
Anti Tubercular Drugs
Anti Tubercular Drugs
You might also like
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- TB RX Part 4Document30 pagesTB RX Part 4Ibrahim JeldiNo ratings yet
- Tuberculosis: Dr. Shami Pokhrel Dept. of Pediatrics, LMCDocument37 pagesTuberculosis: Dr. Shami Pokhrel Dept. of Pediatrics, LMCShami PokhrelNo ratings yet
- Pharmacotherapy of TuberculosisDocument31 pagesPharmacotherapy of TuberculosisjabirNo ratings yet
- Sem2 Anti TB DrugsDocument35 pagesSem2 Anti TB DrugsZijieNo ratings yet
- TuberculosisDocument28 pagesTuberculosisSalifyanji SimpambaNo ratings yet
- Recent TB Treatment GuidelinesDocument28 pagesRecent TB Treatment GuidelinesDr venkatesh jalluNo ratings yet
- Tuberculosis 01Document70 pagesTuberculosis 01kurutalaNo ratings yet
- TuberculosisDocument20 pagesTuberculosisaditya.3757No ratings yet
- TuberculosisDocument28 pagesTuberculosisGuilherme ReisNo ratings yet
- Tuberculosis Management Guidelines and Associated DENTAL Management GuidelinesDocument11 pagesTuberculosis Management Guidelines and Associated DENTAL Management GuidelinesAbdul AkhtarNo ratings yet
- Anti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Document27 pagesAnti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Widy StefannyNo ratings yet
- Multi-Drug-Resistant Tuberculosis (MDR-TB) Is Defined: EpidemiologyDocument3 pagesMulti-Drug-Resistant Tuberculosis (MDR-TB) Is Defined: EpidemiologyJhemar Handa JulhamidNo ratings yet
- Treatment of TuberculosisDocument19 pagesTreatment of TuberculosisMalavika A GNo ratings yet
- Rabin 2Document24 pagesRabin 2RagamNo ratings yet
- Pharmacology of Tuberculosis: Department of Pharmacology Medical Faculty Lambung Mangkurat UniversityDocument38 pagesPharmacology of Tuberculosis: Department of Pharmacology Medical Faculty Lambung Mangkurat UniversityNur HasanahNo ratings yet
- Anti-Tuberculosis DrugsDocument23 pagesAnti-Tuberculosis DrugsemmanuelmkibuniNo ratings yet
- Dots 2Document19 pagesDots 2Allum KaribasappaNo ratings yet
- SP Farmakologi TBDocument5 pagesSP Farmakologi TBvikaNo ratings yet
- Presented By: Hazel Tiam Wat-Ututalum WMSU, College of NursingDocument12 pagesPresented By: Hazel Tiam Wat-Ututalum WMSU, College of NursingYasyas Tiamwat UtutalumNo ratings yet
- MX of Paediatric TBDocument8 pagesMX of Paediatric TBAjanapakhi SahaNo ratings yet
- SP - Management of MDR-TBDocument6 pagesSP - Management of MDR-TBvikaNo ratings yet
- Treatment of TBDocument46 pagesTreatment of TBJindal Chest ClinicNo ratings yet
- MDR TB MehakDocument6 pagesMDR TB MehakKeham LeogNo ratings yet
- Anti - Tubercular DrugsDocument88 pagesAnti - Tubercular DrugsEscitalopram 5mgNo ratings yet
- Drugs Used in Tuberculosis With Recent AdvancesDocument35 pagesDrugs Used in Tuberculosis With Recent AdvancesBindira MaharjanNo ratings yet
- Upadated Management of TB: Dr. Mohammed Aqib Javed Assistatnt Registrar, MU-I SZMCHDocument47 pagesUpadated Management of TB: Dr. Mohammed Aqib Javed Assistatnt Registrar, MU-I SZMCHNusrat JahanNo ratings yet
