Professional Documents
Culture Documents
Antifungal PDF
Antifungal PDF
Uploaded by
Umashankar SharmaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Antifungal PDF
Antifungal PDF
Uploaded by
Umashankar SharmaCopyright:
Available Formats
ANTIFUNGAL DRUGS
1 . Introduction
Invasive fungal infections represent a global problem resulting in 1.7 million deaths every
year [1,2]. They are common in immunocompromised patients, as reflected in their
chemotherapy, acquired immune deficiency syndrome, and/or organ transplantation [1]. The
recent annual incidence of invasive aspergillosis, candidiasis, and mucormycosis is over
300,000, 750,000, and 10,000 cases, respectively [3]. The incidence of mucormycosis may
exceed 900,000 cases per year after the inclusion of Indian data estimates [4]. Furthermore,
these infections are associated with high mortality rates. The epidemiology of invasive fungal
infections usually focuses on specific areas. The lack of available global data leads to a broad
range of mortality rates, e.g., 30%–95% and 46%–75% in invasive aspergillosis and
candidiasis, respectively [5]. The overall incidence of disseminated scedosporiosis and
fusariosis is one [6] or six [7] cases per 1000 hematopoietic stem cell transplant recipients.
Currently, four antifungal drug classes are used by clinicians and veterinarians for systemic
treatment [8]. These classes target different parts of the fungal cell. First, the polyene class
includes the heptaene amphotericin B (AMB), which interacts with ergosterol, the major part
of the fungal cell membrane. AMB is highly fungicidal against Candida genera [9] and
Aspergillus fumigatus and A. flavus [10]. Second, first‐ and second‐generation of triazoles
disrupt the ergosterol biosynthesis in the lanosterol demethylation step. Generally, triazoles
exhibit the fungistatic effect against yeasts but are fungicidal for Aspergillus spp. [11].
Echinocandins block the synthesis of β‐D‐glucans located in the fungal cell wall.
Echinocandins are fungicidal and fungistatic against Candida and Aspergillus spp.,
respectively [12]. Finally, the pyrimidine analogue flucytosine (5‐FC) interacts at the nucleus
level of the fungus, affecting protein and deoxyribonucleic acid (DNA) biosynthesis [8]. The
overuse of antifungal agents increases the opportunistic pathogen resistance [13]. The World
Health Organization has identified this type of antimicrobial resistance as one of the dominant
threats of 2019 [14].
In this work, we reviewed the important approved and selected experimental antifungal drugs.
Immunomodulatory therapies [15,16], covering both molecular and cell‐based therapies, were
not the subject of this manuscript. Similarly, the application of mycoviruses or therapeutic
enzymes to degrade fungal biofilms or cell wall structures has not been included in the
present communication and can be found elsewhere.
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 1
ANTIFUNGAL DRUGS
2 . Overview of Antifungal Agents and Their Mechanisms of Action
Since the 1950s, more than 200 polyenes with antifungal activity have been discovered; however,
amphotericin B remains the single polyene drug of choice in the treatment of invasive fungal
infections [19]. 5‐Flucytosine was first designed and used as the antimetabolite in cancer
treatment. As its antineoplastic activity was low, 5‐FC now serves in combinational antifungal
therapy [20]. Whereas fluconazole (FLC) and itraconazole (ITC) are first‐generation
triazoles, the second‐ generation of triazoles, with improved pharmacological profiles,
include voriconazole (VOR), posaconazole (POS), and isavuconazole (ISV) [21].
Caspofungin (CSF), micafungin (MCF), and anidulafungin (ANF) represent the newest class
of peptide antifungals called echinocandins. The chronology of antifungal application and
development is shown in Figure 1. The power of combination therapy in the treatment of
invasive fungal infections was summarized recently [22].
Amphotericin B is a cyclic heptaene (Figure 2A) produced by the Gram‐positive bacterium
Streptomyces nodosus. It has two mechanisms of action (Figure 3). First, several molecules of
AMB incorporate into the fungal lipid bilayer and bind to ergosterol. By ergosterol
sequestration, pores are formed, and both the ions (K+, Mg2+, Ca2+, and Cl−) and electrolyte
glucose are released. The rapid depletion of intracellular ions results in fungal cell death.
Second, AMB induces the accumulation of reactive oxygen species (ROS), resulting in DNA,
protein, mitochondrial, and membrane damage [23]. The structural parts mycosamine and
hydroxyl groups at the C8, C9, and C35 positions are critical for the AMB biological activity
[24].
5‐Flucytosine (Figure 2B) is a synthetic analogue of cytosine. After administration, 5‐FC is
taken up by cytosine permease into the fungal cell and deaminated to 5‐fluorouracil (Figure
2C) by cytosine deaminase. 5‐Fluorouracil is subsequently converted into 5‐fluorouridine
triphosphate. Unlike uridylic acid, this compound is incorporated into fungal ribonucleic acid
(RNA), resulting in inhibition of protein synthesis (Figure 3). Besides, 5‐fluorouracil can be
metabolized to the 5‐ fluorodeoxyuridine monophosphate by uridine monophosphate
pyrophosphorylase. This compound inhibits the primary source of thymidine in DNA
biosynthesis, thymidylate synthetase, due to the enzyme’s inability to remove the fluorine
atom [25].
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 2
ANTIFUNGAL DRUGS
Figure 1. Sixty‐five years of antifungal therapy. Most antifungal agents were discovered in
the most recent three decades. Colored dots refer to specific antifungal drug class—polyenes
(blue), pyrimidine analogues (purple), triazoles (green), and echinocandins (orange).
Antifungal drugs under development and/or testing in clinical trials are marked black (see the
chapter Antifungal pipeline for further information). AMB = amphotericin B, 5‐FC =
flucytosine, FLC = fluconazole, ITC = itraconazole, CSF = caspofungin, VOR =
voriconazole, MCF = micafungin, POS = posaconazole, ANF = anidulafungin, ISV =
isavuconazole, SUBA‐ITC = super bioavailable itraconazole.
The mechanism of action of triazoles (Figure 2D–H) is based on the inhibition of the
microsomal cytochrome P450 (CYP450) monooxygenase dependent 14‐α‐demethylase
(Figure 3). The demethylation of fungal lanosterol is a two‐step process involving the reduced
form of nicotinamide dinucleotide phosphate (NADPH) and oxygen. As nitrogen from the
triazole ring binds to the heme iron, oxidation of the methyl group is prevented. The
combination of the accumulation of toxic 14‐α‐ methylsterols and depletion of ergosterol
results in the fungistatic effect [26].
Echinocandins are modified analogues of pneumocandins and are fermentation products of a
variety of microorganisms. Namely, anidulafungin is derived from echinocandin B0
(Aspergillus nidulans), caspofungin from pneumocandin B0 (Glarea lozoyensis), and
micafungin from pneumocandin A0 (Coleophoma empetri). Echinocandins are targeted
against 1,3‐β‐D‐glucan synthase (Figure 3), the enzyme complex composed of the
transmembrane catalytic Fks and intracellular regulatory Rho1 subunits. The former is
non‐competitively inhibited; therefore, 1,3‐β‐D‐glucan synthase cannot convert uridine
diphosphate glucose to a β‐D‐glucan, and the fungal cell wall becomes highly permeable [27].
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 3
ANTIFUNGAL DRUGS
Echinocandins are cyclic hexapeptides with specific lipophilic N‐‐ acetylated side chains
(Figure 4A–C).
C). Their core determines their physicochemical properties
properties— homotyrosine
inhibits 1,3‐β‐D‐glucan
β‐D‐glucan synthase; proline residues enhance antifungal potency; and
substitution with a hydroxyl group, ethylenediamine, and sulph
sulphated
ated moieties improve water
solubility. Because the linoleoyl side chain in echinocandin B0 exhibit the hemolytic activity,
it has been modified to a dimethylmyristoyl, diphenyl substituted isoxazole, and
alkoxytriphenyl chain [12,28].
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE
SCIENCE-PHARMACY Page 4
ANTIFUNGAL DRUGS
Figure 3. Mechanisms of actions of antifungals in the fungal cell. ((A): ): In the fungal
cytoplasm, AMB induces ROS formation resulting in the mitochondrial, biomembrane, DNA,
and protein damage. Furthermore, 55‐FC
‐FC prevents DNA, RNA, and thus protein biosynthesis.
