Download as pdf or txt
You might also like
- Astm E337 15Document24 pagesAstm E337 15Yeferson Fabian Rico Osma100% (1)
- AJMP 32 7 13 Final PDFDocument7 pagesAJMP 32 7 13 Final PDFHaythem AbidiNo ratings yet
- Brachytherapy Systems, Remote AfterloadingDocument24 pagesBrachytherapy Systems, Remote Afterloadingtuffaha1333No ratings yet
- Dosimetry in Brachytherapy – An International Code of Practice for Secondary Standards Dosimetry Laboratories and HospitalsFrom EverandDosimetry in Brachytherapy – An International Code of Practice for Secondary Standards Dosimetry Laboratories and HospitalsNo ratings yet
- Filme EBT3 Usando Fonte Ir-192 HDR 2022Document14 pagesFilme EBT3 Usando Fonte Ir-192 HDR 2022Andreyson SilvaNo ratings yet
- Image Quality Standards For Digital Imaging and Interventional RadiologyDocument8 pagesImage Quality Standards For Digital Imaging and Interventional RadiologyAnonymous 2gLSPeNo ratings yet
- MP 14540Document48 pagesMP 14540Andreyson SilvaNo ratings yet
- Palmer 20131Document8 pagesPalmer 20131Andreyson SilvaNo ratings yet
- IJRR v12n3p265 enDocument7 pagesIJRR v12n3p265 enÔmar Vega CNo ratings yet
- Guidelines For The Calibration of Dosimeters For Use in Radiation ProcessingDocument19 pagesGuidelines For The Calibration of Dosimeters For Use in Radiation ProcessingMuhammad ZanuarNo ratings yet
- Room Design Study To Convert Ir192 To Co60 in HDR BrachyDocument6 pagesRoom Design Study To Convert Ir192 To Co60 in HDR BrachySurya SuganthanNo ratings yet
- Template For Radium-223 Dosimetry: AuthorsDocument7 pagesTemplate For Radium-223 Dosimetry: AuthorsarifpharmjuNo ratings yet
- Cobalt 60 VS Iridium 192Document6 pagesCobalt 60 VS Iridium 192Rares PNo ratings yet
- 41 JMSCRDocument8 pages41 JMSCRvamsi NathNo ratings yet
- Ir 192 Vs Co 60Document6 pagesIr 192 Vs Co 60Rin FemboyNo ratings yet
- J Applied Clin Med Phys - 2022 - Anetai - Assessment of Using A Gamma Index Analysis For Patient Specific Quality AssuranceDocument16 pagesJ Applied Clin Med Phys - 2022 - Anetai - Assessment of Using A Gamma Index Analysis For Patient Specific Quality AssuranceJosep GamarraNo ratings yet
- BIIJ - HDR Brachytherapy QADocument7 pagesBIIJ - HDR Brachytherapy QAClaudia Morales UlloaNo ratings yet
- PALMER2013Document19 pagesPALMER2013Andreyson SilvaNo ratings yet
- Measurement Validation and Uncertainty of An ExperDocument17 pagesMeasurement Validation and Uncertainty of An ExperRONALD ALFONSO PACHECO TORRESNo ratings yet
- Instant MicroDocument24 pagesInstant MicrojcintpaNo ratings yet
- GSMA International EMF Exposure Guideline Oct21Document36 pagesGSMA International EMF Exposure Guideline Oct21Saief AhmadNo ratings yet
- Clinical Efficacy of An Electronic Portal Imaging Device Versus A Physical PhantomDocument12 pagesClinical Efficacy of An Electronic Portal Imaging Device Versus A Physical Phantomxiwevi4103No ratings yet
- Khairi Salem v2Document14 pagesKhairi Salem v2Padmitha KrishnakumarNo ratings yet
- SFDA Requirement For DEXADocument9 pagesSFDA Requirement For DEXAEhsan alwafaaNo ratings yet
- TRS457 WebDocument372 pagesTRS457 WebramdhandadanNo ratings yet
- Hospital BDocument4 pagesHospital Bwovefiv466No ratings yet
- Jurnal Internasional Aso PDFDocument8 pagesJurnal Internasional Aso PDFAffrilinaNo ratings yet
- Applications of Ionzing RadiationDocument15 pagesApplications of Ionzing RadiationSuper CellNo ratings yet
- Polymers 13 01815Document13 pagesPolymers 13 01815Amor BchetniaNo ratings yet
- Draft Guidelines For RadiopharmacyDocument14 pagesDraft Guidelines For RadiopharmacyRomildo da SilvaNo ratings yet
- 2021 - Li - A Fast Determination of Insecticide Deltamethrin by Spectral Data FusionDocument8 pages2021 - Li - A Fast Determination of Insecticide Deltamethrin by Spectral Data FusionvaleriapbNo ratings yet
- Applsci 11 09749 v2Document10 pagesApplsci 11 09749 v2Angelina ProtikNo ratings yet
- ESM Andersen BrochureDocument12 pagesESM Andersen BrochureGezgin BiriNo ratings yet