- New Drugs and Regimens For TB: 2015 Update: Scott K. Heysell MD, MPH (No Disclosures)Document21 pagesNew Drugs and Regimens For TB: 2015 Update: Scott K. Heysell MD, MPH (No Disclosures)Nop PiromNo ratings yet
- Drug Treatment in TuberculosisDocument8 pagesDrug Treatment in TuberculosisCaren ChanNo ratings yet
- Treatment of TuberculosisDocument15 pagesTreatment of TuberculosisLabbakYaMahdiNo ratings yet
- Prevention and Management of MDR-TB in ChildrenDocument32 pagesPrevention and Management of MDR-TB in ChildrenHarpreet SinghNo ratings yet
- MDR TBDocument8 pagesMDR TBMahira Bayu AdiftaNo ratings yet
- Typhoid Fever: Divisi Tropik Dan Infeksi Bag/Smf - Ilmu Penyakit Dalam FK Unsyiah Rsud. Dr. Zainoel Abidin Banda AcehDocument23 pagesTyphoid Fever: Divisi Tropik Dan Infeksi Bag/Smf - Ilmu Penyakit Dalam FK Unsyiah Rsud. Dr. Zainoel Abidin Banda Acehandreva8No ratings yet
- TB 2Document11 pagesTB 2giant nitaNo ratings yet
- Drug Treatment of Pulmonary Tuberculosis: 4 Medical Year PharmacologyDocument30 pagesDrug Treatment of Pulmonary Tuberculosis: 4 Medical Year PharmacologyRuchi KholiyaNo ratings yet
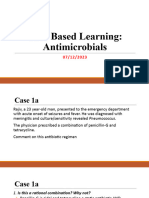
- Case Based Learning Antimicrobials 05-12-2023Document50 pagesCase Based Learning Antimicrobials 05-12-2023aditya.3757No ratings yet
- Adverse Effects of Anti Tubercular Drugs. MDR TBDocument75 pagesAdverse Effects of Anti Tubercular Drugs. MDR TBDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- 16.MDR-XDR TBDocument18 pages16.MDR-XDR TBLinna SriwaningsiNo ratings yet
- 3.0 Drug ResistanceDocument18 pages3.0 Drug ResistanceRey AlwiwikhNo ratings yet
- 3.0 Drug ResistanceDocument18 pages3.0 Drug ResistanceMohammed HammedNo ratings yet
- Pharma Uro Cotrimoxazole +fqsDocument14 pagesPharma Uro Cotrimoxazole +fqsHussein AlhaddadNo ratings yet
- Anti Tubercular & Antileprotic DrugsDocument99 pagesAnti Tubercular & Antileprotic DrugsHrishikesh NachinolkarNo ratings yet
- Management of DR-TB: PMDT GuidelineDocument41 pagesManagement of DR-TB: PMDT GuidelineSomnath Das GuptaNo ratings yet
- NTP MOP 6th Ed Module 7 Treatment of TB in Special Situations 10.20.20Document56 pagesNTP MOP 6th Ed Module 7 Treatment of TB in Special Situations 10.20.20gbNo ratings yet
- Anti-Tubercular DrugsDocument76 pagesAnti-Tubercular DrugsGeneral InquiriesNo ratings yet
- TB Hiv CoinfectionDocument29 pagesTB Hiv CoinfectionVinobhachowdary DondapatiNo ratings yet
- In The Management Of: Dr. Soji Ige FWACPDocument22 pagesIn The Management Of: Dr. Soji Ige FWACPFemi AustinNo ratings yet
- Diagnosis and Treatment of Drug-Resistant Tuberculosis-Hermanto QuedarusmanDocument20 pagesDiagnosis and Treatment of Drug-Resistant Tuberculosis-Hermanto QuedarusmanHermanto QuedarusmanNo ratings yet
- Dots 150320013145 Conversion Gate01Document25 pagesDots 150320013145 Conversion Gate01only and only pubg GAMEPLAYNo ratings yet
- MDR TB Made EasyDocument58 pagesMDR TB Made EasyNezly IderusNo ratings yet
- 3.0 Drug ResistanceDocument18 pages3.0 Drug ResistanceMeenachi ChidambaramNo ratings yet
- Tuberculosis 022007 HartDocument68 pagesTuberculosis 022007 HartWildan HumairahNo ratings yet
- Rntcp-Revised National Tuberculosis Control ProgrammeDocument29 pagesRntcp-Revised National Tuberculosis Control ProgrammedranshulitrivediNo ratings yet
