No. 6:23-cv-00003 USDC Southern District of Texas Victoria DivisionHip-hop LegalNo ratings yet
- Opo - Letter Karanam ManasaDocument5 pagesOpo - Letter Karanam Manasananjundavardhan5No ratings yet
- 52 - Puncia V Toyota Shaw - G.R. No. 214399Document3 pages52 - Puncia V Toyota Shaw - G.R. No. 214399DAblue ReyNo ratings yet
- Consideration Revision Sheet McKendrickDocument18 pagesConsideration Revision Sheet McKendrickDaniella DanjumaNo ratings yet
- Himachal Pradesh University Gyan Path, Summer Hill, Shimla - 171 005 (For Private and Re-Appear Candidates)Document3 pagesHimachal Pradesh University Gyan Path, Summer Hill, Shimla - 171 005 (For Private and Re-Appear Candidates)Sunny Music Productions100% (1)
- Belisario Vs IacDocument2 pagesBelisario Vs IacArvin Guevarra100% (1)