(B): In the fungal biomembrane, 1,3‐β‐D‐glucan
1,3 β‐D‐glucan synthase (1) and 14‐α‐demethylase (2) are
inhibited by echinocandins and triazoles, respectively. Additionally, ergosterol contained in
the biomembrane is sequestered by AMB, resulting in pore formation
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE
SCIENCE-PHARMACY Page 5
ANTIFUNGAL DRUGS
3 . Classes of antifungal agents
Most antifungal drugs interfere with biosynthesis or integrity of ergosterol, the major sterol in
the fungal cell membrane. Others cause disruption of the fungal cell wall. Based on their
mechanism of action,12 the major agents can be grouped into five classes:1 polyenes; azoles;
allylamines; echinocandins; and other agents, including griseofulvin and flucytosine.
Antifungal agents
Azole antifungal agents
These are the most widely used antifungal drugs, and act primarily by inhibiting the fungal
cytochrome P450 enzyme, 14-demethyl- ase. There are two groups in clinical use: the
imidazoles (ketocon- azole, miconazole, clotrimazole, and econazole) and the triazoles
(fluconazole, itraconazole, voriconazole, and posaconazole). As the triazoles have greater
affinity for fungal compared with mam- malian P450 enzymes, their safety profile is
significantly improved over the imidazoles. The use of imidazoles is limited to treating
superficial mycoses and is only briefly discussed (see “Superficial fungal infections”). The
triazoles have broad application in therapy of both superficial and IFIs. Box 1 presents the
drug profiles of the four clinically important triazoles; detailed pharmacological and efficacy
data are available in recent articles and in the relevant product information.
First generation triazole agents
Fluconazole has good overall activity against Candida species and Cryptococcus neoformans.
However, resistance to the drug is encountered in certain non-albicans Candida species such
as C. krusei and some isolates of C. glabrata.4 It is available as oral and intravenous
formulations (Box 1). Itraconazole has activity against yeasts and some moulds (including
Aspergillus), but is disadvan- taged by variable bioavailability and an unpleasant taste. In
Australia, two oral formulations (the intravenous preparation is not licensed) are available:
capsule, and oral solution. The bio- availability of the capsule form is highly influenced by
concomi- tant food intake, and there is considerable intra- and inter-patient variability in
plasma drug concentrations;20 the solution form has a more favourable pharmacokinetic
profile.21 Fluconazole is com- monly given once daily, but can be prescribed twice daily for
larger total daily doses. Itraconazole is usually given twice daily (Box 1).
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 6
ANTIFUNGAL DRUGS
Second generation triazole agents
Voriconazole and posaconazole are second-generation triazoles with an extended spectrum of
activity against yeasts, C. neoformans and moulds, including Aspergillus, Scedosporium and
Fusarium species.15,18 Voriconazole is active against fluconazole-resistant Candida species,
although cross-resistance has been observed. 15 Posaconazole, licensed in May 2007, is the
broadest spectrum azole to date. Cross-resistance with fluconazole is uncommon, and
posaconazole is the only azole with clinical activity against zygo- mycete fungi. 14,17 Both
drugs are available as oral formulations and are easily administered (Box 1); voriconazole is
also available for intravenous use (in a sulfobutyl betadex sodium vehicle). Voricon- azole is
administered twice daily. Posaconazole is usually pre- scribed initially in four divided doses
to achieve adequate plasma levels, but may be given twice daily in non-life-threatening
situations.14 Its absorption is improved when taken with food or nutritional supplements (Box
1).
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 7
ANTIFUNGAL DRUGS
4 . Adverse effects
In general, the triazoles are relatively safe, even when used for prolonged periods. The main
adverse reactions are shown in Box 1. All triazoles can cause hepatotoxicity, but only 5%–7%
of patients require treatment cessation. Hepatic reactions range from mild transient elevations
in transaminases to clinical hepatitis, cholestasis and liver failure.2,15,16 These reactions are
idiosyncratic, so there is no cross-sensitivity between triazoles. The major drawback associ-
ated with triazole use relates to their metabolism by the hepatic cytochrome P450 (CYP)
enzyme system (mainly CYP2C9, CYP2C19 and CYP3A4). Triazole levels are affected by
other drugs metabolised by this pathway.13,15,17 Because triazoles also inhibit CYP enzymes,
plasma levels of any drug metabolised by these enzymes may be elevated (see Box 2 for the
major drug interactions). Concomitant use of a triazole and such a drug, where not
contraindicated, must be accompanied by monitoring of plasma drug levels (Box 2). The
potential for drug–drug interactions is greatest for itraconazole and voriconazole, 16-19 but
lower for posaconazole and fluconazole, as these azoles are not metabolised to the same
extent by the CYP system (Box 1).14,16 Conversely, CYP isoenzyme inducers substan- tially
decrease plasma triazole levels. The most clinically significant interaction occurs with
rifampicin, where concomitant use with itraconazole, voriconazole and posaconazole is
contraindicated (Box 2). Where possible, rifampicin should not be used in conjunction with
fluconazole.
AMB formulations
AMB formulations are commonly used to treat fungal infections. All have a similarly broad
spectrum of activity against a wide range of fungal pathogens.
AMB deoxycholate
Conventional AMB or AMB deoxycholate has long been used to successfully treat various
yeast, cryptococcal and mould infec- tions.22,23 Unfortunately, its clinical use is hindered by
intrinsic toxicity and the requirement for intravenous administration. Dose- dependent
nephrotoxicity is frequently encountered with thera- peutic doses (Box 3). Although renal
failure is usually reversible, permanent renal failure may occur. Infusion-related adverse reac-
tions and thrombophlebitis are common even with preventive measures (Box 3)
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 8
ANTIFUNGAL DRUGS
Lipid preparations of AMB
Two of three marketed lipid formulations of AMB are licensed in Australia: liposomal AMB
and AMB lipid complex (Box 3). Their development has substantially reduced, but not
eliminated, neph- rotoxicity; other AMB-associated adverse effects also occur less frequently
(Box 3). Other advantages include the ability to admin- ister larger doses of AMB. Although
at least as efficacious as conventional AMB in treating IFIs, lipid formulations have not been
shown to be more effective.23 They are substantially more expensive than conventional AMB,
but despite this, have become the “standard of care” for seriously ill patients with actual or
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 9
ANTIFUNGAL DRUGS
potential renal compromise. The choice of antifungal agent, or between different formulations
of a particular drug, depends primarily on the specific pathogen and clinical setting. With
expensive drugs, the cost–benefit ratio should be considered on an individual patient basis. A
number of pharmacoeconomic analyses of the use of lipid-associated AMB and triazole
agents have been published.24,25
AMB formulations are given as single daily doses by slow (2–4 hours) intravenous infusion
(see Box 3 for usual dosing sched- ules). Conventional AMB oral suspension or lozenges are
not absorbed, but may be used for oral candid- iasis (see later). AMB is extensively bound to
tissue, although the relationships between serum and tissue concentrations and clinical
efficacy or toxicity are unclear. Penetration into cerebrospinal fluid (CSF) is poor, and yet
AMB is effective in treating certain causes of fungal meningitis (eg, cryptococcosis).
Echinocandins
There are three clinically important echi- nocandins. Caspofungin is the first to be licensed in
Australia. Micafungin is only approved in Japan and the United States. Anidulafungin is
currently undergoing review for marketing in Australia. All three show good in vitro activity
against Candida and Aspergillus species, but are not active against C. neoformans or non-
Aspergillus moulds.13,26
Caspofungin is as effective as conven- tional AMB for treating mucosal and sys- temic
candidiasis, and is approved for treating such infections.13,26-28 It is also effective as salvage
therapy for invasive aspergillosis, but has yet to be evaluated for primary treatment of mould
infec- tions.13,26 Penetration into tissue is good, although CSF levels are low. Caspofungin is
available only as an intravenous formula- tion (oral bioavailability, < 0.2%). Owing to the
long half-life, it can be administered
once daily. The recommended dose is a 70 mg loading dose followed by 50 mg daily. Dose
adjustment in renal impairment is not required. However, in moderate hepatic insufficiency
(Child– Pugh score B), dose reduction is recommended; after the initial loading dose, the
subsequent daily dose should be 35 mg.28
Toxicity associated with echinocandins is infrequent because their action is specific to fungal
cell walls (glucan is not found in mammalian cells). They are not metabolised via the
cytochrome P450 enzymes, so there are minimal drug–drug interactions. An exception is
cyclosporin, for which concomitant use is not recom- mended because of the risk of raised
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 10
ANTIFUNGAL DRUGS
liver transaminase levels. Hepatitis is otherwise rare. Other adverse effects include histamine
release reactions (irritation at infusion site, headache, rash; 15%– 20%) and fever (10%–
35%).13,26
Terbinafine
Topical and oral preparations of this allylamine drug are widely used to treat nail and skin
infections, and terbinafine is the treatment of choice for onychomycosis (Box 4). The usual
dose is 250 mg once daily. There are also anecdotal reports of its value in certain invasive
mould infections (eg, scedosporiosis) in combina- tion with either a triazole or AMB
formulation.29,30 It is generally well tolerated, but may cause gastrointestinal upset, taste
distur- bance and transient elevation of liver enzymes. Dose reduction is required in the
presence of chronic liver disease.