- Public Health Aspects of TBDocument53 pagesPublic Health Aspects of TBmaskericon ChivesNo ratings yet
- Developments in The Diagnosis & Management of PTBDocument50 pagesDevelopments in The Diagnosis & Management of PTBadamu mohammadNo ratings yet
- Antimicrobial Therapy in Sepsis PDFDocument38 pagesAntimicrobial Therapy in Sepsis PDFTatik HandayaniNo ratings yet
- Treatment of TB in Adults: by Dr. Irfhan Ali Hyder AliDocument45 pagesTreatment of TB in Adults: by Dr. Irfhan Ali Hyder AliInspireGutsNo ratings yet
- DotsDocument5 pagesDotsYusephAwangSanaaniNo ratings yet
- A Statistical Inquiry Into the Nature and Treatment of EpilepsyFrom EverandA Statistical Inquiry Into the Nature and Treatment of EpilepsyNo ratings yet
- Operasi Dakriosistorhinostomi DCR Pada Pasien Dengan Dakriosistitis Kronis - Novaqua YandiDocument13 pagesOperasi Dakriosistorhinostomi DCR Pada Pasien Dengan Dakriosistitis Kronis - Novaqua YandiIDI Bangka BaratNo ratings yet
- 6 Best Homeopathic Medicines For KeloidsDocument3 pages6 Best Homeopathic Medicines For KeloidssuganNo ratings yet
- Pattern Classification in Kampo Medicine: ArticleDocument6 pagesPattern Classification in Kampo Medicine: ArticlehipkunNo ratings yet
- Significances of The Study-Definition of TermsDocument4 pagesSignificances of The Study-Definition of TermsYannah HidalgoNo ratings yet
- What Is DehydrationDocument7 pagesWhat Is DehydrationMarwan WijayaNo ratings yet
- Nurse Patient Nurse: Tugas Sir Jon. Admission Patient DialogueDocument7 pagesNurse Patient Nurse: Tugas Sir Jon. Admission Patient DialogueIndry LabungasaNo ratings yet
- Nursing ExamsDocument5 pagesNursing ExamsPedialy AvilesNo ratings yet
- Differences Between Men and Women BrainDocument1 pageDifferences Between Men and Women BrainHuiLingNo ratings yet
- 1116005I Rev. 02Document2 pages1116005I Rev. 02kirubel demelashNo ratings yet
- Eslit-Vinea-LA 03 Task #1-4Document11 pagesEslit-Vinea-LA 03 Task #1-4darkNo ratings yet
- RenalDocument60 pagesRenalEdmalyn Dela CruzNo ratings yet
- Papa Reports 04-04-2022Document6 pagesPapa Reports 04-04-2022Anish goyalNo ratings yet
- Human Virus Families and Their DiseasesDocument1 pageHuman Virus Families and Their DiseasesKate EvangelistaNo ratings yet
- CHN Lec ReviewerDocument26 pagesCHN Lec ReviewerShekinah PuntilarNo ratings yet
- Philippine Adult Immunization Recommendation 2017 PDFDocument2 pagesPhilippine Adult Immunization Recommendation 2017 PDFLinius CruzNo ratings yet
- JMSCR Vol - 07 - Issue - 08 - Page 294-297 - August: Use of Polyetylene Glycolenema in Patients On Hemodialysis PatientsDocument4 pagesJMSCR Vol - 07 - Issue - 08 - Page 294-297 - August: Use of Polyetylene Glycolenema in Patients On Hemodialysis PatientsJaydeep VayedaNo ratings yet
- Education For Physically Challenged Children Set 1Document6 pagesEducation For Physically Challenged Children Set 1Ahmed KhanNo ratings yet
- COVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologyDocument10 pagesCOVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologydrToikNo ratings yet
