
Labreportnew (8) - 3
Labreportnew (8) - 3
You might also like
- Pass Nclex IN 30 DAYS!Document9 pagesPass Nclex IN 30 DAYS!Jude olga75% (4)
- Computer System Validation Risk Assessment ToolDocument3 pagesComputer System Validation Risk Assessment Toolcpkakope100% (1)
- Vegan AestheticsDocument12 pagesVegan AestheticselyseNo ratings yet
- 1-Complete Blood Count - PO1106326185-399Document8 pages1-Complete Blood Count - PO1106326185-399Arup KumarNo ratings yet
- Po4009507960 540Document15 pagesPo4009507960 540PRADEEP KUMARNo ratings yet
- 1-Good Health Premium Package - PO1065281239-651Document19 pages1-Good Health Premium Package - PO1065281239-651Renu ChoudharyNo ratings yet
- Kidney FunctionDocument19 pagesKidney FunctionFarooq Bin MahfoozNo ratings yet
- DR. Neelanjana SHARMADocument5 pagesDR. Neelanjana SHARMADr. Neelanjana SharmaNo ratings yet
- Report 831a66a7 PDFDocument23 pagesReport 831a66a7 PDFViral PatelNo ratings yet
- Devendra - 2401611Document3 pagesDevendra - 2401611arslansiddique406No ratings yet
- agilius report_unlockedDocument8 pagesagilius report_unlockedSucharit NarangNo ratings yet
- Health Report 2023Document30 pagesHealth Report 2023Pranay GuptaNo ratings yet
- Don't Know Love - 1004584Document14 pagesDon't Know Love - 1004584baapj39No ratings yet
- 1-Women Wellness Premium Package_PO1180038496-860Document22 pages1-Women Wellness Premium Package_PO1180038496-860sttt13331No ratings yet
- Lab Report NewDocument5 pagesLab Report Newsamirghosal19No ratings yet
- Mr. Abhijeet BhoyarDocument9 pagesMr. Abhijeet BhoyarMahesh TilanteNo ratings yet
- Hematology: Test Name Result Reference Range Unit SpecimenDocument4 pagesHematology: Test Name Result Reference Range Unit Specimennirmala.arunanNo ratings yet
- Final: Code/Name & AddressDocument6 pagesFinal: Code/Name & AddresscrypticgarvNo ratings yet
- Comprehensive body lab reportDocument18 pagesComprehensive body lab reportTanvi PunjabiNo ratings yet
- 0056XF00339756_980475vDocument10 pages0056XF00339756_980475vAjay YadavNo ratings yet
- Checkup ReportDocument17 pagesCheckup Reportshashwatpandey736No ratings yet
- Report F412b1a3Document18 pagesReport F412b1a3055Nitish BhatiaNo ratings yet
- BloodDocument18 pagesBloodPriyanshu GuptaNo ratings yet
- Sangeeta Vishnio ReportsDocument13 pagesSangeeta Vishnio ReportsDigital WorldNo ratings yet
- ReportDocument12 pagesReportSimran jeet kaurNo ratings yet
- MR JoshanramDocument4 pagesMR JoshanrammuthurajctNo ratings yet
- 1-Comprehensive Silver Full Body Checkup - PO3444322131-391Document21 pages1-Comprehensive Silver Full Body Checkup - PO3444322131-391xiaomi giaNo ratings yet
- report-f84ffee37e97ca0bba01b28ead7ca1afd3000d5e (2)Document35 pagesreport-f84ffee37e97ca0bba01b28ead7ca1afd3000d5e (2)Amit JainNo ratings yet
- Report b2771712Document16 pagesReport b2771712Rishabh SinghNo ratings yet
- ReportDocument10 pagesReportAnkita GoyalNo ratings yet
- 1-Good Health Gold Package - PO3815496868-824Document19 pages1-Good Health Gold Package - PO3815496868-824mractiv8No ratings yet
- Report 6737931eDocument19 pagesReport 6737931eNeevinternational NeevNo ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- Mayur Mandraha 23103731Document5 pagesMayur Mandraha 23103731Eat Mode onNo ratings yet