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 11
ANTIFUNGAL DRUGS
FLUCYTOSINE
Flucytosine should not be administered as a single agent because of rapid development of
resistance. Its role is limited to use in combination with an AMB formulation for treating
cryptococcal meningitis.31 It is available as oral and intravenous formulations, with more than
90% of an oral dose absorbed. Gastrointestinal effects are uncommon, but bone marrow
toxicity and hepatotox- icity may occur. Monitoring of serum drug levels is required.
Superficial fungal infections
Fungal infections of the skin (level of evidence E31) or mucosa (E2) can usually be
successfully managed by topical imidazole preparations (see Box 5 for level-of-evidence
codes).32 Topical nystatin preparations may also be effective for skin or mucosal candidiasis,
including uncomplicated vulvovaginal infections (Box 4). For recurrent yeast infections,
oesophageal candidiasis and infection unresponsive to topical agents, treatment with an oral
triazole drug is indicated, with fluconazole being the drug of choice (E2) (Box 4). In these
cases, species identification of the pathogen and determination of antifungal susceptibility are
recom- mended. If resistance to fluconazole develops, either caspofungin (E2) or
voriconazole (E2) may be used. Terbinafine is the treat- ment of choice for dermatophyte
infections where systemic treat- ment is indicated (E2) (Box 4). Although griseofulvin can be
used, safer and more effective alternatives are preferred.
Invasive fungal infections
Treatment of IFIs is usually initiated in hospitals, but is increas- ingly continued in the
outpatient setting. Box 6 presents guide- lines, based on national and international
recommendations, for the use of antifungal agents in treating the major systemic mycoses.
Specific treatment details for various IFIs are given in recently published articles.19,30,31,33-35
Invasive candidiasis, which includes bloodstream infections (candidaemia), is the most
frequently encountered IFI. Although C. albicans remains the commonest causative species
(40%–50% candidaemias),36 clinicians should be alert to the rise in infections due to azole-
resistant Candida species. In patients with candid- aemia, it is essential to exclude
dissemination of infection to other body sites (eg, endopthalmitis, endocar- ditis, or
osteomyelitis), as this influences treatment duration and has prognostic implications.
Aspergillus fumigatus and other Aspergillus species are common pathogenic moulds and
cause major mor- bidity, especially in neutropenic, and organ-transplant patients.3,6 Other
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 12
ANTIFUNGAL DRUGS
moulds, such as Scedosporium and the zygomycetes, albeit less common, are associated with
high mortality (at least 60%) depending on site of infection and host factors. 3,6 In all cases,
accurate iden- tification of the pathogen is critical to selecting appropriate antifungal therapy
(Box 6) given the resistance of emerging fungi to many antifungal agents. Endemic mycoses
caused by dimorphic fungi are rare; only histoplasmosis can be acquired in Australia.
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 13
ANTIFUNGAL DRUGS
5 . Combination antifungal therapy
The only fungal infection for which com- bination therapy is of proven clinical benefit is
cryptococcocal meningitis where treatment with AMB formulations plus flucytosine results in
higher cure rates and more rapid CSF sterilisa- tion.31,37 However, with the availability of
potent extended-spectrum azoles, safer AMB formulations and the novel echinoc- andins,
combination antifungal therapy is conceptually appealing, especially for very ill patients with
poor prognosis. There are, for instance, reports of suc- cessful outcomes following
combination therapy with voriconazole and terbin- afine for Scedosporium prolificans infec-
tion.29,30 The cases for (eg, poor outcomes associated with monotherapy) and against (eg,
increased drug toxicity) combination therapy have been compre-
hensively reviewed, particularly for the treatment of aspergill- osis.37-39 Studies in vitro and in
vivo indicate triazole– echinocandin combinations are often synergistic, sometimes indif-
ferent, although never antagonistic; however, combinations of a polyene (AMB) with a
triazole show conflicting data.37-39 As results of preclinical studies cannot be used to direct
clinical decisions, and in the absence of prospective, comparative data in humans, selecting
patients that could benefit from combination therapy should be done individually.
Adjunctive therapy
Surgery may be required in instances such as fungal endocarditis or for large isolated lesions
(eg, pulmonary cryptococcomas) that persist despite antifungal treatment (E4). 31,34
Aggressive surgical debridement is also mandatory in zygomycete infections (E4); for these
infections, there are anecdotal reports of successful outcomes with adjunctive hyperbaric
oxygen therapy and, more recently, iron chelation therapy (E4). The role of adjuvant
recombinant cytokine therapy such as granulocyte-macrophage-stimulating fac- tor in
improving the host immune response remains investiga- tional. Most recently, an approach
using a monoclonal antibody against a fungal heat shock protein in combination with lipid-
associated AMB resulted in improved outcomes for patients with invasive candidiasis (E2).40
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 14
ANTIFUNGAL DRUGS
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 15
ANTIFUNGAL DRUGS
6 . Pharmacology and Toxicity of Antifungal Agents
In the drug formulation, amphotericin B is bound to sodium deoxycholate because of its limited
solubility in water. After intravenous administration, AMB dissociates from deoxycholate,
binds to plasma lipoproteins, and accumulates in the spleen and liver. With the elimination
half‐life of over 15 days, AMB is not metabolized by CYP450 enzymes, but is excreted into
the urine (33%) and feces (43%) as the unchanged drug. The inherent limitations of AMB
deoxycholate application consist in its infusion‐ and dose‐related toxicity. The
infusion‐related toxicity arises from the induction of pro‐ inflammatory cytokines and
chemokines such as interleukin 1β, tumor necrosis factor α, monocyte chemotactic protein 1,
and macrophage inflammatory protein 1β. On the other hand, high doses of AMB cause
nephrotoxicity due to the non‐selective disruption of renal cells. To reduce these undesirable
effects, AMB deoxycholate has been incorporated into lipidic formulations still retaining its
fungicidal activity. Three lipidic formulations are commercially available: AMB lipid
complex (ABLC), liposomal AMB (LAMB), and AMB colloidal dispersion (ABCD) [29].
In contrast, 5‐flucytosine, as a small hydrophilic molecule, is absorbed rapidly, and its
bioavailability reaches almost 90%. Liver enzymes metabolize 5‐FC minimally. It is
eliminated exclusively via glomerular filtration with excellent antifungal activity in the
bladder, and its plasma clearance is as fast as creatinine clearance. 5‐FC is dosed frequently
because of its half‐life, which is up to four hours. Co‐administration of 5‐FC with the
cytarabine (an effective drug for the treatment of acute myeloid leukemia [30]) competitively
inhibits its antifungal activity due to the same transport system by susceptible cells. Severe
side effects include hepatotoxicity, myelotoxicity, and gastrointestinal problems [20].
The pharmacological profiles of triazoles vary with their molecular weight, solubility, and
protein binding. Selected pharmacological data are presented in Table 1. All triazoles are
available both for peroral and intravenous applications. Notably, isavuconazole is
administered as the water‐ soluble prodrug isavuconazonium. Furthermore, the only
metabolism of itraconazole results in the active metabolite hydroxyitraconazole.
On the other hand, genetic polymorphisms of CYP2C19 and CYP3A4 affect the metabolism
of voriconazole. Generally, triazoles are well tolerated. The most common serious side effect,
hepatotoxicity, occurs most often with VOR (in 31% cases). Whereas ISV shortens the QT
interval (the time between the start of the ventricular depolarization and the end of the
ventricular repolarization), the rest of triazoles act in the opposite way. Unfortunately,
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 16
ANTIFUNGAL DRUGS
triazoles have many potential drug–drug interactions due to their affinity for CYP450
isoenzymes [31].
Triazole FLC ITC [33] VOR [34] POS [35] ISV [36]
[32]
Bioavailability [%] 90 55 90–96 variable >98
Protein binding11–12 99 51–67 >98 >99
[%]
Metabolism (CYP) – 3A4 2C19/2C9/3A glucuronidatio 3A4/3A5
4 n
Half‐life [h] 27–37 15–42 6 15–35 80–130
Route ofrenal hepatic hepatic hepatic hepatic
elimination
Unchanged [%] 64–90 3–18 <2 66 45
Table 1. Pharmacological properties of triazoles.
