Download as pdf or txt
You might also like
- Pop Up The Art of Dimensional Moving Paper Designs 4Document20 pagesPop Up The Art of Dimensional Moving Paper Designs 4Rodrigo L. B.100% (1)
- 27 - Pajonk2010Document11 pages27 - Pajonk2010Sergio Machado NeurocientistaNo ratings yet
- Short Communication: J Rehabil Med 47Document4 pagesShort Communication: J Rehabil Med 47iltaNo ratings yet
- 30 Kimhy2015Document10 pages30 Kimhy2015Sergio Machado NeurocientistaNo ratings yet
- 7 Lin2016Document2 pages7 Lin2016Sergio Machado NeurocientistaNo ratings yet
- 4Document4 pages4Amr Mohamed GalalNo ratings yet
- 2 - Papiol2017Document9 pages2 - Papiol2017Sergio Machado NeurocientistaNo ratings yet
- Exercise and OpioidsDocument10 pagesExercise and OpioidsCatalina Vallejos PaillaoNo ratings yet
- Jurnal BekamDocument8 pagesJurnal BekamAprilia nur ainiNo ratings yet
- 18 Kimhy2016Document3 pages18 Kimhy2016Sergio Machado NeurocientistaNo ratings yet
- 1 s2.0 S0014299916304800 MainDocument10 pages1 s2.0 S0014299916304800 MainlypemenosdiogenesNo ratings yet
- Jurnal EbpDocument11 pagesJurnal Ebpega youngNo ratings yet
- Determining The Effectiveness of Salavat in Reduction of Anxiety With The Mediation of Neurofeedback DeviceDocument3 pagesDetermining The Effectiveness of Salavat in Reduction of Anxiety With The Mediation of Neurofeedback Deviceelyaz bornakNo ratings yet
- Intense Exercise Increases Circulating Endocannabinoid and BDNF Levels in Humans - Possible Implications For Reward and DepressionDocument8 pagesIntense Exercise Increases Circulating Endocannabinoid and BDNF Levels in Humans - Possible Implications For Reward and DepressionHasse HasseNo ratings yet
- The Journal of Physiology - 2016 - Nokia - Physical Exercise Increases Adult Hippocampal Neurogenesis in Male Rats ProvidedDocument19 pagesThe Journal of Physiology - 2016 - Nokia - Physical Exercise Increases Adult Hippocampal Neurogenesis in Male Rats Providedelspops.tab05No ratings yet
- 33 Malchow2016Document10 pages33 Malchow2016Sergio Machado NeurocientistaNo ratings yet
- Gray 2014Document10 pagesGray 2014Nada MachichNo ratings yet
- Bougea 2013Document9 pagesBougea 2013Lia YulianiNo ratings yet
- 1 s2.0 S2095254619301073 MainDocument8 pages1 s2.0 S2095254619301073 MainNia RwNo ratings yet
- Vipasaana and FmriDocument21 pagesVipasaana and FmriAravind VeeraraghavanNo ratings yet
- Papn MS Id 000156Document7 pagesPapn MS Id 000156niekoNo ratings yet
- International Journal of Health Sciences and ResearchDocument8 pagesInternational Journal of Health Sciences and Researchagil1094No ratings yet
- Capstone OutlineDocument4 pagesCapstone Outlineapi-310320629No ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptFrontiersNo ratings yet
- Jurnal 9 Neuropatic Pain On HIVDocument22 pagesJurnal 9 Neuropatic Pain On HIVKukuhWibisonoNo ratings yet
- Nutrients: The Effect of Chicken Extract On Mood, Cognition and Heart Rate VariabilityDocument18 pagesNutrients: The Effect of Chicken Extract On Mood, Cognition and Heart Rate VariabilityNeri ErinNo ratings yet
- Bartlett 2020Document9 pagesBartlett 2020Erick SolisNo ratings yet
- Research. 244, 394-402Document6 pagesResearch. 244, 394-402annespeaks017No ratings yet
- Neurofeedback ResearchDocument50 pagesNeurofeedback Researchdocs1234567No ratings yet
- Impact of Acute Aerobic Exercise and Car20160312 5746 Kuirrl With Cover Page v2Document13 pagesImpact of Acute Aerobic Exercise and Car20160312 5746 Kuirrl With Cover Page v2Fellipe GodoyNo ratings yet
- JCSM 3 4 380 PDFDocument7 pagesJCSM 3 4 380 PDFAgus BlancoNo ratings yet
- Sheu 2003Document7 pagesSheu 2003CORO CORPSNo ratings yet