- Name of Patient: Name of Patient: Name of Patient: Name of Patient: Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyaz Mrs. Nuzhat RiyazDocument9 pagesName of Patient: Name of Patient: Name of Patient: Name of Patient: Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyazgazal sharmaNo ratings yet
- 2023 03 15 Mr. ROSHAN-2Document2 pages2023 03 15 Mr. ROSHAN-2Sunny YadavNo ratings yet
- Report of Mr. RAJA PDFDocument3 pagesReport of Mr. RAJA PDFraja.tyagi2125No ratings yet
- Anjali Khapare - 23071171Document3 pagesAnjali Khapare - 23071171dr.menganeNo ratings yet
- Honey CBC Bio Elisa RiadDocument3 pagesHoney CBC Bio Elisa RiadMd.Monjurul IslamNo ratings yet
- HAEMATOLOGYDocument2 pagesHAEMATOLOGYParamita BeraNo ratings yet
- Test Name Result Biological Ref. Interval Method: 2.09 Mlu/L 0.46-4.68 CliaDocument5 pagesTest Name Result Biological Ref. Interval Method: 2.09 Mlu/L 0.46-4.68 CliaBhavnaNo ratings yet
- Report 89594e5fDocument10 pagesReport 89594e5fNaresh SrikakolapuNo ratings yet
- 1-Senior Citizen Basic Package - PO3248534977-432Document16 pages1-Senior Citizen Basic Package - PO3248534977-432Krishna Nand RaiNo ratings yet
- !null !null !6044 !makkah Medical Center !b300023 !salama Ibrahim Yousef !260524 !null !combinedreport !nullDocument3 pages!null !null !6044 !makkah Medical Center !b300023 !salama Ibrahim Yousef !260524 !null !combinedreport !nullYalla LudoNo ratings yet
- Complete Blood Picture (CBP), EDTA Whole Blood: Master - SushanthDocument3 pagesComplete Blood Picture (CBP), EDTA Whole Blood: Master - SushanthAbdul MuqeemNo ratings yet
- 1-Senior Citizen Advanced Package - PO3427386675-856Document18 pages1-Senior Citizen Advanced Package - PO3427386675-856Ravi PrakashNo ratings yet
- Prajwal AwasthiDocument3 pagesPrajwal AwasthiPrajjwal awasthiNo ratings yet
- DownloadDocument11 pagesDownloadDrGuptaaTvmNo ratings yet
- LabreportnewDocument16 pagesLabreportnewmirashaik3No ratings yet
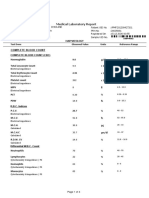
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- PdfText23 03 29T07490Document9 pagesPdfText23 03 29T07490Sudhir BhardwajNo ratings yet
- Juhi Shinde (871) 05.05.23Document6 pagesJuhi Shinde (871) 05.05.23Tushar ShindeNo ratings yet
- LabReport L14 Mrs - RAJESHWARI60YRS F 06 04 202420240406 2 E38fgDocument3 pagesLabReport L14 Mrs - RAJESHWARI60YRS F 06 04 202420240406 2 E38fgAnkit GairolaNo ratings yet
- Department of Laboratory: BiochemistryDocument3 pagesDepartment of Laboratory: Biochemistrymissarbz717No ratings yet
- LabTest 03jul2023Document5 pagesLabTest 03jul2023jkgupta0003No ratings yet
- 1-Glucose - Postprandial YOGESHDocument19 pages1-Glucose - Postprandial YOGESHMeet PatelNo ratings yet
- Report 400d0061Document18 pagesReport 400d0061Santosh BhandarkarNo ratings yet
- Lab - Report - BHAVISHKA JIDocument4 pagesLab - Report - BHAVISHKA JIYogeshKumarLoharNo ratings yet
- 240306743011M5 Avika Baweja 2 3 28 2024 8 50 51 AmDocument4 pages240306743011M5 Avika Baweja 2 3 28 2024 8 50 51 AmdrneerajpalsinghNo ratings yet
- PdfText - 2023-10-16T101203.851Document12 pagesPdfText - 2023-10-16T101203.851Sanjana AntilNo ratings yet
- Equine Clinical PathologyFrom EverandEquine Clinical PathologyRaquel M. WaltonNo ratings yet
