Download as pdf or txt
You might also like
- Exoplan.2.3.Supported Implant Libraries enDocument18 pagesExoplan.2.3.Supported Implant Libraries envaleriu vatamanNo ratings yet
- F& C OSCE Notes - University of Manchester, WL GanDocument57 pagesF& C OSCE Notes - University of Manchester, WL GanWeh Loong Gan100% (7)
- General Lung Cancer Fact Sheet 2017Document2 pagesGeneral Lung Cancer Fact Sheet 2017Hendarsyah SuryadinataNo ratings yet
- Does Open or Closed Endotracheal Suction Affect The Incidence of Ventilator Associated Pneumonia in The Intensive Care Unit A Systematic ReviewDocument7 pagesDoes Open or Closed Endotracheal Suction Affect The Incidence of Ventilator Associated Pneumonia in The Intensive Care Unit A Systematic Reviewaperfectcircle7978No ratings yet
- Senam LafiskaDocument6 pagesSenam LafiskaAyuNo ratings yet
- Referral 9b66451b 9b66451bDocument1 pageReferral 9b66451b 9b66451bleonelale95No ratings yet
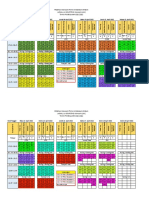
- Jadwal UKK FixDocument2 pagesJadwal UKK FixandikNo ratings yet
- Retrospective Review of Laparoscopic Versus Open.27Document6 pagesRetrospective Review of Laparoscopic Versus Open.27Lena Wahyu SetianingsihNo ratings yet
- Educati On Stati Sti CS: X-Axi S I Ndi Cat orDocument1 pageEducati On Stati Sti CS: X-Axi S I Ndi Cat orSih Calimio DesepazNo ratings yet
- GP Fellowship Pathway: Eligibility RequirementsDocument2 pagesGP Fellowship Pathway: Eligibility RequirementsNataraj ThambiNo ratings yet
- Unlocking T Cell Potential Multiparameter Characterization of CAR T Cells 1711606816Document1 pageUnlocking T Cell Potential Multiparameter Characterization of CAR T Cells 1711606816pramod226No ratings yet
- Update On Difficult Airway Management With A.10Document10 pagesUpdate On Difficult Airway Management With A.10Minaz PatelNo ratings yet
- MulteeDocument1 pageMulteeGavin MuhammadNo ratings yet
- Queen's Medical Centre Corridor Plan NHS: E FloorDocument1 pageQueen's Medical Centre Corridor Plan NHS: E Floorgoogle manNo ratings yet
- Ispa NOPEMBER PKM Bawan - 105924Document1 pageIspa NOPEMBER PKM Bawan - 105924Harianto Taro SembiringNo ratings yet
- Current Affairs-153Document3 pagesCurrent Affairs-153Ganji LakshmanaraoNo ratings yet
- Finding Your Way Around NNIDocument2 pagesFinding Your Way Around NNIcarlson.aberin2020No ratings yet
- IONIX ModelDocument6 pagesIONIX ModelTrường Bửu TrầnNo ratings yet
- gender sensitiveDocument52 pagesgender sensitiveRG JulianNo ratings yet
- Nilai Raport KLS Xi Upw 1 SMT 2Document16 pagesNilai Raport KLS Xi Upw 1 SMT 2artha wiriye negareNo ratings yet
- Nilai Raport KLS Xi Upw 1 SMT 1Document16 pagesNilai Raport KLS Xi Upw 1 SMT 1artha wiriye negareNo ratings yet
- Mental Health Quiz Online - Psychiatric Disorders - Mental Health Nursing - Nursing OfficerDocument26 pagesMental Health Quiz Online - Psychiatric Disorders - Mental Health Nursing - Nursing OfficermanishjeswalNo ratings yet
- Gynecological Tumors SummaryDocument1 pageGynecological Tumors SummaryZahid iqbalNo ratings yet
- Doctors PrescriptionDocument1 pageDoctors Prescriptionmanisha.sharma.gnpsNo ratings yet
- BEH UpdatedDocument1 pageBEH Updatedqw46qyzhb5No ratings yet
- Schedule 3rd-Year5th-Sem-22-23Document1 pageSchedule 3rd-Year5th-Sem-22-23Rosalia RozzaNo ratings yet