- Effect of Yoga On Short Term Heart Rate Variability Measure As A Stress Index in Subjunior Cyclists: A Pilot StudyDocument6 pagesEffect of Yoga On Short Term Heart Rate Variability Measure As A Stress Index in Subjunior Cyclists: A Pilot StudysujiNo ratings yet
- Griffin 2011Document8 pagesGriffin 2011anang fajarNo ratings yet
- Baihui EA RatsDocument9 pagesBaihui EA Ratsrebeca9230No ratings yet
- The Effects of Exercise On Self-Rated Sleep Among Adults With Chronic Sleep ComplaintsDocument10 pagesThe Effects of Exercise On Self-Rated Sleep Among Adults With Chronic Sleep ComplaintsDanielaa ZapataNo ratings yet
- 19 Duncan2016Document7 pages19 Duncan2016Sergio Machado NeurocientistaNo ratings yet
- Short-And Long-Term Effects of Exercise On Neck Muscle Function in Cervical Radiculopathy: A Randomized Clinical TrialDocument9 pagesShort-And Long-Term Effects of Exercise On Neck Muscle Function in Cervical Radiculopathy: A Randomized Clinical Trialvidisanjaya21No ratings yet
- Integrating A Portable Biofeedback Device Into Clinical Practice For Patients With Anxiety Disorders: Results of A Pilot StudyDocument7 pagesIntegrating A Portable Biofeedback Device Into Clinical Practice For Patients With Anxiety Disorders: Results of A Pilot StudyLuis A Gil PantojaNo ratings yet
- Adl Inter 1Document7 pagesAdl Inter 1dewi pspta sriNo ratings yet
- 6 Cheng2017Document7 pages6 Cheng2017Sergio Machado NeurocientistaNo ratings yet
- 2015 LeeDocument3 pages2015 LeeJavier PelaezNo ratings yet
- Liang 2021Document15 pagesLiang 2021lucianoNo ratings yet
- Psychology of Sport & Exercise: Nicola J. Robinson, Catharine Montgomery, Laura Swettenham, Amy WhiteheadDocument12 pagesPsychology of Sport & Exercise: Nicola J. Robinson, Catharine Montgomery, Laura Swettenham, Amy WhiteheadSanghita BiswasNo ratings yet
- Interface Between Hypothalamic-Pituitary-Adrenal Axis Andbrain-Derived Neurotrophic Factor in DepressionDocument13 pagesInterface Between Hypothalamic-Pituitary-Adrenal Axis Andbrain-Derived Neurotrophic Factor in DepressioncarlosNo ratings yet
- The Short-Term Effect of Hippotherapy On Spasticity in Patients With Spinal Cord InjuryDocument5 pagesThe Short-Term Effect of Hippotherapy On Spasticity in Patients With Spinal Cord InjuryMasa JovanovicNo ratings yet
- 2a3e PDFDocument5 pages2a3e PDFAnonymous b2k9ABe7eNo ratings yet
- Biofeedback and Neurofeedback Role in Physical Therapy Applied PsychophysiologyDocument27 pagesBiofeedback and Neurofeedback Role in Physical Therapy Applied Psychophysiologyesam jadNo ratings yet
- Ejercicios Fernando Gomez PinillaDocument14 pagesEjercicios Fernando Gomez PinillaYajaira Saavedra JimenezNo ratings yet
- Effects of Flotation Therapy On Relaxation and Mental StateDocument4 pagesEffects of Flotation Therapy On Relaxation and Mental Statefriend717No ratings yet
- Sudarshan Kriya Yoga Mejora El Control Autonómico Cardíaco en Pacientes Con Trastornos de Ansiedad-DepresiónDocument7 pagesSudarshan Kriya Yoga Mejora El Control Autonómico Cardíaco en Pacientes Con Trastornos de Ansiedad-DepresiónPablo Ignacio González GálvezNo ratings yet
- List of Papers Cited by Ilchi LeeDocument7 pagesList of Papers Cited by Ilchi LeeCharlie MitchellNo ratings yet
- 27 - Jpts 2014 785Document3 pages27 - Jpts 2014 785jayadevanNo ratings yet
- Experimental Gerontology: ArticleinfoDocument7 pagesExperimental Gerontology: ArticleinfoLaily Mita AndriaNo ratings yet
- Hypoglossal Nerve Stimulation Therapy Does Not Alter Tongue Protrusion Strength and Fatigability in Obstructive Sleep ApneaDocument8 pagesHypoglossal Nerve Stimulation Therapy Does Not Alter Tongue Protrusion Strength and Fatigability in Obstructive Sleep ApneaHamzeh AlsalhiNo ratings yet
- Altered States of Consciousness PDFDocument14 pagesAltered States of Consciousness PDFShunki YouNo ratings yet
- Pediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDDocument6 pagesPediatric Neurology: Hye-Ryun Yeh MD, Min-Jee Kim MD, Tae-Sung Ko MD, PHD, Mi-Sun Yum MD, PHD, Su-Jeong You MD, PHDAdrian KhomanNo ratings yet
- The Mechanism of Neurofeedback Training For TreatmDocument14 pagesThe Mechanism of Neurofeedback Training For TreatmcornelteusdeaNo ratings yet
- Comparison of Cranio-Cervical Flexion Training Versus Cervical Proprioception Training in Pt's With Chronic Neck PainDocument8 pagesComparison of Cranio-Cervical Flexion Training Versus Cervical Proprioception Training in Pt's With Chronic Neck Painbcvaughn019No ratings yet
- The Effects of Breath-Counting Meditation and Deep Breathing On Heart Rate VariabilityDocument9 pagesThe Effects of Breath-Counting Meditation and Deep Breathing On Heart Rate VariabilityMadame MoseilleNo ratings yet
- Summary of John J. Ratey with Eric Hagerman's SparkFrom EverandSummary of John J. Ratey with Eric Hagerman's SparkRating: 4 out of 5 stars4/5 (2)
- Controlledstudy AJCM2007Document30 pagesControlledstudy AJCM2007Sergio Machado NeurocientistaNo ratings yet
- 43 Beebe2013Document7 pages43 Beebe2013Sergio Machado NeurocientistaNo ratings yet
- 31 Malchow2015Document12 pages31 Malchow2015Sergio Machado NeurocientistaNo ratings yet
- 22 Masa Font2015Document9 pages22 Masa Font2015Sergio Machado NeurocientistaNo ratings yet
- 26 Sailer2015Document12 pages26 Sailer2015Sergio Machado NeurocientistaNo ratings yet
- 35 Ho2014Document7 pages35 Ho2014Sergio Machado NeurocientistaNo ratings yet
- 6 Cheng2017Document7 pages6 Cheng2017Sergio Machado NeurocientistaNo ratings yet
- The Ecological Validity of Neuropsychological Tests: A Review of The Literature On Everyday Cognitive SkillsDocument17 pagesThe Ecological Validity of Neuropsychological Tests: A Review of The Literature On Everyday Cognitive SkillsSergio Machado NeurocientistaNo ratings yet
- 6 - Takahashi2012Document6 pages6 - Takahashi2012Sergio Machado NeurocientistaNo ratings yet
- 2 - Papiol2017Document9 pages2 - Papiol2017Sergio Machado NeurocientistaNo ratings yet
- Prinz 1995Document8 pagesPrinz 1995Sergio Machado NeurocientistaNo ratings yet
- 27 Loh2015Document11 pages27 Loh2015Sergio Machado NeurocientistaNo ratings yet
- 10 Su2016Document41 pages10 Su2016Sergio Machado NeurocientistaNo ratings yet
- Carlesimo 1992Document51 pagesCarlesimo 1992Sergio Machado NeurocientistaNo ratings yet
- 13 Yoon2016Document7 pages13 Yoon2016Sergio Machado NeurocientistaNo ratings yet
- 2009 Can Cognitive Exercise Prevent The Onset of Dementia Systematic Review of Randomized Clinical Trials With Longitudinal Follow UpDocument9 pages2009 Can Cognitive Exercise Prevent The Onset of Dementia Systematic Review of Randomized Clinical Trials With Longitudinal Follow UpSergio Machado NeurocientistaNo ratings yet
- Journal of Neuroengineering and Rehabilitation: Motor Rehabilitation Using Virtual RealityDocument8 pagesJournal of Neuroengineering and Rehabilitation: Motor Rehabilitation Using Virtual RealitySergio Machado NeurocientistaNo ratings yet
- Link To Publication in University of Groningen/UMCG Research DatabaseDocument19 pagesLink To Publication in University of Groningen/UMCG Research DatabaseSergio Machado NeurocientistaNo ratings yet
- Cognitive Rehabilitation For Schizophrenia: Problems, Prospects, and StrategiesDocument18 pagesCognitive Rehabilitation For Schizophrenia: Problems, Prospects, and StrategiesSergio Machado NeurocientistaNo ratings yet
- 14 FullDocument17 pages14 FullSergio Machado NeurocientistaNo ratings yet
- 01 DTMDocument2 pages01 DTMMauro BorgesNo ratings yet
- PRACTICA 3 - Holguino ErnestoDocument6 pagesPRACTICA 3 - Holguino ErnestoErnesto HolguinoNo ratings yet