- Gmail - Congratulation! We Are Scheduling Your Interview For The Role of CUSTOMER SERVICE EXECUTIVEDocument1 pageGmail - Congratulation! We Are Scheduling Your Interview For The Role of CUSTOMER SERVICE EXECUTIVERocky JNo ratings yet
- Horizontal Axis and Vertical Axis Wind TurbinesDocument3 pagesHorizontal Axis and Vertical Axis Wind TurbinesRocky JNo ratings yet
- MMMMDocument13 pagesMMMMRocky JNo ratings yet
- 2nd Merit List GCCDocument23 pages2nd Merit List GCCRocky JNo ratings yet
- All India Shri Shivaji Memorial Society's Polytechnic Kennedy Road, Near RTO, Pune - 411001Document11 pagesAll India Shri Shivaji Memorial Society's Polytechnic Kennedy Road, Near RTO, Pune - 411001Rocky JNo ratings yet
- ETM MCQ ALL - MCQ 479862600 ETM MCQ ALL - MCQDocument181 pagesETM MCQ ALL - MCQ 479862600 ETM MCQ ALL - MCQRocky JNo ratings yet
- PER 2015 NewDocument11 pagesPER 2015 NewRocky JNo ratings yet
- Advantages and Disadvantages of Hydraulic SystemDocument2 pagesAdvantages and Disadvantages of Hydraulic SystemRocky JNo ratings yet
- FINALDocument67 pagesFINALRocky JNo ratings yet
- Coverage Page For Black BookDocument2 pagesCoverage Page For Black BookRocky JNo ratings yet
- 2016 Winter Model Answer PaperDocument20 pages2016 Winter Model Answer PaperRocky JNo ratings yet
- Assignment No 1: Four Points)Document3 pagesAssignment No 1: Four Points)Rocky JNo ratings yet
- DATES of AEN & IEQDocument5 pagesDATES of AEN & IEQRocky JNo ratings yet
- Unit No. 04 - Quality Control and InspectionDocument198 pagesUnit No. 04 - Quality Control and InspectionRocky JNo ratings yet
- Payment ProcesDocument8 pagesPayment ProcesRocky JNo ratings yet
- ETM Question BankDocument225 pagesETM Question BankRocky JNo ratings yet
- CERTIFICATEDocument1 pageCERTIFICATERocky JNo ratings yet
- Information On Control Systems: Cascades Stream Temperature Control SystemDocument2 pagesInformation On Control Systems: Cascades Stream Temperature Control SystemRocky JNo ratings yet
- Sudject: Defence Studies: Roll No: 38 Division:Jasmine Std:IxDocument14 pagesSudject: Defence Studies: Roll No: 38 Division:Jasmine Std:IxRocky JNo ratings yet
- Analysis On Explanation TextDocument2 pagesAnalysis On Explanation Textasih dwi astutiNo ratings yet
- Promotion Letter ShwetaDocument2 pagesPromotion Letter ShwetayogeshNo ratings yet
- Toothpaste Survey FormDocument1 pageToothpaste Survey FormBimalendu Konar50% (2)
- Vespa S 125 3V Ie 150 3V Ie UPUTSTVODocument90 pagesVespa S 125 3V Ie 150 3V Ie UPUTSTVOdoughstoneNo ratings yet
- Class 11 English Notes Studyguide360Document272 pagesClass 11 English Notes Studyguide360IsnatainiNo ratings yet
- Cylone - Lab Report - FinalizeDocument19 pagesCylone - Lab Report - FinalizeSiti Khairunnur LaderlahNo ratings yet
- Planning and Facilities: Building StorageDocument31 pagesPlanning and Facilities: Building Storagequsai migdadiNo ratings yet
- Iec Inverse Protection CurvesDocument1 pageIec Inverse Protection CurvesEng-Ahmad Abo-AledousNo ratings yet
- The Development of A Heat Wave Vulnerability Index For London-2013Document10 pagesThe Development of A Heat Wave Vulnerability Index For London-2013gilberto777No ratings yet
- Workload ManagementDocument25 pagesWorkload Managementdex adecNo ratings yet
- Acceptance Criteria of Weld Defects As Per Different CodesDocument17 pagesAcceptance Criteria of Weld Defects As Per Different CodesMidhun K Chandrabose96% (25)