- AcuPulse Versatility SupplementDocument16 pagesAcuPulse Versatility SupplementSD DSNo ratings yet
- Posterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentDocument8 pagesPosterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentNegru TeodorNo ratings yet
- PotakaDocument6 pagesPotakaTrisha Olila CasimeroNo ratings yet
- Sialolithiasis - A Report of Two Cases and ReviewDocument4 pagesSialolithiasis - A Report of Two Cases and Reviewmaharani spNo ratings yet
- Management of Low Birth Weight BabiesDocument59 pagesManagement of Low Birth Weight BabiesKiran Khasa100% (2)
- Thyrocare Test Price ListDocument2 pagesThyrocare Test Price ListRoyal MarathaNo ratings yet
- ClaspDocument4 pagesClaspRebin AliNo ratings yet
- List of Members of Person's With Disability - Gulod (APWD-Gulod) Barangay Gulod, District 5, Quezon CityDocument33 pagesList of Members of Person's With Disability - Gulod (APWD-Gulod) Barangay Gulod, District 5, Quezon CityJurryNo ratings yet
- First Regular Session: Senate S. NoDocument13 pagesFirst Regular Session: Senate S. NoJSTNo ratings yet
- Molecular Laboratory ReportDocument1 pageMolecular Laboratory ReportCristina TorresNo ratings yet
- Minscat Bongabong Campus, To Be Placed On 'Localized Lockdown' Due To Coronavirus ThreatDocument5 pagesMinscat Bongabong Campus, To Be Placed On 'Localized Lockdown' Due To Coronavirus ThreatFranz Chavez GarciaNo ratings yet
- Sci10 Quarter 3 Module 5 NO ANSWER KEYDocument33 pagesSci10 Quarter 3 Module 5 NO ANSWER KEYNiña Miles TabañagNo ratings yet
























































































Download as pdf or txt
You might also like
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- TB RX Part 4Document30 pagesTB RX Part 4Ibrahim JeldiNo ratings yet
- Tuberculosis: Dr. Shami Pokhrel Dept. of Pediatrics, LMCDocument37 pagesTuberculosis: Dr. Shami Pokhrel Dept. of Pediatrics, LMCShami PokhrelNo ratings yet
- Pharmacotherapy of TuberculosisDocument31 pagesPharmacotherapy of TuberculosisjabirNo ratings yet
- Sem2 Anti TB DrugsDocument35 pagesSem2 Anti TB DrugsZijieNo ratings yet
- TuberculosisDocument28 pagesTuberculosisSalifyanji SimpambaNo ratings yet
- Recent TB Treatment GuidelinesDocument28 pagesRecent TB Treatment GuidelinesDr venkatesh jalluNo ratings yet
- Tuberculosis 01Document70 pagesTuberculosis 01kurutalaNo ratings yet
- TuberculosisDocument20 pagesTuberculosisaditya.3757No ratings yet
- TuberculosisDocument28 pagesTuberculosisGuilherme ReisNo ratings yet
- Tuberculosis Management Guidelines and Associated DENTAL Management GuidelinesDocument11 pagesTuberculosis Management Guidelines and Associated DENTAL Management GuidelinesAbdul AkhtarNo ratings yet
- Anti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Document27 pagesAnti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Widy StefannyNo ratings yet
- Multi-Drug-Resistant Tuberculosis (MDR-TB) Is Defined: EpidemiologyDocument3 pagesMulti-Drug-Resistant Tuberculosis (MDR-TB) Is Defined: EpidemiologyJhemar Handa JulhamidNo ratings yet
- Treatment of TuberculosisDocument19 pagesTreatment of TuberculosisMalavika A GNo ratings yet
