Download as pdf or txt
You might also like
- Test Bank For Handbook of Informatics For Nurses and Healthcare Professionals 6th Edition Toni L Hebda Kathleen Hunter Patricia CzarDocument17 pagesTest Bank For Handbook of Informatics For Nurses and Healthcare Professionals 6th Edition Toni L Hebda Kathleen Hunter Patricia Czarcourtneyriveraefjpadcmyx100% (31)
- Ethics in Health Services Management, Sixth Edition (Excerpt)Document12 pagesEthics in Health Services Management, Sixth Edition (Excerpt)Health Professions Press, an imprint of Paul H. Brookes Publishing Co., Inc.63% (8)
- Medical Billing Training ManualDocument51 pagesMedical Billing Training ManualRadha Raman SharmaNo ratings yet
- Two-Way Referral Form PDFDocument1 pageTwo-Way Referral Form PDFcatherine joy macalos100% (4)
- Basics of Medical Billing & CodingDocument86 pagesBasics of Medical Billing & CodingRic Sánchez100% (3)
- Appeal That ClaimDocument65 pagesAppeal That ClaimParag Shinde100% (2)
- Healthcare Revenue Cycle Management RCM Important Approach That Hospitals Should FollowDocument10 pagesHealthcare Revenue Cycle Management RCM Important Approach That Hospitals Should FollowMohab FawzyNo ratings yet
- Appeal That ClaimDocument65 pagesAppeal That ClaimYudhistira YuliandraNo ratings yet
- U A Managers's Charge Case StudyDocument9 pagesU A Managers's Charge Case Studyyt65hg2hvmNo ratings yet
- The UB-04 Claim Form and NPIDocument4 pagesThe UB-04 Claim Form and NPImyousafkNo ratings yet
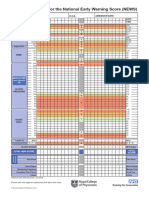
- Early Warning Score Chart PDFDocument2 pagesEarly Warning Score Chart PDFLucia NatashaNo ratings yet
- Program Integrity White PaperDocument8 pagesProgram Integrity White PaperGovtfraudlawyerNo ratings yet
- DOH AuditDocument25 pagesDOH AuditNews10NBC100% (1)
- Blog 13Document7 pagesBlog 13NobiaWahabNo ratings yet
- RecoveryAudits BookletDocument110 pagesRecoveryAudits Bookletsitu6100% (1)
- Textbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesFrom EverandTextbook of Urgent Care Management: Chapter 38, Audits by Managed-Care Organizations and Regulatory AgenciesNo ratings yet
- NR526 Collaboration Cafe M3Document5 pagesNR526 Collaboration Cafe M396rubadiri96No ratings yet
- Newman's Billing and Coding Technicians Study GuideFrom EverandNewman's Billing and Coding Technicians Study GuideRating: 4.5 out of 5 stars4.5/5 (2)
- Business of MedicineDocument9 pagesBusiness of MedicineCeline MorenoNo ratings yet
- OIG Compliance Program For Third-Party Medical Billing CompaniesDocument15 pagesOIG Compliance Program For Third-Party Medical Billing CompaniesaaronborosNo ratings yet
- Chapter 10: Fraud Management: Certificate in Health InsuranceDocument0 pagesChapter 10: Fraud Management: Certificate in Health InsuranceJonathon CabreraNo ratings yet
- MCM 7Document174 pagesMCM 7Mido HasaNo ratings yet
- General Medicaid RulesDocument4 pagesGeneral Medicaid RulesRam KumarNo ratings yet
- Risk Adjustment Data Validation of Payments Made To Pacificare of California For Calendar Year 2007Document64 pagesRisk Adjustment Data Validation of Payments Made To Pacificare of California For Calendar Year 2007christina_jewettNo ratings yet
- Blog 10Document7 pagesBlog 10NobiaWahabNo ratings yet
- 2016 National Training ProgramDocument50 pages2016 National Training ProgramTian Njawani100% (1)
- IG ReportDocument44 pagesIG ReportDaniel BentleyNo ratings yet
- Understanding Doctor'S Rights: Effective Use of E-Discovery: Edicare Verpayment UditsDocument31 pagesUnderstanding Doctor'S Rights: Effective Use of E-Discovery: Edicare Verpayment UditsEdward M RocheNo ratings yet