- Social Studies jss2 First Term EXAMSDocument5 pagesSocial Studies jss2 First Term EXAMSalmightyfavouriteNo ratings yet
- Discard ManagementDocument9 pagesDiscard ManagementDevvrath SinghNo ratings yet
- Department of Education: Learning Activity SheetDocument7 pagesDepartment of Education: Learning Activity SheetKaren May UrlandaNo ratings yet
- It's A Safe World After All : TÜV FS EngineerDocument5 pagesIt's A Safe World After All : TÜV FS Engineerizadi1979No ratings yet
- Barcode v1Document31 pagesBarcode v1Desinta OctavianiNo ratings yet
- Hospital Management System: Dept. of CSE, GECRDocument30 pagesHospital Management System: Dept. of CSE, GECRYounus KhanNo ratings yet
- Dokumen - Tips - Diagnostic Test Mapeh 10Document4 pagesDokumen - Tips - Diagnostic Test Mapeh 10charry ruayaNo ratings yet
- Science G7 Q2 LP4Document13 pagesScience G7 Q2 LP4Lovely GuintoNo ratings yet
- CCO HandbookDocument44 pagesCCO HandbookVenkata Suresh MandavaNo ratings yet
- Model: Stored Energy Solutions For A Demanding World: Dimensions MM InchDocument2 pagesModel: Stored Energy Solutions For A Demanding World: Dimensions MM Incheddywidjaya9No ratings yet
- Automatic Control Basic Course: Exercises 2021Document124 pagesAutomatic Control Basic Course: Exercises 2021Duc-Duy Pham NguyenNo ratings yet
- SDS Hardener 2750 EN 221004Document10 pagesSDS Hardener 2750 EN 221004juprykaNo ratings yet
- Case Study On A Highway Project: Environmental Impact AssesmentDocument10 pagesCase Study On A Highway Project: Environmental Impact AssesmentSRUTHI FRANCIS M.Tech Environmental Engineering 2020-2022No ratings yet
- Dec. 4 2021 Bldg. Tech ReviewDocument58 pagesDec. 4 2021 Bldg. Tech Reviewadyjoy antonioNo ratings yet
- On Light: Science Holiday Homework Made By-Aish Mishra Class-8 Diamond Roll No.-6Document9 pagesOn Light: Science Holiday Homework Made By-Aish Mishra Class-8 Diamond Roll No.-6Ansh MishraNo ratings yet
- Waste Heat RecoveryDocument37 pagesWaste Heat Recoveryommech2020No ratings yet










































































































Download as pdf or txt
You might also like
- Pass Nclex IN 30 DAYS!Document9 pagesPass Nclex IN 30 DAYS!Jude olga75% (4)
- Computer System Validation Risk Assessment ToolDocument3 pagesComputer System Validation Risk Assessment Toolcpkakope100% (1)
- Vegan AestheticsDocument12 pagesVegan AestheticselyseNo ratings yet
- 1-Complete Blood Count - PO1106326185-399Document8 pages1-Complete Blood Count - PO1106326185-399Arup KumarNo ratings yet
- Po4009507960 540Document15 pagesPo4009507960 540PRADEEP KUMARNo ratings yet
- 1-Good Health Premium Package - PO1065281239-651Document19 pages1-Good Health Premium Package - PO1065281239-651Renu ChoudharyNo ratings yet
- Kidney FunctionDocument19 pagesKidney FunctionFarooq Bin MahfoozNo ratings yet
- DR. Neelanjana SHARMADocument5 pagesDR. Neelanjana SHARMADr. Neelanjana SharmaNo ratings yet
- Report 831a66a7 PDFDocument23 pagesReport 831a66a7 PDFViral PatelNo ratings yet
- Devendra - 2401611Document3 pagesDevendra - 2401611arslansiddique406No ratings yet
- agilius report_unlockedDocument8 pagesagilius report_unlockedSucharit NarangNo ratings yet