Echinocandins have so far been approved for intravenous administration only. Selected
pharmacological data are presented in Table 2. High protein binding and negligible
metabolism by CYP450 are common among them; on the other hand, their half‐life and
degradation processes are different. Caspofungin has the lowest half‐life, and after the
spontaneous opening of the peptide ring, it is further degraded by both peptide hydrolysis and
N‐acetylation into two inactive metabolites. In contrast, anidulafungin has the longest
elimination half‐life. Its biotransformation results in an ineffective open‐ring peptide. Finally,
the metabolism of micafungin forms three metabolites by arylsulphatase,
catechol‐O‐methyltransferase (COMT), and CYP3A side‐chain hydroxylation (Figure 5).
Only the degradation products of CSF are excreted primarily into the urine. Echinocandins
have few known drug–drug interactions because of their reduced substrate potential to
CYP450 enzymes.
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 17
ANTIFUNGAL DRUGS
Figure 5. Metabolites of micafungin. Top: The original sulphate group (blue) on the
dihydroxyhomotyrosine amino acid residue is metabolized to a hydroxyl group followed by
its methylation. Bottom: the third and minor metabolite arises from hydroxylation of the
methyl group (orange) at the ω1 position of the lipophilic side chain. COMT =
catechol‐O‐methyltransferase.
Adequate antifungal dosing strategies are necessary for ensuring successful treatment. The
optimal antifungal dosages vary by given patient populations and include both patient
physical condition
ndition and type of treatment. Therefore, dosage recommendations are written in
several guidelines and review articles, including aspergillosis and candidiasis in neonates
[42], pediatrics [43], and adults [44,45]. These recommendations are summarized and
simplified in Table 3. Furthermore, antifungal prescription for pregnant women is a challenge
due to the limited information about embryotoxic/teratogenic effects. According to the Food
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE
SCIENCE-PHARMACY Page 18
ANTIFUNGAL DRUGS
and Drug Administration classification, only AMB is considered as the safest drug for the
treatment of systemic fungal infection. The rest of antifungals has a worse reputation because
of indication and/or positive evidence of fetal risk based on animal studies [46]. Dose
improvement is also necessary for the obese population due to their often exclusion from drug
development studies resulting in limited pharmacological data for antifungals. Whereas FLC,
CSF, and MCF are correlated with total body weight, dosing alterations are not necessary for
POS, AMB, and ANF [47].
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 19
ANTIFUNGAL DRUGS
7 . Susceptibility of Antifungal Agents
Antifungal susceptibility testing (ast) is a must for both the optimal treatment and the
detection of possible antifungal resistance. Ast is performed by both reference and commercial
methods based on broth microdilution and agar‐based (or disk diffusion) assays. These assays
are standardized according to the european committee on antimicrobial susceptibility testing
(eucast) [49] and the clinical and laboratory standard institute (clsi) [50]. Although the
reference broth microdilution methods are the gold standard for ast, they are time‐consuming
and laborious. Therefore, commercial methods have been developed for daily ast. These
methods are automated or semi‐automated, rapid, and low cost [51].
To distinguish if the microorganism isolates are resistant to antifungal agents or not,
eucast and clsi have set clinical breakpoints expressed as the minimal inhibitory concentration
(mic), indicating the minimum drug concentration that inhibits fungal growth. According to
the 2019 eucast definition [52], a microorganism can be categorized into the s (susceptible,
standard dose regime), i (susceptible, increased exposure), or r (resistant) category.
Additionally, clsi distinguishes between sdd (susceptible, dose‐dependent) and ns
(non‐susceptible) category [53]. Despite the slight methodological differences, both clsi and
eucast yield comparable mic data. Unluckily, clsi has not determined the clinical breakpoints
against any molds [54]. Therefore, modified data presented in tables 4 and 5 summarize the
susceptibilities of antifungal agents against selected aspergillus and candida species covering
the period 2007–2019 from eucast only [55].
The european society for clinical microbiology and infectious diseases (escmid) published
guidelines for the management of aspergillus [45], candida [44], fusarium, and scedosporium
[56] infections. In these guidelines, the correct selection of an antifungal agent is based on the
clinical experience, case studies, clinical trials, and population of patients. Therefore,
voriconazole is also recommended for the management of aspergillosis caused by a. Terreus
and a. Niger. Furthermore, vor should be used in both first‐line and salvage therapy in
immunocompromised patients suffering from fusariosis and scedosporiosis. In the case of
candidemia and invasive candidiasis, the use of all three echinocandins (including
caspofungin) is strongly recommended as an initial targeted treatment in the adult population
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 20
ANTIFUNGAL DRUGS
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 21
ANTIFUNGAL DRUGS
8. Resistance to Antifungal Agents
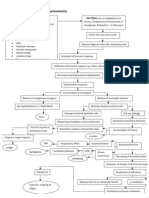
Microbial resistance to antifungal drugs is a result of multiple factors and emerges by a
series of molecular mechanisms (Figure 6). Whereas some intrinsic resistance has been
found naturally, e.g., fluconazole‐resistant C. krusei [57], C. glabrata [58], and Aspergillus
species [59], the acquired resistance has been a consequence of long‐term therapies,
widespread prophylaxis, or use of antifungals in agriculture, especially in the case of
triazoles [60]. Environmental exposure of A. fumigatus to triazole fungicides may explain
their resistance in azole‐naïve patients [61]. Additionally, secondary resistance may occur
after vertical and horizontal transmission in both animals [62] and humans.
Amphotericin B susceptibility depends on the ergosterol content in the fungal cell
membrane. Ergosterol biosynthesis is regulated by 25 known ERG enzymes [66]; their
alterations (ERG3, ERG5, ERG11), gene deletion (ERG11), and harbored mutations
(ERG1, ERG2, ERG6, ERG11) lead to the decreased AMB sensitivity in Candida species
[67]. Furthermore, resistant C. tropicalis isolates showed a thickened cell wall due to the
increased content of 1,3‐β‐D‐glucans [68]. On the other hand, the higher activity of
catalase and superoxide dismutase and the more intense stress response through heat shock
proteins 70 and 90 (Hsp70, Hsp90) contribute to the intrinsic resistance of A. terreus [69].
5‐Flucytosine is known for its rapid development of resistance; therefore, it is used only in
combination therapy with AMB and triazoles. Primary and secondary resistance in
clinically relevant Candida spp. have emerged as a consequence of alterations in the FCY2,
FCY1, and FUR1 genes responsible for 5‐FC uptake and its conversion, respectively.
Additionally, the susceptibility of C. glabrata to 5‐FC increased after deletion of the
CgFPS1 and CgFPS2 homologue encoding plasma membrane aquaglyceroporins that are
required for osmotic stress resistance [70]. It has been shown that 5‐FC activity increases
up to 4000‐fold against A. fumigatus at pH 5. Furthermore, FCYB gene expression is
repressed by the cytosine‐cytosine‐adenosine‐adenosine‐thymidine binding complex
(CBC) and pH‐response transcriptional factor PacC at pH 7, confirming intrinsic resistance
[71].
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 22
ANTIFUNGAL DRUGS
Figure 6. The emergence of microbial resistance is given by three main factors, including c
hoice of antifungal treatment, type of fungal species, and patient medical history. For exam
ple, adequate dosing and distinguishing between fungistatic/fungicidal drug effects are ma
ndatory for successful treatment. Unfortunately, repeated antifungal therapy and often pro
phylaxis narrow the appropriate drug selection. With the fungal biofilm formation, this tas
k becomes more problematic. Furthermore, fungi often decrease drug concentration by effl
ux pump activation or target overexpressionAdditionally, these targets can be amplified or
changed due to several types of mutations, such as
amino acid substitution. Modified from [64,65].
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 23
ANTIFUNGAL DRUGS
The first mechanism of azole resistance involves amino acid substitutions near the heme
binding site of 14‐α‐demethylase or overexpression of the ERG11/CYP51A/CYP51B
genes included in ergosterol biosynthesis. The overexpression of ERG11 is due to
gain‐of‐function mutations in Upc2 in C. albicans. Furthermore, another transcriptional
factor SrbA is required for azole resistance in A. fumigatus. The second mechanism of
acquired azole resistance arises from the upregulation of ABC (adenosine triphosphate
binding cassette) transporters as well as major facilitators responsible for higher drug
efflux [13]. Cdr1, Cdr2, and Mdr1 are responsible for azole efflux in C. albicans, and AtrF,
Mdr3, and Mdr4 in A. fumigatus, respectively. Furthermore, intrinsic resistance to triazoles
is often caused by Candida biofilm formation [72].
The basis of echinocandin resistance consists of amino acid substitutions in the FKS1 and
FKS2 subunits of glucan synthase. The most frequent amino acid changes encompass
Ser641 and Ser645 in C. albicans and Ser629, Phe659, and Ser663 in C. glabrata.