- Now Any DREAM Can Become A REALITY With Us.: Admission AnnouncementDocument6 pagesNow Any DREAM Can Become A REALITY With Us.: Admission AnnouncementResonance KotaNo ratings yet
- Reproduction RevisionDocument1 pageReproduction RevisionAngeline AngelNo ratings yet
- Laporan Posyandu April 2021contohDocument2 pagesLaporan Posyandu April 2021contohmegaNo ratings yet
- Radiology 101Document2 pagesRadiology 101Nadhirah AnandaNo ratings yet
- Batman2 Scenario SuicideSquad enDocument7 pagesBatman2 Scenario SuicideSquad enJohn OldfieldNo ratings yet
- Jan NewsletterDocument1 pageJan NewsletteramittotallyattitudeNo ratings yet
- Garnet Education Catalogue 2010Document66 pagesGarnet Education Catalogue 2010garneteducationNo ratings yet
- Practicalskillschecklist 2017 - 2018 Week 13Document12 pagesPracticalskillschecklist 2017 - 2018 Week 13api-395143739No ratings yet
- F TestDocument1 pageF TestVEDPRAKASH MOHAPATRANo ratings yet
- Aula 5 Logica PolicialDocument1 pageAula 5 Logica PolicialWillian GutierrezNo ratings yet
- Rekapan Sasaran Kel. Nnkan Utara, TengahDocument3 pagesRekapan Sasaran Kel. Nnkan Utara, TengahsyahrirNo ratings yet
- WHO MEC-wheel PDFDocument8 pagesWHO MEC-wheel PDFBillyNicolasNo ratings yet
- Business Model CanvasDocument1 pageBusiness Model CanvasPrateek AnandNo ratings yet
- 6643ed56217a8 Program - Aabip24 Paag April2Document3 pages6643ed56217a8 Program - Aabip24 Paag April2otis2ke9588No ratings yet
- Result May 2022 Mpmsu MbbsDocument22 pagesResult May 2022 Mpmsu MbbsSiya PatilNo ratings yet
- Ledger Semester GenapDocument7 pagesLedger Semester GenapEli LasmiNo ratings yet
- MAPEHDocument23 pagesMAPEHStephannie RepunteNo ratings yet
- Statistics Thống KêDocument11 pagesStatistics Thống KêVu Khanh HuyenNo ratings yet
- Monitoring XV03312016145339Document4 pagesMonitoring XV03312016145339ArifahMaharanyNurIINo ratings yet
- Applies To:: Description Occurrence Symptoms Impact Statement Recommendation Workaround Solution HistoryDocument1 pageApplies To:: Description Occurrence Symptoms Impact Statement Recommendation Workaround Solution HistorypsaikrishNo ratings yet
- Jimenez Guerra Carlos HugoDocument1 pageJimenez Guerra Carlos HugoHugo CarlosNo ratings yet
- Wondfo BrochureDocument10 pagesWondfo BrochureKrijan Man VaidyaNo ratings yet
- Readable FileDocument1 pageReadable Filetanveerali2108No ratings yet
- Secuencia Final Ashtanga (Todas Las Series)Document1 pageSecuencia Final Ashtanga (Todas Las Series)Cristián IgnacioNo ratings yet
- Cerebral Vasospasme After Traumatic Brain InjuryDocument10 pagesCerebral Vasospasme After Traumatic Brain Injurydavid wyantoNo ratings yet
- Shortlist 2Document1 pageShortlist 2rahul dandonaNo ratings yet
- Format For Tracking & Tagging of Pregnancies For The Month of August - 2019Document12 pagesFormat For Tracking & Tagging of Pregnancies For The Month of August - 2019Vallepu MahendrakumarNo ratings yet
- Absen DP-V PN N.CDocument25 pagesAbsen DP-V PN N.CUmmu AlfatimahNo ratings yet
- Edited Leishmaniasis Register MarDocument1 pageEdited Leishmaniasis Register MarDagnachew MulugetaNo ratings yet
- Loïc Caloren - NBS 2021 PosterDocument1 pageLoïc Caloren - NBS 2021 PosterCBR UBCNo ratings yet
- Anatomia 5Document18 pagesAnatomia 5lbnNo ratings yet