- Rabin 2Document24 pagesRabin 2RagamNo ratings yet
- Pharmacology of Tuberculosis: Department of Pharmacology Medical Faculty Lambung Mangkurat UniversityDocument38 pagesPharmacology of Tuberculosis: Department of Pharmacology Medical Faculty Lambung Mangkurat UniversityNur HasanahNo ratings yet
- Anti-Tuberculosis DrugsDocument23 pagesAnti-Tuberculosis DrugsemmanuelmkibuniNo ratings yet
- Dots 2Document19 pagesDots 2Allum KaribasappaNo ratings yet
- SP Farmakologi TBDocument5 pagesSP Farmakologi TBvikaNo ratings yet
- Presented By: Hazel Tiam Wat-Ututalum WMSU, College of NursingDocument12 pagesPresented By: Hazel Tiam Wat-Ututalum WMSU, College of NursingYasyas Tiamwat UtutalumNo ratings yet
- MX of Paediatric TBDocument8 pagesMX of Paediatric TBAjanapakhi SahaNo ratings yet
- SP - Management of MDR-TBDocument6 pagesSP - Management of MDR-TBvikaNo ratings yet
- Treatment of TBDocument46 pagesTreatment of TBJindal Chest ClinicNo ratings yet
- MDR TB MehakDocument6 pagesMDR TB MehakKeham LeogNo ratings yet
- Anti - Tubercular DrugsDocument88 pagesAnti - Tubercular DrugsEscitalopram 5mgNo ratings yet
- Drugs Used in Tuberculosis With Recent AdvancesDocument35 pagesDrugs Used in Tuberculosis With Recent AdvancesBindira MaharjanNo ratings yet
- Upadated Management of TB: Dr. Mohammed Aqib Javed Assistatnt Registrar, MU-I SZMCHDocument47 pagesUpadated Management of TB: Dr. Mohammed Aqib Javed Assistatnt Registrar, MU-I SZMCHNusrat JahanNo ratings yet
- New Drugs and Regimens For TB: 2015 Update: Scott K. Heysell MD, MPH (No Disclosures)Document21 pagesNew Drugs and Regimens For TB: 2015 Update: Scott K. Heysell MD, MPH (No Disclosures)Nop PiromNo ratings yet
- Drug Treatment in TuberculosisDocument8 pagesDrug Treatment in TuberculosisCaren ChanNo ratings yet
- Treatment of TuberculosisDocument15 pagesTreatment of TuberculosisLabbakYaMahdiNo ratings yet
- Prevention and Management of MDR-TB in ChildrenDocument32 pagesPrevention and Management of MDR-TB in ChildrenHarpreet SinghNo ratings yet
- MDR TBDocument8 pagesMDR TBMahira Bayu AdiftaNo ratings yet
- Typhoid Fever: Divisi Tropik Dan Infeksi Bag/Smf - Ilmu Penyakit Dalam FK Unsyiah Rsud. Dr. Zainoel Abidin Banda AcehDocument23 pagesTyphoid Fever: Divisi Tropik Dan Infeksi Bag/Smf - Ilmu Penyakit Dalam FK Unsyiah Rsud. Dr. Zainoel Abidin Banda Acehandreva8No ratings yet
- TB 2Document11 pagesTB 2giant nitaNo ratings yet
- Drug Treatment of Pulmonary Tuberculosis: 4 Medical Year PharmacologyDocument30 pagesDrug Treatment of Pulmonary Tuberculosis: 4 Medical Year PharmacologyRuchi KholiyaNo ratings yet
- Case Based Learning Antimicrobials 05-12-2023Document50 pagesCase Based Learning Antimicrobials 05-12-2023aditya.3757No ratings yet
- Adverse Effects of Anti Tubercular Drugs. MDR TBDocument75 pagesAdverse Effects of Anti Tubercular Drugs. MDR TBDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- 16.MDR-XDR TBDocument18 pages16.MDR-XDR TBLinna SriwaningsiNo ratings yet
- 3.0 Drug ResistanceDocument18 pages3.0 Drug ResistanceRey AlwiwikhNo ratings yet
- 3.0 Drug ResistanceDocument18 pages3.0 Drug ResistanceMohammed HammedNo ratings yet