- ABB Control TP180DA DatasheetDocument3 pagesABB Control TP180DA Datasheetntdien923100% (1)
- Analisis de Pesticidas Usandom FragmentacionDocument159 pagesAnalisis de Pesticidas Usandom FragmentacionroxanaNo ratings yet
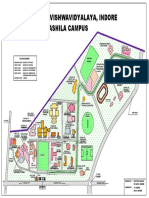
- Devi Ahilya Vishwavidyalaya, Indore Takshashila Campus: Vigyan BhawanDocument1 pageDevi Ahilya Vishwavidyalaya, Indore Takshashila Campus: Vigyan BhawankapasNo ratings yet
- Notes Receivable and Loan ReceivableDocument21 pagesNotes Receivable and Loan ReceivableLady BelleNo ratings yet
- Bluthner PRO 88 Owners enDocument20 pagesBluthner PRO 88 Owners enAnonymous pMgjvHvC41No ratings yet
- Role of Open Surgical Drainage or Aspiration in Management of Amoebic Liver AbscessDocument9 pagesRole of Open Surgical Drainage or Aspiration in Management of Amoebic Liver AbscessIJAR JOURNALNo ratings yet
- Letter From Harvard Leaders To EPA's Andrew Wheeler On Proposed Science PolicyDocument60 pagesLetter From Harvard Leaders To EPA's Andrew Wheeler On Proposed Science PolicyEmily AtkinNo ratings yet
- 30 - Standard 2.4.1Document3 pages30 - Standard 2.4.1Zain ZearkNo ratings yet
- Tle Ia Q4 Week 5Document46 pagesTle Ia Q4 Week 5Joevelyn Adaron GalayNo ratings yet
- Artwork: One-Alpha 0.25 Microgram Soft Capsules One-Alpha 0.5 Microgram Soft Capsules One-Alpha 1 Microgram Soft CapsulesDocument2 pagesArtwork: One-Alpha 0.25 Microgram Soft Capsules One-Alpha 0.5 Microgram Soft Capsules One-Alpha 1 Microgram Soft CapsulesJia Weng FungNo ratings yet
- On The Job Evaluation SheetDocument2 pagesOn The Job Evaluation Sheetmoonbright27No ratings yet
- Fresh AHU ComparisonDocument8 pagesFresh AHU Comparisonevo2oo2No ratings yet
- Vascular and Non-Vascular PlantsDocument3 pagesVascular and Non-Vascular PlantsLeonardo PigaNo ratings yet
- The Sinister Genius of Qassem Soleimani - WSJ PDFDocument5 pagesThe Sinister Genius of Qassem Soleimani - WSJ PDFMuhammad Anique RawnNo ratings yet
- Final Fortran Questions 1Document5 pagesFinal Fortran Questions 1Serdar BilgeNo ratings yet
- MS Fragmentation Functional Groups (Compatibility Mode)Document68 pagesMS Fragmentation Functional Groups (Compatibility Mode)Adriana Estefanía HPNo ratings yet
- Development On Plot No. Donyo Sabuk/Komarock BLOCK 1/25878 Client: Lilian Lutta MalobaDocument12 pagesDevelopment On Plot No. Donyo Sabuk/Komarock BLOCK 1/25878 Client: Lilian Lutta MalobaAustin AnindoNo ratings yet
- Full Download Test Bank For Workshop Statistics Discovery With Data 4th Edition Allan J Rossman Beth L Chance PDF Full ChapterDocument36 pagesFull Download Test Bank For Workshop Statistics Discovery With Data 4th Edition Allan J Rossman Beth L Chance PDF Full Chapterpithsomeknockingsawv100% (24)
- Manual de Servicio Treadmill 2000Document150 pagesManual de Servicio Treadmill 2000pirihuey1234No ratings yet
- Cityscope Sports and LeisureDocument7 pagesCityscope Sports and LeisurePD HoàngNo ratings yet
- Acupressure Animal SheltersDocument1 pageAcupressure Animal SheltersIoana SavaNo ratings yet
- Grid Code For FgPeninsular MalaysiaDocument460 pagesGrid Code For FgPeninsular MalaysiaberapiNo ratings yet
- Iygb Gce: Core Mathematics C2 Advanced SubsidiaryDocument6 pagesIygb Gce: Core Mathematics C2 Advanced SubsidiaryssmithNo ratings yet
- Introduction To Computational Finance and Financial EconometricsDocument54 pagesIntroduction To Computational Finance and Financial EconometricsMR 2No ratings yet
- Savage: Science Fiction Roleplaying For Savage WorldsDocument45 pagesSavage: Science Fiction Roleplaying For Savage WorldsJohn Churchill0% (1)
- CTDI Phantom User's GuideDocument18 pagesCTDI Phantom User's GuideAida Cristiana SanduNo ratings yet
- Caltex Vs PalomarDocument1 pageCaltex Vs PalomarDean Ben100% (2)