- Astm D6348 12 2020 FT IrDocument7 pagesAstm D6348 12 2020 FT IrPRADEEP NAIRNo ratings yet
- Efficacy of Famotidine For COVID-19: A Systematic Review and Meta-AnalysisDocument18 pagesEfficacy of Famotidine For COVID-19: A Systematic Review and Meta-AnalysisSahat Halim BudimanNo ratings yet
- BulganDocument10 pagesBulganIkh nahia Ikh Nakhia PharmNo ratings yet
- RadiometerDocument3 pagesRadiometeromaimaessaad.belhajNo ratings yet
- Trophon 2 Probe Disinfection InnovationDocument3 pagesTrophon 2 Probe Disinfection Innovationultrasounds.salesNo ratings yet
- J Applied Clin Med Phys - 2020 - Mehrens - Survey Results of 3D CRT and IMRT Quality Assurance PracticeDocument7 pagesJ Applied Clin Med Phys - 2020 - Mehrens - Survey Results of 3D CRT and IMRT Quality Assurance Practicephutycharm15No ratings yet
- Specification and Acceptance Testing of Radiotherapy Treatment Planning SystemsDocument68 pagesSpecification and Acceptance Testing of Radiotherapy Treatment Planning Systemsjiar001No ratings yet
- Á1119Ñ Near-Infrared Spectroscopy: Calibration of Temperature-And Humidity-Monitoring DevicesDocument8 pagesÁ1119Ñ Near-Infrared Spectroscopy: Calibration of Temperature-And Humidity-Monitoring DeviceselenitabastosNo ratings yet
- Dose Evaluation For Skin and Organ in HepatocellulDocument11 pagesDose Evaluation For Skin and Organ in HepatocellulAnne MbrkNo ratings yet
- Optical Sensing Techniques For Quality Control of CathetersDocument4 pagesOptical Sensing Techniques For Quality Control of CathetersGleice GermanoNo ratings yet
- Artigo PALMER2012Document16 pagesArtigo PALMER2012Andreyson SilvaNo ratings yet
- Qa AssuranceDocument6 pagesQa AssuranceSari BustillosNo ratings yet
- Environment Monitoring, Result Evaluation and Common Contaminants Study of Vaccine Manufacturing FacilityDocument12 pagesEnvironment Monitoring, Result Evaluation and Common Contaminants Study of Vaccine Manufacturing FacilityIJRASETPublicationsNo ratings yet
- Paperof PermethrinDocument5 pagesPaperof PermethrinRavi AbdillahNo ratings yet
- Foss 01 WP 1712 NirDocument4 pagesFoss 01 WP 1712 NirffmbdrngNo ratings yet
- Commissioning of Brachytherapy ApplicatorDocument17 pagesCommissioning of Brachytherapy ApplicatorMourya AnkurNo ratings yet
- Oeh Airborne FibreDocument61 pagesOeh Airborne Fibregeorge robertsNo ratings yet
- Medical-Grade Ultra-High Molecular Weight Polyethylene YarnsDocument4 pagesMedical-Grade Ultra-High Molecular Weight Polyethylene YarnsJoãoNo ratings yet
- 1 s2.0 S0026265X22006816 MainDocument8 pages1 s2.0 S0026265X22006816 MainBruno LuccaNo ratings yet
- Futuristic BackgroundDocument8 pagesFuturistic Backgroundumeshchandra24276No ratings yet
- Uso de RadiaçãoDocument6 pagesUso de RadiaçãoPedralhadaNo ratings yet
- Coronary Angiography and Percutaneous Transluminal Coronary Angiop - 2010 - PhysDocument9 pagesCoronary Angiography and Percutaneous Transluminal Coronary Angiop - 2010 - PhysAnne MbrkNo ratings yet
- Technical Report, 1997Document21 pagesTechnical Report, 1997samsonNo ratings yet
- Moisture Content Determination of Pharmaceutical Pellets by Near Infrared Spectroscopy: Method Development and ValidationDocument7 pagesMoisture Content Determination of Pharmaceutical Pellets by Near Infrared Spectroscopy: Method Development and ValidationMariana Vazquez CerritosNo ratings yet
- Implementation of a Remote and Automated Quality Control Programme for Radiography and Mammography EquipmentFrom EverandImplementation of a Remote and Automated Quality Control Programme for Radiography and Mammography EquipmentNo ratings yet
- IMRT Optimization Algorithms: David Shepard Swedish Cancer Institute Seattle, WADocument191 pagesIMRT Optimization Algorithms: David Shepard Swedish Cancer Institute Seattle, WAAndreyson SilvaNo ratings yet
- MP 14540Document48 pagesMP 14540Andreyson SilvaNo ratings yet
- Palmer 20131Document8 pagesPalmer 20131Andreyson SilvaNo ratings yet
- PALMER2013Document19 pagesPALMER2013Andreyson SilvaNo ratings yet
- Achy 2015 02 192Document8 pagesAchy 2015 02 192Andreyson SilvaNo ratings yet