- Testimony For House Ways and Means Committee Subcommittee On OversightDocument11 pagesTestimony For House Ways and Means Committee Subcommittee On OversightjustinhorwathNo ratings yet
- HHS-OIG Medicaid Overcharges Pediatric DentalDocument35 pagesHHS-OIG Medicaid Overcharges Pediatric DentalDentist The MenaceNo ratings yet
- Federal Government Payer Program - MedicareDocument5 pagesFederal Government Payer Program - MedicarePeterNo ratings yet
- CMS Auditing SeriesDocument3 pagesCMS Auditing SeriesDiana FitriNo ratings yet
- Arnold Ventures IRA Excise Tax Comment LetterDocument3 pagesArnold Ventures IRA Excise Tax Comment LetterArnold VenturesNo ratings yet
- Madhav 2Document9 pagesMadhav 2chanikyanagipoguNo ratings yet
- White Paper - Utilization Management Through The Lens of Value-Based CareDocument7 pagesWhite Paper - Utilization Management Through The Lens of Value-Based CarevamseeNo ratings yet
- Medical Billing ProcessDocument24 pagesMedical Billing ProcessNajamHass100% (5)
- Federal Register / Vol. 63, No. 35 / Monday, February 23, 1998 / NoticesDocument12 pagesFederal Register / Vol. 63, No. 35 / Monday, February 23, 1998 / NoticesGudegna GemechuNo ratings yet
- Breaches and Medical Identity TheftDocument25 pagesBreaches and Medical Identity TheftTrent SeibertNo ratings yet
- Precertification by DR Delroy Jefferson PDFDocument38 pagesPrecertification by DR Delroy Jefferson PDFBernewsAdminNo ratings yet
- RAC Audit In-ServiceDocument15 pagesRAC Audit In-ServiceAndreaNo ratings yet
- Medical Coding and Compliance NIHDocument18 pagesMedical Coding and Compliance NIHBrandi TadlockNo ratings yet
- United States General Accounting Office Washington, DC 20548Document25 pagesUnited States General Accounting Office Washington, DC 20548politixNo ratings yet
- Comptroller's Medicaid AuditDocument25 pagesComptroller's Medicaid AuditDavid LombardoNo ratings yet
- Compendium 2021Document99 pagesCompendium 2021stacyNo ratings yet
- StateDataSpotlight ME May2011Document3 pagesStateDataSpotlight ME May2011SHADACNo ratings yet
- Pip Experience Draft1808Document10 pagesPip Experience Draft1808JamaliNo ratings yet
- Chapter IIDocument11 pagesChapter IIIsahNo ratings yet
- Pai Medical Audits White Paper Feb 162012Document23 pagesPai Medical Audits White Paper Feb 162012Ahmed GoudaNo ratings yet
- Downcoding and Bundling ClaimsDocument10 pagesDowncoding and Bundling ClaimsKarna Palanivelu100% (1)
- HHS OIG - Offshore Outsourcing OEI-09-12-00530Document13 pagesHHS OIG - Offshore Outsourcing OEI-09-12-00530Michael BarbereNo ratings yet
- Gaynor Et Al Final Report v11Document40 pagesGaynor Et Al Final Report v11padmanaban manickavelanNo ratings yet
- TOPICSDocument23 pagesTOPICSLili GomezNo ratings yet
- Mining for Gold In a Barren Land: Pioneer Accountable Care Organization Potential to Redesign the Healthcare Business Model in a Post-Acute SettingFrom EverandMining for Gold In a Barren Land: Pioneer Accountable Care Organization Potential to Redesign the Healthcare Business Model in a Post-Acute SettingNo ratings yet
- Maine Medicad Mistakes.Document3 pagesMaine Medicad Mistakes.Vamsi KrishnaNo ratings yet
- Final Project Submission - Edited.editedDocument15 pagesFinal Project Submission - Edited.editedSammy DeeNo ratings yet
- CERTMedRecDoc FactSheet ICN909160Document6 pagesCERTMedRecDoc FactSheet ICN909160KHAIRUL REDZUANNo ratings yet
- Final Project Submission - Edited.editedDocument15 pagesFinal Project Submission - Edited.editedSammy DeeNo ratings yet
- Compliance 2017Document5 pagesCompliance 2017Swisskelly1No ratings yet