Moreover, the elevated MIC values in C. parapsilosis are due to naturally occurring
polymorphisms linked with the proline‐to‐alanine change in FKS1. FKS2‐dependent
resistance in C. glabrata can be reversed by treatment with the calcineurin inhibitor
tacrolimus. Treatment with echinocandins is connected with higher biosynthesis of β‐D‐
glucans and chitin in C. glabrata and C. parapsilosis. The higher molecular weight cell
wall content may play a role in echinocandin resistance [73]. In addition, protection against
cell wall weakening is induced through a variety of stress adaption mechanisms involving
protein kinase C, calcineurin, and Hsp90 [74].
The clinically relevant Fusarium spp. (especially F. solani complex, F. oxysporum, and F.
fujikuroi complex [75]) are resistant to amphotericin B, triazoles, and echinocandins. In the
case of triazoles, the combination of CYP51A amino acid substitution and/or gene
overexpression may be involved. In FKS1, the changes of Phe639 to Tyr and Pro647 to
Ala contribute to echinocandin resistance. Moreover, cross‐resistance has been observed
among both triazoles and echinocandins . The Scedosporium species have intrinsically low
susceptibility or high resistance to azoles; furthermore, their echinocandin resistance is due
to the Trp‐to‐Phe substitution at position 695. Mucormycetes are resistant to short‐tailed
triazoles voriconazole and fluconazole. The molecular mechanism resistance comprises the
Phe129 substitution for Tyr in the paralogue gene CYP51 F5, including the possible
contribution of Val‐to‐Ala substitutions at positions 291 and 293. On the other hand,
isavuconazole, posaconazole, and itraconazole usually provide effective treatment [78].
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 24
ANTIFUNGAL DRUGS
9. The Antifungal Pipeline
The research in antifungal drug development focuses on both old and new fungal targets.
In addition, antifungal susceptibility testing and ongoing clinical trials have modified
already licensed antifungals, i.e., drugs with originally different purposes or novel
synthesized substances (Table 6).
In ergosterol biosynthesis, modified tetrazoles (VT‐1129, 1161, 1598; Figure 7A–C) show
higher specificity to the fungal Cyp51 [84]. The new triazole PC1244 (Figure 7D) has
recently been reported and is specifically designed to be inhaled and persists at high
concentrations in the lungs for a long time [82]. To enhance bioavailability of itraconazole
after oral administration, new super bioavailable itraconazole (SUBA‐ITC) has been
developed. This SUBA‐ITC comprises its solid dispersion in a pH‐ dependent matrix
ensuring doubled bioavailability compared to the original ITC formulation [85].
Furthermore, coumarins and aminopiperidines as non‐azole compounds inhibit ERG11 and
ERG24, respectively. Aminopiperidines show antifungal activity against
fluconazole‐resistant Candida spp. and A. fumigatus [86]. In addition to ergosterol
sequestration, amphotericin B cochleate (CAMB) has been developed as an oral
formulation of AMB. CAMB is made up of phosphatidylserine and phospholipid‐calcium
precipitates and demonstrates successful treatment in murine mouse model against C.
albicans [85].
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 25
ANTIFUNGAL DRUGS
In β‐D‐glucan synthesis, newly developed molecules include rezafungin (CD101, Figure
7E) with an extended half‐life (>80 h), enabling once‐weekly intravenous dosing.
Rezafungin is a peptide that has not yet passed all the phases of testing [22]. Ibrexafungerp
(SCY‐078, Figure 7F) is a triterpenoid and is one of the first glucan synthase inhibitor
administered per os [84]. Both agents have low rates of drug–drug interactions and
excellent safety profiles [23]. However, neither is active against mucormycetes.
Contemporary research is directed towards novel fungal targets, especially enzymes
involved in other metabolic pathways [87]. The inositol acyltransferase inhibitor
Fosmanogepix (APX001, Figure 7G) prevents microorganism colonization/adhesion [86]
and is effective against pulmonary scedosporiosis or fusariosis in immunocompromised
mice [88]. The dihydroorotate dehydrogenase inhibitor F901318 (Olorofim, Figure 7H),
the first representative of the orotomides, inhibits the pyrimidine biosynthesis and is active
against Aspergillus and Scedosporium spp., including Lomentospora prolificans [89].
Co‐administration of Hos2 fungal histone deacetylase inhibitor MGCD290 with both
azoles and echinocandins enhance fungicidal effect against Candida and Aspergillus spp.
[85]. Arylamidine T‐2307 (Figure 7I) is taken up via the spermine/spermidine transport
system and probably affects mitochondrial membrane potential balance in yeast [83].
Furthermore, monoterpenoids citronellal (Figure 7J) and perillaldehyde (Figure 7K)
enhance the ROS production in C. albicans, resulting in DNA and mitochondrial damage.
In this pathogen, inhibition of the prostaglandin E2 by cyclooxygenase inhibitors reduces
the biofilm development [90].
Acylhydrazones, inhibitors of fungal sphingolipid synthesis, showed promising results in
terms of efficacy and toxicity. For example, brominated acylhydrazone BHBM (Figure 7L)
and its derivative D13 (Figure 7M) were found to be highly effective against several
pathogenic fungi, including Cryptococcus neoformans, Cryptococcus gattii, Rhizopus
oryzae, Histoplasma capsulatum, Blastomyces dermatitidis, Pneumocystis murina, and
Pneumocystis jirovecii [91,92]. More antifungal compounds in development with novel
targets can be found in an excellent review by J.R. Perfect [87].
In particular, the basic experimental way of antimicrobial research focuses on
siderophores. Iron hijack belongs to profound virulence factors in infection; therefore,
disruption of iron assimilation offers three novel antimicrobial strategies. The first strategy
uses the siderophore‐antifungal drug‐ conjugate in a Trojan horse therapy that enables drug
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 26
ANTIFUNGAL DRUGS
delivery into the cytoplasm of the microorganism and drug release at the active site. These
conjugates arise naturally (sideromycins) or synthetically with antibiotics [93]. Next,
inhibition of nonribosomal peptide synthetases (NRPS), polyketide synthases, and
NRPS‐independent siderophore synthetases prevents iron scavenging [94]. As an example,
celastrol (Figure 7N) blocks A. fumigatus growth by the inhibition of flavin‐ dependent
monooxygenase siderophore A required for the L‐ornithine hydroxylation [95]. Last,
competitive iron chelators, such as lactoferrin and iron substitution by gallium, can reduce
biofilm formation [93]. Phosphopantetheine transferase inhibitors directly affecting
siderophore synthesis also represent the possible future antifungals [96,97], either alone or
in combination therapy.
It is worth mentioning that specialized mammalian cells secrete lipocalins preventing iron
hijack by catecholate‐type siderophore sequestration [98]. VL‐2397 (Figure 7O) is a hydro
xamate siderophore similar to ferrichrome. It was isolated from Acremonium spp. and exhi
bits significant activity against Aspergillus spp. The mechanism of action of this compoun
d is not known. Still, its selectivity for fungal cells derives from the fact that it is taken up
by the fungal siderophore transporter Sit1, which is absent from mammalian cells [99]. Bes
ides these approaches, siderophores can lead to an early, selective, and sensitive diagnosis
of infectious diseases [100], and their detection in urine is non‐invasive [101].
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 27
ANTIFUNGAL DRUGS
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 28
ANTIFUNGAL DRUGS
10 . Conclusion
Antifungal agents are essential for treating a wide range of fungal infections affecting the
body locally and systemically. However, there are a number of acute and chronic toxic
associations with the use of antifungals in humans and animals. Because of their toxicology
and adverse effects, clinicians must be both careful and specific when prescribing antifungals
to patients. The agent's route of exposure, therapeutic range, drug interactions, and organ
toxicities are important characteristics to consider. Additionally, a detailed patient history that
includes their current medications, allergies, and comorbidities can help to tailor the agent that
would be the most beneficial while also providing favorable toxicology.
The term ‘invasive fungal disease’ (IFD) encompasses a wide range of fungal infections,
ranging from candidiasis to aspergillosis, and from cryptococcosis to mucormycosis.1 The
risk factors and patient populations at risk of developing fungal infections also vary between
different fungal species. For example, Aspergillus is more common in patients with
haematological malignancies (allogeneic stem cell transplant recipients or patients receiving
chemotherapy for acute myeloid leukaemia) and in lung transplant recipients,2 while
cryptococcosis is historically associated with patients diagnosed with AIDS.3 Invasive
candidiasis (IC) and candidaemia can be considered good examples of the potential pitfalls in
the use and misuse of antifungal agents, and also of the limited guidance that is available in
how to reduce catheter-related infections.