- Filme EBT3 Usando Fonte Ir-192 HDR 2022Document14 pagesFilme EBT3 Usando Fonte Ir-192 HDR 2022Andreyson SilvaNo ratings yet
- Estro AcropDocument12 pagesEstro AcropAndreyson SilvaNo ratings yet
- Filtro Dinâmico 2020Document12 pagesFiltro Dinâmico 2020Andreyson SilvaNo ratings yet
- Wave Optics MCQDocument8 pagesWave Optics MCQGuru ki physicsNo ratings yet
- Characteristics of A Solar Cell (Mp1) : Laboratory Course II. Group BA-C-09Document25 pagesCharacteristics of A Solar Cell (Mp1) : Laboratory Course II. Group BA-C-09carmensanpeNo ratings yet
- Topic 3 DM025 202021Document16 pagesTopic 3 DM025 202021Daeyanna SamsudinNo ratings yet
- Question Paper - (Electrical) : Maximum Marks: 50 Time Allowed: 1 HourDocument6 pagesQuestion Paper - (Electrical) : Maximum Marks: 50 Time Allowed: 1 Hourbikas_sahaNo ratings yet
- DCW - Zoomlion Technical Specs of 8M3 Truck Mixer PDFDocument11 pagesDCW - Zoomlion Technical Specs of 8M3 Truck Mixer PDFjacques PerronNo ratings yet
- CS301 Midterm Solved Mega File With ReferenceDocument30 pagesCS301 Midterm Solved Mega File With ReferenceZohaib GNo ratings yet
- Battery Charger SizingDocument1 pageBattery Charger SizingSenthil RajanNo ratings yet
- Analyses For Multi-Site Experiments Using Augmented Designs: Hij HijDocument2 pagesAnalyses For Multi-Site Experiments Using Augmented Designs: Hij HijMustakiMipa RegresiNo ratings yet
- Periodicity Review SL KeyDocument4 pagesPeriodicity Review SL KeyYeyoung ParkNo ratings yet
- Department of Education: Teacher's Weekly Instructional Learning Plan For Modular Distance LearningDocument2 pagesDepartment of Education: Teacher's Weekly Instructional Learning Plan For Modular Distance LearningMark Paul AlvarezNo ratings yet
- ClosTron 2Document3 pagesClosTron 2Sakir ApexNo ratings yet
- TFP3051 Demo SpecSheetDocument2 pagesTFP3051 Demo SpecSheetAlexandr KorolevNo ratings yet
- Haptics Seminar ReportDocument38 pagesHaptics Seminar Reportmonty083No ratings yet
- CAT Questions On CubesDocument4 pagesCAT Questions On CubesRanjith DNo ratings yet
- CHP 11 Part 2Document24 pagesCHP 11 Part 2Valarmathi SaravananNo ratings yet
- Agricola - CatalogoDocument217 pagesAgricola - CatalogoUnodostres Cinco Ocho Trece100% (1)
- UNIT 3 GRAPHS Class NotesDocument24 pagesUNIT 3 GRAPHS Class NotesSUDHA SNo ratings yet
- ChatGPT What Do Know About TelepathyDocument6 pagesChatGPT What Do Know About TelepathyBruce WilliamsNo ratings yet
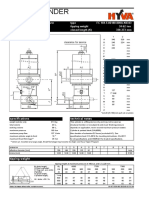
- Hyva CylinderDocument2 pagesHyva CylinderDinifaanNo ratings yet
- STH Poster Winter 2013Document2 pagesSTH Poster Winter 2013SakuragiNo ratings yet
- Nail Making Machine 20-21Document8 pagesNail Making Machine 20-21parhamadkNo ratings yet
- Testmaster 10Document8 pagesTestmaster 10Đức ĐạtNo ratings yet
- General Chemistry 1: Learner'S Packet inDocument13 pagesGeneral Chemistry 1: Learner'S Packet inAbcd ReyesNo ratings yet
- Work Energy Chapter Problems-2009-05-13Document21 pagesWork Energy Chapter Problems-2009-05-13Liam ReillyNo ratings yet
- Integrity Management With S-RBI: Using The w-IMS ToolDocument28 pagesIntegrity Management With S-RBI: Using The w-IMS ToolHari ShNo ratings yet
- Impact of Occupant Autonomy On Satisfaction and Building Energy EffciencyDocument9 pagesImpact of Occupant Autonomy On Satisfaction and Building Energy EffciencyAngelica ElboNo ratings yet
- Arista Precision Data Analysis With DANZ WhitePaperDocument11 pagesArista Precision Data Analysis With DANZ WhitePaperZekNo ratings yet
- P P P P: Duplex 2205 Specifications: UNS S32205/S31803Document2 pagesP P P P: Duplex 2205 Specifications: UNS S32205/S31803Bagus AdiriantoNo ratings yet
- Unit 2.4 Software Requirement SpecificationDocument15 pagesUnit 2.4 Software Requirement SpecificationJolly KumarNo ratings yet
- 400 Series: Industrial 23.6 KW / 31.6 HP at 2400 RPM 26.1 KW / 35.0 HP at 2600 RPMDocument5 pages400 Series: Industrial 23.6 KW / 31.6 HP at 2400 RPM 26.1 KW / 35.0 HP at 2600 RPMMouh ElobeyNo ratings yet