Download as pdf or txt
You might also like
- Dubai World Ehs - 2007 Regulations & StandardsDocument106 pagesDubai World Ehs - 2007 Regulations & StandardsSAYED100% (10)
- ASPEN Pediatría 2017Document37 pagesASPEN Pediatría 2017Consultorio Pediatria ShaioNo ratings yet
- Guia Esphan Espen Espr Cspen Nutricion ParenteralDocument127 pagesGuia Esphan Espen Espr Cspen Nutricion ParenteralLuz Dary Paez VArgasNo ratings yet
- PYMS TamizajeDocument6 pagesPYMS TamizajeKevinGallagherNo ratings yet
- J Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultDocument30 pagesJ Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultPabloNo ratings yet
- Clinical Impact of Prescribed Doses of Nutrients For Patients Exclusively Receiving Parenteral Nutrition in Japanese HospitalsDocument9 pagesClinical Impact of Prescribed Doses of Nutrients For Patients Exclusively Receiving Parenteral Nutrition in Japanese Hospitalsmarco marcoNo ratings yet
- J Parenter Enteral Nutr - 2017 - Mehta - Guidelines For The Provision and Assessment of Nutrition Support Therapy in TheDocument37 pagesJ Parenter Enteral Nutr - 2017 - Mehta - Guidelines For The Provision and Assessment of Nutrition Support Therapy in TheZ. Raquel García OsornoNo ratings yet
- A Stepwise Enteral Nutrition Algorithm For Critically Ill ChildrenDocument13 pagesA Stepwise Enteral Nutrition Algorithm For Critically Ill ChildrenHerwina BrahmantyaNo ratings yet
- Assesing The Appropriatenes of Parenteral Nutrition Use in Hospitalized Patients EspenDocument8 pagesAssesing The Appropriatenes of Parenteral Nutrition Use in Hospitalized Patients EspenDarío ParraNo ratings yet
- J Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultDocument30 pagesJ Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The Adultsulemi castañonNo ratings yet
- A Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)Document7 pagesA Stepwise Enteral Nutrition Algorithm For Critically (Susan Dan Nilesh Mehta)NyomanGinaHennyKristiantiNo ratings yet
- Ems 113478Document16 pagesEms 113478AfniNo ratings yet
- 10 1002@jpen 1723Document16 pages10 1002@jpen 1723Helena OliveiraNo ratings yet
- LitiasisDocument7 pagesLitiasisSandy SalazarNo ratings yet
- Nutrition Therapy in Critically Ill Patients A Review of Current Evidence For CliniciansDocument7 pagesNutrition Therapy in Critically Ill Patients A Review of Current Evidence For CliniciansangiolikkiaNo ratings yet
- ESPEN Guidelines On Nutritional Support For Polymorbid Internal Med PatDocument18 pagesESPEN Guidelines On Nutritional Support For Polymorbid Internal Med PatAmany SalamaNo ratings yet
- Nut in Clin Prac - 2023 - Mohamed Elfadil - Peptide Based Formula Clinical Applications and BenefitsDocument11 pagesNut in Clin Prac - 2023 - Mohamed Elfadil - Peptide Based Formula Clinical Applications and BenefitshizburNo ratings yet
- Nutrition Practices With A Focus On Parenteral NutDocument10 pagesNutrition Practices With A Focus On Parenteral NutJose VasquezNo ratings yet
- Post-ICU Nutrition The Neglected Side of Metabolic SupportDocument3 pagesPost-ICU Nutrition The Neglected Side of Metabolic SupportHubert PastasNo ratings yet
- 1 s2.0 S0261561420301941 MainDocument8 pages1 s2.0 S0261561420301941 MainNatalia BeltranNo ratings yet