There are a variety of challenges related to improving treatment for patients with IFD. For
example, IFDs frequently present with non-specific clinical manifestations, early diagnosis is
often difficult, and there is likely to be a high risk of toxicity and side effects associated with
antifungal treatment.4,5 This Supplement highlights the key factors for consideration for
optimal treatment of IFD, focusing on current issues with diagnosis, improvements in
treatment and the need to encourage effective and practical multidisciplinary plans for the
implementation of antifungal stewardship (AFS) programmes.
With regard to diagnosis, a recent study in 219 high-risk haematological patients
demonstrated that a combination of the serum galactomannan (GM) assay and PCR-based
detection of Aspergillus DNA in blood was associated with an earlier diagnosis of invasive
aspergillosis (IA).6 The Aspergillus lateral-flow device could also be an effective diagnostic
tool for IA, due to its high specificity, point-of-care diagnostic potential and reduced time to
perform when compared with the GM assay.7 As alluded to in this Supplement by
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 29
ANTIFUNGAL DRUGS
Maertens et al.,8 other biomarkers that may be useful for the diagnosis of IA are also in
development, such as the electronic nose (eNose) or the detection of bis(methylthio)gliotoxin
(bmGT). It is also important to note that in recent years, several non-culture-based tests for
the diagnosis of IC have been developed. 1,3-β-D-Glucan (BDG) testing, PCR-based tests and
detection of Candida mannan/antimannan antibodies in serum have been evaluated, showing a
high negative predictive value for the diagnosis of IC;9–11 PCR could therefore be an
efficacious test for promptly detecting Candida infection.12Candida antibody detection kits
are also under evaluation. As mentioned by Lortholary et al.,13 it has been demonstrated that
a multiplex quantitative PCR targeting 18S rDNA
of Mucor spp./Rhizopus spp., Lichtheimia complex and Rhizomucor spp. in combination may
be an effective diagnostic test to facilitate the early diagnosis of mucormycosis and serve as a
model for the diagnosis of other fungal infections.14 Semi-quantitative tools for detection of
cryptococcal polysaccharide antigen (CRAG) are also currently under evaluation to help
improve the diagnosis of latent cryptococcal meningitis. These tools may have the potential to
help improve the prognosis of patients, allowing earlier diagnosis and treatment; however,
most of these tools are not yet available in the majority of centres.
With regard to treatment, recent improvements in antifungal drugs have significantly
improved the prognosis of high-risk patients. As discussed by Bassetti et al.15 in this
Supplement, echinocandins have a strong fungicidal and biofilm activity, especially
against Candida, without the toxicity and side effects associated with azoles and amphotericin
B. These are now recommended as first-line drugs for the treatment of IC and candidaemia.16
However, despite the advances in the diagnosis and treatment of IFD in recent years, new
challenges are currently being faced in the management of IFD. One of the main questions
today relates to the costs associated with the management of these diseases. The treatment of
IFD is usually expensive and resources are often limited. The importance of attaining a cost-
effective treatment for patients has encouraged the development of multidisciplinary teams
and AFS programmes. As mentioned by Agrawal et al.17 in this Supplement,
multidisciplinary teams with clinical expertise in the management of IFD, as well as extensive
knowledge of fungal epidemiology and antifungal treatment options, are of great value when
considering how to optimize care for patients.18–20 These teams should be responsible for
implementing local AFS programmes, as referred to by Muñoz and Bouza,21 through a close
and continuous collaboration with different medical specialties (haematology, intensive care,
internal medicine, etc.). Multidisciplinary teams are able to advise on the most appropriate
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 30
ANTIFUNGAL DRUGS
antifungal drug depending on the type of patient/infection, e.g. by replacing inappropriate and
expensive antifungal drugs with those that may be less costly but equally effective, but also in
deciding which patients would benefit from antifungal prophylactic regimens or when an
empirical antifungal treatment could be safely withdrawn. Multidisciplinary teams can also
advise on which diagnostic tests are most appropriate for each patient, as well as aiding in
their interpretation. Several studies have proved that multidisciplinary teams and AFS
programmes are extremely effective in reducing the costs associated with the management of
IFD, although this effect often diminishes once their advisory work is
discontinued.22,23 Another potential key advantage of these programmes is that encouraging
the appropriate use of antifungal drugs will likely limit, and possibly decrease, the emergence
of antifungal resistance, which is currently a major concern in relation to the treatment of IFD.
The authors believe that, in the future, all hospitals should have their own antifungal
multidisciplinary team and a corresponding AFS programme.
In summary, the diagnosis and treatment of IFD remains challenging, and IFDs are often still
associated with significant morbidity and mortality.1 Although new diagnostic tests, such as
BDG or PCR, and the extended use of prophylactic regimens and empirical treatment have
reduced the burden of IFD, the treatment of these diseases is still associated with significant
challenges and costs. It appears advisable to implement multidisciplinary teams and AFS
programmes in order to encourage the appropriate use of resources, with the aim of
optimizing patient care in a cost-effective manner.
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 31
ANTIFUNGAL DRUGS
11 . References
1. Kauffman CA. New antifungal agents. Semin Respir Crit Care Med 2004; 25: 233-
239.
2. Sheehan DJ, Hitchcock CA, Sibley CM. Current and emerging azole antifungal
agents. Clin Microbiol Rev 1999; 12: 40-79.
3. Walsh TJ, Groll A, Hiemenez J, et al. Infections due to emerging and uncommon
medically important fungal pathogens. Clin Microbiol Infect 2004; 10 Suppl 1: 48-
66.
4. Pfaller MA, Diekma DJ. Rare and emerging opportunistic fungal patho- gens:
concern for resistance beyond Candida albicans and Aspergillus fumigatus. J Clin
Microbiol 2004; 42: 4419-4431.
5. Hajjeh RA, Sofair AN, Harrison LH, et al. Incidence of blood stream infection due
to Candida species and in vitro susceptibilities of isolates collected from 1998 to
2000 in a population-based active surveillance program. J Clin Microbiol 2004; 42:
1519-1527.
6. Marr KA, Carter RA, Crippa F, et al. Epidemiology and outcome of mould
infections in haematopoietic stem cell transplant recipients. Clin Infect Dis 2002;
34: 909-917.
7. Lin S, Schranz J, Teutsch S. Aspergillosis case-fatality rate: systemic review of the
literature. Clin Infect Dis 2001; 32: 358-366.
8. Gudlaugsson O, Gillespie S, Lee K, et al. Attributable mortality of candidaemia,
revisited. Clin Infect Dis 2003; 37: 1172-1177.
9. Ullmann AJ, Cornerly OA. Antifungal prophylaxis for invasive mycoses in high
risk patients. Curr Opin Infect Dis 2006; 19: 571-576.
10. Bow EJ, Laverdière M, Lussier N, et al. Antifungal prophylaxis for severely
neutropenic chemotherapy recipients. A meta-analysis of randomized- controlled
clinical trials. Cancer 2002; 94: 3230-3246.
11. Cornerly OA, Ullmann AJ, Karthaus M. Evidence-based assessment of primary
antifungal prophylaxis in patients with hematological malignan- cies. Blood 2003;
101: 3365-3372.
12. Georgopapadakou NH, Walsh TJ. Antifungal agents: chemotherapeutic targets and
immunologic strategies. Antimicrob Agents Chemother 1996; 40: 279-291.
13. Boucher HW, Groll AH, Chiou C, Walsh TJ. Newer systemic antifungal agents.
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 32
ANTIFUNGAL DRUGS
Drugs 2004; 64: 1997-2020.
14. Torres HA, Hachem RY, Chemaly RF, et al. Posaconazole: a broad- spectrum
triazole antifungal. Lancet Infect Dis 2005; 5: 775-785. Donnelly JP, De Pauw BE.
Voriconazole — a new therapeutic agent with an extended spectrum of antifungal
activity. Clin Microbiol Infect 2004; 10 Suppl 1: 107-117.
15. Pfizer Australia Pty Ltd. Product information: Diflucan (fluconazole).
16. Version pfpdiflb11206. 29 Dec 2006.
17. Schering-Plough, Australia. Product information: Noxafil oral suspension
(posaconazole). Version 060310. 2006.
18. Pfizer Australia Pty Ltd. Prescribing information: Vfend (voriconazole).
19. Version pfpvfend10406. 12 Apr 2006.
20. Sugar AM. Treatment of invasive aspergillosis. UpToDate 2007. http://
www.uptodate.com (accessed Sep 2007).
21. Poirier JM, Berlioz F, Isnard F, Cheymol G. Marked intra- and inter-patient
variability of itraconazole steady state plasma concentrations. Therapie 1996; 51:
163-167.
22. Barone JA, Moskovitz BL, Guarnieri J, et al. Enhanced bioavailability of
itraconazole in hydroxypropyl--cyclodextrin solution versus capsules in health
volunteers. Antimicrob Agents Chemother 1998; 42: 1862-1865.