- Medicaid Medical Record DocumentationDocument3 pagesMedicaid Medical Record DocumentationRam KumarNo ratings yet
- HealthcareDocument14 pagesHealthcareAntony AjowiNo ratings yet
- Behavioral Health Medical RecordsDocument4 pagesBehavioral Health Medical RecordsRam KumarNo ratings yet
- Office of Inspector General Report: Sunrise HospitalDocument53 pagesOffice of Inspector General Report: Sunrise HospitalFOX5 VegasNo ratings yet
- Michigan Medicaid Claim Predictive Modeling PolicyDocument2 pagesMichigan Medicaid Claim Predictive Modeling PolicyBeverly TranNo ratings yet
- Lamar State College - Port Arthur Upward Mobility Program RNSG 2361 Clinical Care PlanDocument5 pagesLamar State College - Port Arthur Upward Mobility Program RNSG 2361 Clinical Care PlanAlmaHernandezNo ratings yet
- Claim Process Flow ChartDocument2 pagesClaim Process Flow ChartanjnaNo ratings yet
- Thorpe - Wendy - Executive BioDocument1 pageThorpe - Wendy - Executive BioAnonymous LcWk91CsJFNo ratings yet
- The Art of Taking A Medical HistoryDocument4 pagesThe Art of Taking A Medical HistorypuneetNo ratings yet
- Understanding MedicareDocument4 pagesUnderstanding Medicare1224adhNo ratings yet
- Prevention of BedsoresDocument5 pagesPrevention of BedsoresMadhu KumarNo ratings yet
- 834 2224 1 SMDocument1 page834 2224 1 SMpatelmsNo ratings yet
- مفهوم التسويق الصحي لعجال العمريةDocument19 pagesمفهوم التسويق الصحي لعجال العمريةGhiles Battache100% (1)
- Impact of Medicaid Extension and Local Spending For Health Care by Texas House DistrictDocument300 pagesImpact of Medicaid Extension and Local Spending For Health Care by Texas House Districtbee5834No ratings yet
- House Hearing, 112TH Congress - Medicare Premium Support ProposalsDocument107 pagesHouse Hearing, 112TH Congress - Medicare Premium Support ProposalsScribd Government DocsNo ratings yet
- LTC LR 18Document227 pagesLTC LR 18Afik GalNo ratings yet
- Dpope Nurs5327 Teachingphilosophy WebsiteDocument2 pagesDpope Nurs5327 Teachingphilosophy Websiteapi-496551085No ratings yet
- Na PDP Classic Eoc 2022 Na2pdgeoc79428e RDocument146 pagesNa PDP Classic Eoc 2022 Na2pdgeoc79428e RMelva MosleyNo ratings yet
- My 1/20/20 Correspondence With Tomas Lopez of "Y-Strap - Com" of Seville, Spain - NO REPLY TO MY QUESTIONSDocument4 pagesMy 1/20/20 Correspondence With Tomas Lopez of "Y-Strap - Com" of Seville, Spain - NO REPLY TO MY QUESTIONSPeter M. HeimlichNo ratings yet
- Vba 21P 534ez AreDocument14 pagesVba 21P 534ez AreARNOLD GONZALESNo ratings yet
- Food Handlers Daily Handwashing Tracking Log SheetDocument1 pageFood Handlers Daily Handwashing Tracking Log SheetWeston Musonda Jr.No ratings yet
- Capstone FinalDocument36 pagesCapstone Finalsamantha pabalan100% (2)
- Fulfilling The Promise of Obamacare RepealDocument14 pagesFulfilling The Promise of Obamacare RepealJuniper Research GroupNo ratings yet
- Clinical Documentation in The Inpatient SettingDocument30 pagesClinical Documentation in The Inpatient SettingmeddouNo ratings yet
- FORTUNE: Caterpillar Serious ConsiderationDocument2 pagesFORTUNE: Caterpillar Serious ConsiderationFortuneNo ratings yet
- Star Health Medi Classic BrochureDocument2 pagesStar Health Medi Classic BrochureranchipkcNo ratings yet
- Hospitals List PDFDocument228 pagesHospitals List PDFGlobal Health Alliance FoundationNo ratings yet
- DR Athar RanaDocument2 pagesDR Athar Ranaatharrana1823No ratings yet
- 004 Goals and ObjectivesDocument4 pages004 Goals and ObjectivesAeryll JasminNo ratings yet
- Healthcare AnalyticsDocument9 pagesHealthcare AnalyticsRamyaNo ratings yet