- Python Programming - Mindmap - Opendir - CloudDocument2 pagesPython Programming - Mindmap - Opendir - Cloudadapa.sai2022No ratings yet
- Form - 13. Data SDM Program Kesehatan Anak 2022.Xlsx - Tahunan (SDM)Document4 pagesForm - 13. Data SDM Program Kesehatan Anak 2022.Xlsx - Tahunan (SDM)walatangNo ratings yet
- Drug Study... MyomaDocument12 pagesDrug Study... MyomaChristine Joy Bautista- CastroNo ratings yet
- Chapter IDocument8 pagesChapter IVincent QuinaoNo ratings yet
- Pulmonary Diseases - Dental ManagementDocument45 pagesPulmonary Diseases - Dental Managementfilyouth4life100% (3)
- SOP Open Access Endoscopy Updated30AprilDocument29 pagesSOP Open Access Endoscopy Updated30AprilmungicideNo ratings yet
- Who Ten Step Management of Severe MalnutritionDocument4 pagesWho Ten Step Management of Severe MalnutritionShely Karma Astuti50% (4)
- BREASTFEEDING ResearchDocument17 pagesBREASTFEEDING ResearchshaileshNo ratings yet
- KSR RS BZAp1Document41 pagesKSR RS BZAp1ksr prasadNo ratings yet
- Protein Energy MalnutritionDocument44 pagesProtein Energy Malnutritionokwadha simionNo ratings yet
- Physicians' Open Letter To WHODocument3 pagesPhysicians' Open Letter To WHOGlennKesslerWPNo ratings yet
- PerindoprilDocument25 pagesPerindoprilYeyenJaejoongNo ratings yet
- Neuropsycholgical Assessment IgnouDocument29 pagesNeuropsycholgical Assessment IgnouFiroz AhmedNo ratings yet
- Notification MMRCL Various Vacancy PostsDocument14 pagesNotification MMRCL Various Vacancy PostsabhishekNo ratings yet
- VertigoandDizziness 2Document50 pagesVertigoandDizziness 2Au Ah Gelap100% (1)
- Acute Myocardial InfarctionDocument53 pagesAcute Myocardial InfarctionYew Ping Hee100% (1)
- Case Study MCN IIDocument19 pagesCase Study MCN IIAthena SaturdayNo ratings yet
- SRNA Orientation ChecklistDocument40 pagesSRNA Orientation Checklistihtisham1No ratings yet
- Strongman For Football Update 11.08Document20 pagesStrongman For Football Update 11.0814shoe100% (1)
- np1 5Document25 pagesnp1 5Sittie Haya LazimNo ratings yet
- 02 Aug14 Trans Neuro Pedia Correlates and PBL Session DrASalongaDocument3 pages02 Aug14 Trans Neuro Pedia Correlates and PBL Session DrASalongaDelsie Vicente100% (1)
- Multiple SclerosisDocument5 pagesMultiple SclerosisEliDavidNo ratings yet
- Welcome Homeopathy - Dr. S. C. MadanDocument195 pagesWelcome Homeopathy - Dr. S. C. Madanreza100% (4)
- W&W Homeopathic Medicines Product DetailsDocument26 pagesW&W Homeopathic Medicines Product DetailsErica Lindsey100% (3)
- Case Study 1Document13 pagesCase Study 1Kiana TehraniNo ratings yet
- Genetics: IAP UG Teaching Slides 2015-16Document39 pagesGenetics: IAP UG Teaching Slides 2015-16AkkiNo ratings yet
- Nutrition in Intensive Care: Richard Leonard ST Mary's Hospital, LondonDocument50 pagesNutrition in Intensive Care: Richard Leonard ST Mary's Hospital, LondonNurulain MD AnuarNo ratings yet
- Hypertension in PregnancyDocument101 pagesHypertension in PregnancyKevin ArroyoNo ratings yet
- Coronary Artery DiseaseDocument33 pagesCoronary Artery DiseaseAlma Rifa'Ana LiskaNo ratings yet
- CIR 0b013e3182742cf6 FullDocument88 pagesCIR 0b013e3182742cf6 FullKussetya AnggaNo ratings yet
- Women and Strength TrainingDocument18 pagesWomen and Strength Trainingkhajezade44No ratings yet