23. Patel R. Antifungal agents. Part I. Amphotericin B preparations and flucytosine.
Mayo Clin Proc 1998; 73: 1205-1225.
24. Ostrosky-Zeichner L, Marr KA, Rex JH, Cohen SH. Amphotericin B: time for a
new “gold standard”. Clin Infect Dis 2003; 37: 415-425.
25. Wenzel R, Del Favero A, Kibbler C, et al. Economic evaluation of voriconazole
compared with conventional amphotericin B for the primary treatment of
aspergillosis in immunocompromised patients. J Antimicrob Chemother 2005; 55:
352-361.
26. Cagnoni P, Walsh TJ, Prendergast MM, et al. Pharmacoeconomic analysis of
liposomal amphotericin B versus conventional amphotericin B in the empirical
treatment of persistently febrile neutropenic patients. J Clin Oncol 2000; 18: 2476-
2483.
27. Denning DW. Echinocandin antifungal drugs. Lancet 2003; 362: 1142-
28. 1151.
29. Mora-Duarte J, Betts R, Rotstein C, et al. Comparison of caspofungin and
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 33
ANTIFUNGAL DRUGS
amphotericin B for invasive candidiasis. N Engl J Med 2002; 347: 2020- 2029.
30. Deresinski SC, Stevens DA. Caspofungin. Clin Infect Dis 2003; 36: 1445-
31. 1457.
32. Howden BP, Slavin MA, Schwarer AP, et al. Successful control of dissemi- nated
Scedosporium prolificans infection with a combination of voricon- azole and
terbinafine. Eur J Clin Microbiol Infect Dis 2003; 22: 111-113.
33. Steinbach WJ, Perfect JR. Scedosporium species infections and treat- ments. J
Chemother 2003; 15 (Suppl 2): 16-27.
34. Saag M, Graybill R, Larsen R, et al. Practice guidelines for the manage- ment of
cryptococcal disease. Clin Infect Dis 2000; 30: 710-718.
35. National Health and Medical Research Council. A guide to the develop- ment,
implementation and evaluation of clinical practice guidelines. Canberra: NHMRC,
1999.
36. Slavin MA, Szer J, Grigg AP, et al. Guidelines for the use of antifungal agents in
the treatment of invasive Candida and mould infections. Intern Med J 2004; 34:
192-200.
37. Pappas PG, Rex JH, Sobel JD, et al. Guidelines for treatment of candidiasis. Clin
Infect Dis 2004; 38: 161-189.
38. Greenberg RN, Scott LJ, Vaughan HH, Ribes JA. Zygomycosis (mucormy- cosis):
emerging clinical importance and new treatments. Curr Opin Infect Dis 2004; 17:
517-525.
39. Chen S, Slavin M, Nguyen Q, et al. Active surveillance for candidaemia, Australia.
Emerg Infect Dis 2006; 12: 1508-1516.
40. Baddey JW, Pappas PG. Antifungal combination therapy. Drugs 2005; 65: 1461-
1480.
41. Johnson MD, MacDougall C, Ostrosky-Zeichner L, et al. Combination antifungal
therapy. Antimicrob Agents Chemother 2004; 48: 693-715.
42. Meletiadis J, Petraitis V, Petraitiene R, et al. Triazole-polyene antagonism in
experimental invasive pulmonary aspergillosis: in vitro and in vivo correlation. J
Infect Dis 2006; 194: 1008-1018.
43. Pachl J, Svoboda P, Jacobs F, et al. A randomised, blinded, multicentre trial of
lipid-associated amphotericin B alone versus in combination with an antibody-
based inhibitor of heat shock protein 90 in patients with invasive candidiasis. Clin
Infect Dis 2006; 42: 1404-14
BHOPAL INSTITUTE OF TECHNOLOGY AND SCIENCE-PHARMACY Page 34
You might also like
- ILS L4 Transcripts PDFDocument38 pagesILS L4 Transcripts PDFThuy Lan75% (4)
- A1782 v1 Alere Triage MeterPro Training ManualDocument13 pagesA1782 v1 Alere Triage MeterPro Training ManualCésar A. PereiraNo ratings yet
- Antifungal AgentsDocument7 pagesAntifungal AgentstenawNo ratings yet
- Anti FungiDocument13 pagesAnti FungiFirdasari KarimNo ratings yet
- Definition of Antifungal DrugsDocument11 pagesDefinition of Antifungal DrugsShah ZebNo ratings yet
- 1471 2180 13 184 PDFDocument12 pages1471 2180 13 184 PDFluanadumitruNo ratings yet
- A C A D e M I C S C I e N C e SDocument11 pagesA C A D e M I C S C I e N C e SWalid EbaiedNo ratings yet
- MH BukuDocument33 pagesMH Bukunurul rezki fitrianiazisNo ratings yet
- 13 - Antibiotic III Nalidixic AcidDocument7 pages13 - Antibiotic III Nalidixic AcidMoataz TrabehNo ratings yet
- Antifungal DrugsDocument66 pagesAntifungal DrugsMalueth AnguiNo ratings yet
- Yuandani 2013Document10 pagesYuandani 2013Khrisna Whaty SilalahiNo ratings yet
- PharChm2 - TetracyclinesDocument9 pagesPharChm2 - TetracyclinesEdrick RamoranNo ratings yet
- How To Improve Antifungal StewardshipDocument12 pagesHow To Improve Antifungal StewardshipciaranNo ratings yet
- Antifungal Agents 17971Document35 pagesAntifungal Agents 17971TES SENNo ratings yet
- Synthesis and Antifilarial Evaluation of N, N - Xylofuranosylated DiaminoalkanesDocument12 pagesSynthesis and Antifilarial Evaluation of N, N - Xylofuranosylated DiaminoalkanesRumana AhmadNo ratings yet
- Abstract BenzimidazoleDocument9 pagesAbstract BenzimidazoleTeresa WrightNo ratings yet
- Pharmaceutics 13 02028Document22 pagesPharmaceutics 13 02028Magda CsávásNo ratings yet
- SK Suruj, Medicinal Chemistry III, Roll No - 38301921059, 3rd Year 6th Sem..PDF Ca2Document10 pagesSK Suruj, Medicinal Chemistry III, Roll No - 38301921059, 3rd Year 6th Sem..PDF Ca2Sk SurajNo ratings yet
- Sdavdz AdscxzDocument7 pagesSdavdz AdscxzHendra Wana Nur'aminNo ratings yet
- 956 FullDocument10 pages956 FullMuhammad IqbalNo ratings yet
- Developing Antimicrobial Compounds From Natural SourcesDocument10 pagesDeveloping Antimicrobial Compounds From Natural SourcesIvy NazeerahNo ratings yet
- Cymbopogon Nardus 4Document16 pagesCymbopogon Nardus 4wulanNo ratings yet
- Host Modulation-Promising Direction in Periodontal TherapyDocument5 pagesHost Modulation-Promising Direction in Periodontal TherapyIOSR Journal of PharmacyNo ratings yet
- Novel Antifungal Activity of Purpurin Against Candida Species in VitroDocument8 pagesNovel Antifungal Activity of Purpurin Against Candida Species in VitroEgg TelorNo ratings yet
- Plasmodium Falciparum Dihydroorotate Dehydrogenase: A Drug Target Against MalariaDocument24 pagesPlasmodium Falciparum Dihydroorotate Dehydrogenase: A Drug Target Against MalariaDelvina RahmadaniNo ratings yet
- Suppression of Nitric Oxide Production From Nasal Fibroblasts by Metabolized Clarithromycin in VitroDocument12 pagesSuppression of Nitric Oxide Production From Nasal Fibroblasts by Metabolized Clarithromycin in VitroMaria RandeNo ratings yet
- ANTIFUNGALS (Autosaved)Document72 pagesANTIFUNGALS (Autosaved)Franci Kay SichuNo ratings yet
- Biochemical Pharmacology: Joseph George TDocument9 pagesBiochemical Pharmacology: Joseph George TNiarti Ulan SariNo ratings yet
- Antifungal AgentsDocument41 pagesAntifungal AgentsSami YGNo ratings yet
- Fungal Drug OssetDocument20 pagesFungal Drug OssetSaman Kumara PereraNo ratings yet
- Flucytosi Review of PharmacologyDocument10 pagesFlucytosi Review of PharmacologyHanung PujanggaNo ratings yet
- Anti Fungal 180303181604Document51 pagesAnti Fungal 180303181604Alfredo SarachoNo ratings yet