- Pharma Uro Cotrimoxazole +fqsDocument14 pagesPharma Uro Cotrimoxazole +fqsHussein AlhaddadNo ratings yet
- Anti Tubercular & Antileprotic DrugsDocument99 pagesAnti Tubercular & Antileprotic DrugsHrishikesh NachinolkarNo ratings yet
- Management of DR-TB: PMDT GuidelineDocument41 pagesManagement of DR-TB: PMDT GuidelineSomnath Das GuptaNo ratings yet
- NTP MOP 6th Ed Module 7 Treatment of TB in Special Situations 10.20.20Document56 pagesNTP MOP 6th Ed Module 7 Treatment of TB in Special Situations 10.20.20gbNo ratings yet
- Anti-Tubercular DrugsDocument76 pagesAnti-Tubercular DrugsGeneral InquiriesNo ratings yet
- TB Hiv CoinfectionDocument29 pagesTB Hiv CoinfectionVinobhachowdary DondapatiNo ratings yet
- In The Management Of: Dr. Soji Ige FWACPDocument22 pagesIn The Management Of: Dr. Soji Ige FWACPFemi AustinNo ratings yet
- Diagnosis and Treatment of Drug-Resistant Tuberculosis-Hermanto QuedarusmanDocument20 pagesDiagnosis and Treatment of Drug-Resistant Tuberculosis-Hermanto QuedarusmanHermanto QuedarusmanNo ratings yet
- Dots 150320013145 Conversion Gate01Document25 pagesDots 150320013145 Conversion Gate01only and only pubg GAMEPLAYNo ratings yet
- MDR TB Made EasyDocument58 pagesMDR TB Made EasyNezly IderusNo ratings yet
- 3.0 Drug ResistanceDocument18 pages3.0 Drug ResistanceMeenachi ChidambaramNo ratings yet
- Tuberculosis 022007 HartDocument68 pagesTuberculosis 022007 HartWildan HumairahNo ratings yet
- Rntcp-Revised National Tuberculosis Control ProgrammeDocument29 pagesRntcp-Revised National Tuberculosis Control ProgrammedranshulitrivediNo ratings yet
- Public Health Aspects of TBDocument53 pagesPublic Health Aspects of TBmaskericon ChivesNo ratings yet
- Developments in The Diagnosis & Management of PTBDocument50 pagesDevelopments in The Diagnosis & Management of PTBadamu mohammadNo ratings yet
- Antimicrobial Therapy in Sepsis PDFDocument38 pagesAntimicrobial Therapy in Sepsis PDFTatik HandayaniNo ratings yet
- Treatment of TB in Adults: by Dr. Irfhan Ali Hyder AliDocument45 pagesTreatment of TB in Adults: by Dr. Irfhan Ali Hyder AliInspireGutsNo ratings yet
- DotsDocument5 pagesDotsYusephAwangSanaaniNo ratings yet
- A Statistical Inquiry Into the Nature and Treatment of EpilepsyFrom EverandA Statistical Inquiry Into the Nature and Treatment of EpilepsyNo ratings yet
- Operasi Dakriosistorhinostomi DCR Pada Pasien Dengan Dakriosistitis Kronis - Novaqua YandiDocument13 pagesOperasi Dakriosistorhinostomi DCR Pada Pasien Dengan Dakriosistitis Kronis - Novaqua YandiIDI Bangka BaratNo ratings yet
- 6 Best Homeopathic Medicines For KeloidsDocument3 pages6 Best Homeopathic Medicines For KeloidssuganNo ratings yet
- Pattern Classification in Kampo Medicine: ArticleDocument6 pagesPattern Classification in Kampo Medicine: ArticlehipkunNo ratings yet
- Significances of The Study-Definition of TermsDocument4 pagesSignificances of The Study-Definition of TermsYannah HidalgoNo ratings yet
- What Is DehydrationDocument7 pagesWhat Is DehydrationMarwan WijayaNo ratings yet
- Nurse Patient Nurse: Tugas Sir Jon. Admission Patient DialogueDocument7 pagesNurse Patient Nurse: Tugas Sir Jon. Admission Patient DialogueIndry LabungasaNo ratings yet