- Clinical Nutrition: ESPEN GuidelineDocument18 pagesClinical Nutrition: ESPEN GuidelineMariana RodriguesNo ratings yet
- Nutritional ManagmentDocument19 pagesNutritional ManagmentgianellaNo ratings yet
- Parenteral Nutrition Objectives For Very Low Birth Weight Infants: Results of A National SurveyDocument9 pagesParenteral Nutrition Objectives For Very Low Birth Weight Infants: Results of A National SurveyjlionelmoNo ratings yet
- Perioperative Nutrition in Extremely Preterm Infants Undergoing Surgery For Patent Ductus ArteriosusDocument12 pagesPerioperative Nutrition in Extremely Preterm Infants Undergoing Surgery For Patent Ductus ArteriosusOctavianus KevinNo ratings yet
- Characterizing International Approaches To Weaning Children From Tube Feeding - A Scoping ReviewDocument12 pagesCharacterizing International Approaches To Weaning Children From Tube Feeding - A Scoping Revieweo.mobilestoreNo ratings yet
- Simple Nutrition Screening Tool For Pediatric InpatientsDocument7 pagesSimple Nutrition Screening Tool For Pediatric InpatientsYulmira YulmiraNo ratings yet
- Wong 2016Document7 pagesWong 2016Andreas Dhymas DmkNo ratings yet
- 1.2.21 Aspects of Protected Mealtimes Are Associated With Improved Mealtime Energy and Protein Intakes in Hospitalized Adult Patients On Medical and Surgical Wards Over 2 YearsDocument5 pages1.2.21 Aspects of Protected Mealtimes Are Associated With Improved Mealtime Energy and Protein Intakes in Hospitalized Adult Patients On Medical and Surgical Wards Over 2 Yearsciksas19No ratings yet
- Nutrients: Complications Associated With Enteral Nutrition: CAFANE StudyDocument12 pagesNutrients: Complications Associated With Enteral Nutrition: CAFANE StudySiti WarohmahNo ratings yet
- Mekhancha Dahel2014Document1 pageMekhancha Dahel2014richard menzNo ratings yet
- 2022 - Enteral Feeding, IF 2.2Document8 pages2022 - Enteral Feeding, IF 2.2Manal Haj HamadNo ratings yet
- A Systematic Review of Practice Surveys On Parenteral Nutrition For Preterm InfantsDocument5 pagesA Systematic Review of Practice Surveys On Parenteral Nutrition For Preterm InfantsKhor Chin PooNo ratings yet
- Kad 2Document50 pagesKad 2nellieauthorNo ratings yet
- (2019) Parenteral Nutrition in The ICU Lessons Learned Over The Past Few YearsDocument7 pages(2019) Parenteral Nutrition in The ICU Lessons Learned Over The Past Few YearsAnna Maria Ariesta PutriNo ratings yet
- ASPEN NutritionDocument18 pagesASPEN Nutritionsilvio da costa guerreiroNo ratings yet
- 1 s2.0 S2405457722000432 MainDocument7 pages1 s2.0 S2405457722000432 MainjvracuyaNo ratings yet
- Optimal Timing For Introducing Enteral Nutrition in The Neonatal Intensive Care UnitDocument8 pagesOptimal Timing For Introducing Enteral Nutrition in The Neonatal Intensive Care UnitAnonymous 1EQutBNo ratings yet
- Intensive & Critical Care Nursing: Research ArticleDocument6 pagesIntensive & Critical Care Nursing: Research ArticleJaemin cuteNo ratings yet
- Volume-Based Protocol Improves Delivery of Enteral Nutrition in Critically Ill Trauma Patients 2020Document6 pagesVolume-Based Protocol Improves Delivery of Enteral Nutrition in Critically Ill Trauma Patients 2020Marcelo Andrés Ortega ArjonaNo ratings yet