- Fungi: Therapy of Non-Dermatophytic Mycoses in AnimalsDocument16 pagesFungi: Therapy of Non-Dermatophytic Mycoses in AnimalsDr EnéasNo ratings yet
- Antifungal AgentsDocument5 pagesAntifungal AgentsNutan Desai RaoNo ratings yet
- Ijms 23 08337 v2Document15 pagesIjms 23 08337 v2응우엔티 트랑No ratings yet
- Antifungal Drugs 3Document21 pagesAntifungal Drugs 3عبدالرحمن دودينNo ratings yet
- Bacterial and Fungal InfectionDocument9 pagesBacterial and Fungal Infectionstampjason835No ratings yet
- Antibacterial and Antifungal DrugsDocument7 pagesAntibacterial and Antifungal Drugszzb9k9w9gzNo ratings yet
- Antifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Document37 pagesAntifungal: Department of Medical Microbiology University of Maiduguri Teaching Hospital 19TH JANUARY, 2021Hafsat JimetaNo ratings yet
- 1 s2.0 S1567576913000337 MainDocument7 pages1 s2.0 S1567576913000337 MainA'in Qurrota A'yuninNo ratings yet
- Unit - 3Document39 pagesUnit - 3ujjwalNo ratings yet
- Jurnal Ipd 7Document11 pagesJurnal Ipd 7indra mendilaNo ratings yet
- Molecules 26 00005Document18 pagesMolecules 26 00005elektifppra2022No ratings yet
- Molecules 28 07705Document26 pagesMolecules 28 07705ditta23002No ratings yet
- AntifungalDocument41 pagesAntifungalDeribe BekeleNo ratings yet
- Farmakologi Anti JamurDocument13 pagesFarmakologi Anti JamurPapay MaulidyaNo ratings yet
- Anti Fungal Drugs: Dr. Jahid Assistant Professor (Unit Pharmacology) CucmsDocument70 pagesAnti Fungal Drugs: Dr. Jahid Assistant Professor (Unit Pharmacology) Cucmslailatul husnaNo ratings yet
- Antibacterial and Anti-Inflammatory Activities of 4-Hydroxycordoin: Potential Therapeutic BenefitsDocument6 pagesAntibacterial and Anti-Inflammatory Activities of 4-Hydroxycordoin: Potential Therapeutic BenefitsVinícius PiantaNo ratings yet
- Ssjcoe Manufacture of FluconazoleDocument83 pagesSsjcoe Manufacture of FluconazoleBhavik PanchalNo ratings yet
- Olymyxins A Review Focusing On Their NephrotoxicityDocument7 pagesOlymyxins A Review Focusing On Their NephrotoxicityVel MuruganNo ratings yet
- Cheng 2008Document8 pagesCheng 2008L LaaNo ratings yet
- Chat GPTDocument8 pagesChat GPTbiplob royNo ratings yet
- تحضير ثايودايازولDocument12 pagesتحضير ثايودايازولUsama AliNo ratings yet
- Van Daele 2020, Posaconazole in Prophylaxis and Treatment of IFDDocument13 pagesVan Daele 2020, Posaconazole in Prophylaxis and Treatment of IFDRodrigo GarciaNo ratings yet
- Antimicrobial Activities of Flavonoid Glycosides From Graptophyllum Grandulosum and Their Mechanism of Antibacterial ActionDocument11 pagesAntimicrobial Activities of Flavonoid Glycosides From Graptophyllum Grandulosum and Their Mechanism of Antibacterial ActionRaquel Filgueira de Souza FerreiraNo ratings yet
- 25.antifungal NigamPKDocument10 pages25.antifungal NigamPKnurulunismuhNo ratings yet
- SulfamethizoleDocument4 pagesSulfamethizoleIlva Kristiāna LangrateNo ratings yet
- Antiprotozoal Activity of α,β-Unsaturated δ-Lactones: Promising Compounds for the Development of New Therapeutic AlternativesDocument10 pagesAntiprotozoal Activity of α,β-Unsaturated δ-Lactones: Promising Compounds for the Development of New Therapeutic AlternativeserikaNo ratings yet
- IsavuconazoleDocument8 pagesIsavuconazolekhangsiean89No ratings yet
- Echinocandins: The Newest Class of Antifungals: Infectious DiseasesDocument11 pagesEchinocandins: The Newest Class of Antifungals: Infectious DiseasesdupuytrenNo ratings yet
- Use of Plant Polyphenols in Antiviral TherapeuticsFrom EverandUse of Plant Polyphenols in Antiviral TherapeuticsRating: 5 out of 5 stars5/5 (1)
- Chapter 08 - Transport in HumansDocument84 pagesChapter 08 - Transport in Humanshussaini polackNo ratings yet
- NO Hazard Slight Moderate Serious Extreme: Hazard Hazard Hazard HazardDocument74 pagesNO Hazard Slight Moderate Serious Extreme: Hazard Hazard Hazard HazardCristy Jean100% (1)
- Blood GroupingDocument30 pagesBlood GroupingDarshita SharmaNo ratings yet
- 2013 Vancomycin Do Sing GuideDocument1 page2013 Vancomycin Do Sing GuideaLPHA1No ratings yet
- PPS UPEC PIDSP Rashes in Children ModuleDocument232 pagesPPS UPEC PIDSP Rashes in Children ModuleIda Marionne ArriolaNo ratings yet
- Gram-Positive CocciDocument2 pagesGram-Positive CocciMare5Der5No ratings yet
- Anatomy and Physiology of Salivary Gland ShivaniDocument43 pagesAnatomy and Physiology of Salivary Gland ShivaniDeepika LamichhaneNo ratings yet
- Jab DetoxDocument9 pagesJab DetoxjayjonbeachNo ratings yet
- 8fc93bea-e7cb-4195-87c9-f3835becd068Document6 pages8fc93bea-e7cb-4195-87c9-f3835becd068layanhaliloNo ratings yet
- Glomerulonefrita Acuta Poststreptococica (GNAPS) - Engleza 2 (User-PC - S Conflicted Copy 2013-04-29) - 1Document37 pagesGlomerulonefrita Acuta Poststreptococica (GNAPS) - Engleza 2 (User-PC - S Conflicted Copy 2013-04-29) - 1Ashley PaulNo ratings yet
- Malassezia Furfur An-An Ap-Ap Naturally Found On The SkinDocument48 pagesMalassezia Furfur An-An Ap-Ap Naturally Found On The SkinNikki ValerioNo ratings yet
- Bacteriophages and Their Applications PDFDocument12 pagesBacteriophages and Their Applications PDFLuis AlcarazNo ratings yet
- Final Micro ModuleDocument231 pagesFinal Micro ModuleSamuel SisayNo ratings yet
- Chapter Review: True or FalseDocument2 pagesChapter Review: True or FalseJames Gabriel SalardaNo ratings yet
- ISC Class 11 Bio Specimen PaperDocument6 pagesISC Class 11 Bio Specimen PaperparamNo ratings yet
- Pglo Transformation Lab Write-UpDocument4 pagesPglo Transformation Lab Write-Upapi-314324050No ratings yet
- Seminar PPT Final Ashok P-2506Document35 pagesSeminar PPT Final Ashok P-2506Ashok ChaudharyNo ratings yet
- (Robert J. Pratt) HIV AIDS A Foundation For NurDocument481 pages(Robert J. Pratt) HIV AIDS A Foundation For NurIzzah KhoirunissaNo ratings yet
- Branches of PharmacologyDocument5 pagesBranches of Pharmacologyanon_655324688No ratings yet
- Bio411 C1Document1 pageBio411 C1Aqiena BalqisNo ratings yet
- Pediatric RhabdomyosarcomaDocument24 pagesPediatric RhabdomyosarcomaMikael AngelooNo ratings yet
- BM 8-9 OncogenesisDocument139 pagesBM 8-9 OncogenesisabdullahshiddiqadamNo ratings yet
- Tagma Khamsa PDFDocument23 pagesTagma Khamsa PDFIbad Ur RahmanNo ratings yet
- Microbiology Lab Diagnosis by ARC PDFDocument21 pagesMicrobiology Lab Diagnosis by ARC PDFZahid iqbalNo ratings yet
- POTENZA - Radiofrequency Irradiation Attenuates Angiogenesis and Infl... - I...Document20 pagesPOTENZA - Radiofrequency Irradiation Attenuates Angiogenesis and Infl... - I...TimNo ratings yet
- Thesis VirusDocument4 pagesThesis Virushan0fus1gij2100% (2)
- P N e U M o N I ADocument1 pageP N e U M o N I AchristheleNo ratings yet
- Exploring Genetic Susceptibility To Cancer in Diverse PopulationsDocument6 pagesExploring Genetic Susceptibility To Cancer in Diverse Populationskossma2006No ratings yet