- Nursing ExamsDocument5 pagesNursing ExamsPedialy AvilesNo ratings yet
- Differences Between Men and Women BrainDocument1 pageDifferences Between Men and Women BrainHuiLingNo ratings yet
- 1116005I Rev. 02Document2 pages1116005I Rev. 02kirubel demelashNo ratings yet
- Eslit-Vinea-LA 03 Task #1-4Document11 pagesEslit-Vinea-LA 03 Task #1-4darkNo ratings yet
- RenalDocument60 pagesRenalEdmalyn Dela CruzNo ratings yet
- Papa Reports 04-04-2022Document6 pagesPapa Reports 04-04-2022Anish goyalNo ratings yet
- Human Virus Families and Their DiseasesDocument1 pageHuman Virus Families and Their DiseasesKate EvangelistaNo ratings yet
- CHN Lec ReviewerDocument26 pagesCHN Lec ReviewerShekinah PuntilarNo ratings yet
- Philippine Adult Immunization Recommendation 2017 PDFDocument2 pagesPhilippine Adult Immunization Recommendation 2017 PDFLinius CruzNo ratings yet
- JMSCR Vol - 07 - Issue - 08 - Page 294-297 - August: Use of Polyetylene Glycolenema in Patients On Hemodialysis PatientsDocument4 pagesJMSCR Vol - 07 - Issue - 08 - Page 294-297 - August: Use of Polyetylene Glycolenema in Patients On Hemodialysis PatientsJaydeep VayedaNo ratings yet
- Education For Physically Challenged Children Set 1Document6 pagesEducation For Physically Challenged Children Set 1Ahmed KhanNo ratings yet
- COVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologyDocument10 pagesCOVID-19 Vaccine in Patients With Haematological Disorders British Society For HaematologydrToikNo ratings yet
- AcuPulse Versatility SupplementDocument16 pagesAcuPulse Versatility SupplementSD DSNo ratings yet
- Posterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentDocument8 pagesPosterior Tibial Tendon Dysfunction - What Does The Single Heel Raise Test Mean in AssessmentNegru TeodorNo ratings yet
- PotakaDocument6 pagesPotakaTrisha Olila CasimeroNo ratings yet
- Sialolithiasis - A Report of Two Cases and ReviewDocument4 pagesSialolithiasis - A Report of Two Cases and Reviewmaharani spNo ratings yet
- Management of Low Birth Weight BabiesDocument59 pagesManagement of Low Birth Weight BabiesKiran Khasa100% (2)
- Thyrocare Test Price ListDocument2 pagesThyrocare Test Price ListRoyal MarathaNo ratings yet
- ClaspDocument4 pagesClaspRebin AliNo ratings yet
- List of Members of Person's With Disability - Gulod (APWD-Gulod) Barangay Gulod, District 5, Quezon CityDocument33 pagesList of Members of Person's With Disability - Gulod (APWD-Gulod) Barangay Gulod, District 5, Quezon CityJurryNo ratings yet
- First Regular Session: Senate S. NoDocument13 pagesFirst Regular Session: Senate S. NoJSTNo ratings yet
- Molecular Laboratory ReportDocument1 pageMolecular Laboratory ReportCristina TorresNo ratings yet
- Minscat Bongabong Campus, To Be Placed On 'Localized Lockdown' Due To Coronavirus ThreatDocument5 pagesMinscat Bongabong Campus, To Be Placed On 'Localized Lockdown' Due To Coronavirus ThreatFranz Chavez GarciaNo ratings yet
- Sci10 Quarter 3 Module 5 NO ANSWER KEYDocument33 pagesSci10 Quarter 3 Module 5 NO ANSWER KEYNiña Miles TabañagNo ratings yet