- ESPEN Practical Guideline Clinical Nutrition in Inflammatory Bowel DiseaseDocument22 pagesESPEN Practical Guideline Clinical Nutrition in Inflammatory Bowel DiseaseChico MotaNo ratings yet
- Jurnal AningDocument7 pagesJurnal AningSitaNo ratings yet
- Nutritional Management of The Critically Ill.29Document16 pagesNutritional Management of The Critically Ill.29Ririn Muthia ZukhraNo ratings yet
- Artigo - Compliance Oral Nutrition Supplement - ReviewDocument20 pagesArtigo - Compliance Oral Nutrition Supplement - ReviewFrancielle A.RNo ratings yet
- 2 ESPEN-ESPGHAN-ECFS Guidelines On Nutrition Care For Infants Children and Adults With Cystic FibrosisDocument21 pages2 ESPEN-ESPGHAN-ECFS Guidelines On Nutrition Care For Infants Children and Adults With Cystic FibrosisAmany SalamaNo ratings yet
- Association of Infant Feeding Practices and Food NDocument11 pagesAssociation of Infant Feeding Practices and Food NBULAN IFTINAZHIFANo ratings yet
- Improving Growth of Infants With Congenital Heart Disease Using A Consensus-Based Nutritional PathwayDocument8 pagesImproving Growth of Infants With Congenital Heart Disease Using A Consensus-Based Nutritional Pathwaybela siskaNo ratings yet
- 23 - Bapat2019Document10 pages23 - Bapat2019Rosa PerezNo ratings yet
- Nutricion ParenteralDocument18 pagesNutricion ParenteralTadeo PradoNo ratings yet
- Berger-Monitoreo Nutricional en UCI-2018Document10 pagesBerger-Monitoreo Nutricional en UCI-2018Brayan AuntaNo ratings yet
- Clinical Nutrition ESPENDocument15 pagesClinical Nutrition ESPENBBD BBDNo ratings yet
- Guidelines ASPENDocument138 pagesGuidelines ASPENJaqueline Odair100% (1)
- Nutrition of The Critically Ill Patient and Effects of Implementing A Nutritional Support Algorithm in ICUDocument10 pagesNutrition of The Critically Ill Patient and Effects of Implementing A Nutritional Support Algorithm in ICUFildzah Aulia UlhaqNo ratings yet
- Parenter Enteral Nutr 2009 Mehta 260 76Document17 pagesParenter Enteral Nutr 2009 Mehta 260 76Bogdan CarabasNo ratings yet
- YOR-PICU-001 Updated en Guidelines Dec 2013Document16 pagesYOR-PICU-001 Updated en Guidelines Dec 2013Meirinda HidayantiNo ratings yet
- The Benefits of Early Oral Nutrition in Mild Acute PancreatitisDocument6 pagesThe Benefits of Early Oral Nutrition in Mild Acute PancreatitisrayiNo ratings yet
- Insulin Treatment in Children and Adolescents With DiabetesDocument20 pagesInsulin Treatment in Children and Adolescents With Diabetesmreda983No ratings yet
- PYMS Is A Reliable Malnutrition Screening ToolsDocument8 pagesPYMS Is A Reliable Malnutrition Screening ToolsRika LedyNo ratings yet
- PIIS2405457722004831Document4 pagesPIIS2405457722004831Karla Rosángel CordónNo ratings yet
- Total Nutritional Therapy: A Nutrition Education Program For PhysiciansDocument7 pagesTotal Nutritional Therapy: A Nutrition Education Program For PhysiciansTia WasrilNo ratings yet
- Negative Impact of Hypocaloric Feeding and Energy Balance On Clinical Outcome in ICU PatientsDocument8 pagesNegative Impact of Hypocaloric Feeding and Energy Balance On Clinical Outcome in ICU PatientsDaniela HernandezNo ratings yet
- The Lovely BonesDocument2 pagesThe Lovely BonesJohn ConstantineNo ratings yet
- Laptop Price List-Afresh笔记本Document6 pagesLaptop Price List-Afresh笔记本Miriam BarahonaNo ratings yet
- MBA Syllabus 2021 NewDocument245 pagesMBA Syllabus 2021 Newarchana97anilNo ratings yet
- SensION1 ManualDocument40 pagesSensION1 ManualMaria Victoria GuarinNo ratings yet
- Digital WatermarkingDocument29 pagesDigital WatermarkingAngelNo ratings yet
- Android - Architecture: Linux KernelDocument3 pagesAndroid - Architecture: Linux KernelMahnoor AslamNo ratings yet
- Preventionof HypothermiaDocument2 pagesPreventionof HypothermiarisnayektiNo ratings yet
- The Marketing Challenge of Low Resource CustomersDocument7 pagesThe Marketing Challenge of Low Resource Customersvivek mithraNo ratings yet
- Ieee C37.20.3-2013Document70 pagesIeee C37.20.3-2013damaso taracena100% (2)
- Spss SyllabusDocument2 pagesSpss SyllabusBhagwati ShuklaNo ratings yet
- Stinger 3470: Boom Truck CraneDocument4 pagesStinger 3470: Boom Truck CraneKatherinne ChicaNo ratings yet
- A Semi Detailed Lesson Plan in Physical ScienceDocument2 pagesA Semi Detailed Lesson Plan in Physical ScienceHannah Jane AllesaNo ratings yet
- Afd 021019 1 1B 50Document100 pagesAfd 021019 1 1B 50Sab-Win DamadNo ratings yet
- Shell Turbo Oil T46: Performance, Features & Benefits Main ApplicationsDocument4 pagesShell Turbo Oil T46: Performance, Features & Benefits Main Applicationshaider100% (1)
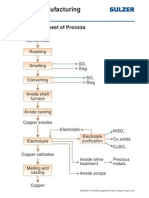
- Copper Manufacturing Process: General Flowsheet of ProcessDocument28 pagesCopper Manufacturing Process: General Flowsheet of ProcessflaviosazevedoNo ratings yet
- Donald Redford - Akhenaten - New Theories and Old FactsDocument27 pagesDonald Redford - Akhenaten - New Theories and Old FactsDjatmiko TanuwidjojoNo ratings yet
- Big Data Analytics (2017 Regulation) : Unit - 2 Clustering and ClassificationDocument7 pagesBig Data Analytics (2017 Regulation) : Unit - 2 Clustering and ClassificationcskinitNo ratings yet
- Ghost Usb Honeypot MasterDocument15 pagesGhost Usb Honeypot MasterVinamra MittalNo ratings yet
- Laboratory Rules and SafetyDocument9 pagesLaboratory Rules and SafetyMehul KhimaniNo ratings yet
- Final - ERP Implementation in Indian ContextDocument9 pagesFinal - ERP Implementation in Indian Contextsurajmukti0% (1)
- 25 191 1 PB PDFDocument11 pages25 191 1 PB PDFRaihatil UmmiNo ratings yet
- The Impact of Psak 73 Implementation On Leases in Indonesia Telecommunication CompaniesDocument17 pagesThe Impact of Psak 73 Implementation On Leases in Indonesia Telecommunication CompaniesAnin YusufNo ratings yet
- 02-Mushtaq Ali LigariDocument32 pages02-Mushtaq Ali LigariAbdul Arham BalochNo ratings yet
- 2020 ECO Topic 1 International Economic Integration Notes HannahDocument23 pages2020 ECO Topic 1 International Economic Integration Notes HannahJimmyNo ratings yet
- Digital BankingDocument3 pagesDigital BankingDPC Gym100% (1)
- Phil Hine en PermutationsDocument41 pagesPhil Hine en Permutationsgunter unserNo ratings yet
- Servest Training CatalogueDocument62 pagesServest Training Catalogueayandamakabongwe06No ratings yet
- DVT Case StudyDocument3 pagesDVT Case StudyCrystal B Costa78No ratings yet
- MTH151 Syllabus S12Document6 pagesMTH151 Syllabus S12schreckk118No ratings yet