- Health Report 2023Document30 pagesHealth Report 2023Pranay GuptaNo ratings yet
- Don't Know Love - 1004584Document14 pagesDon't Know Love - 1004584baapj39No ratings yet
- 1-Women Wellness Premium Package_PO1180038496-860Document22 pages1-Women Wellness Premium Package_PO1180038496-860sttt13331No ratings yet
- Lab Report NewDocument5 pagesLab Report Newsamirghosal19No ratings yet
- Mr. Abhijeet BhoyarDocument9 pagesMr. Abhijeet BhoyarMahesh TilanteNo ratings yet
- Hematology: Test Name Result Reference Range Unit SpecimenDocument4 pagesHematology: Test Name Result Reference Range Unit Specimennirmala.arunanNo ratings yet
- Final: Code/Name & AddressDocument6 pagesFinal: Code/Name & AddresscrypticgarvNo ratings yet
- Comprehensive body lab reportDocument18 pagesComprehensive body lab reportTanvi PunjabiNo ratings yet
- 0056XF00339756_980475vDocument10 pages0056XF00339756_980475vAjay YadavNo ratings yet
- Checkup ReportDocument17 pagesCheckup Reportshashwatpandey736No ratings yet
- Report F412b1a3Document18 pagesReport F412b1a3055Nitish BhatiaNo ratings yet
- BloodDocument18 pagesBloodPriyanshu GuptaNo ratings yet
- Sangeeta Vishnio ReportsDocument13 pagesSangeeta Vishnio ReportsDigital WorldNo ratings yet
- ReportDocument12 pagesReportSimran jeet kaurNo ratings yet
- MR JoshanramDocument4 pagesMR JoshanrammuthurajctNo ratings yet
- 1-Comprehensive Silver Full Body Checkup - PO3444322131-391Document21 pages1-Comprehensive Silver Full Body Checkup - PO3444322131-391xiaomi giaNo ratings yet
- report-f84ffee37e97ca0bba01b28ead7ca1afd3000d5e (2)Document35 pagesreport-f84ffee37e97ca0bba01b28ead7ca1afd3000d5e (2)Amit JainNo ratings yet
- Report b2771712Document16 pagesReport b2771712Rishabh SinghNo ratings yet
- ReportDocument10 pagesReportAnkita GoyalNo ratings yet
- 1-Good Health Gold Package - PO3815496868-824Document19 pages1-Good Health Gold Package - PO3815496868-824mractiv8No ratings yet
- Report 6737931eDocument19 pagesReport 6737931eNeevinternational NeevNo ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- Hematology: KongamdanaDocument1 pageHematology: KongamdanaShariqNo ratings yet
- Mayur Mandraha 23103731Document5 pagesMayur Mandraha 23103731Eat Mode onNo ratings yet
- Name of Patient: Name of Patient: Name of Patient: Name of Patient: Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyaz Mrs. Nuzhat RiyazDocument9 pagesName of Patient: Name of Patient: Name of Patient: Name of Patient: Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyaz Mrs. Nuzhat Riyazgazal sharmaNo ratings yet
- 2023 03 15 Mr. ROSHAN-2Document2 pages2023 03 15 Mr. ROSHAN-2Sunny YadavNo ratings yet
- Report of Mr. RAJA PDFDocument3 pagesReport of Mr. RAJA PDFraja.tyagi2125No ratings yet
- Anjali Khapare - 23071171Document3 pagesAnjali Khapare - 23071171dr.menganeNo ratings yet
- Honey CBC Bio Elisa RiadDocument3 pagesHoney CBC Bio Elisa RiadMd.Monjurul IslamNo ratings yet
- HAEMATOLOGYDocument2 pagesHAEMATOLOGYParamita BeraNo ratings yet
- Test Name Result Biological Ref. Interval Method: 2.09 Mlu/L 0.46-4.68 CliaDocument5 pagesTest Name Result Biological Ref. Interval Method: 2.09 Mlu/L 0.46-4.68 CliaBhavnaNo ratings yet
- Report 89594e5fDocument10 pagesReport 89594e5fNaresh SrikakolapuNo ratings yet
- 1-Senior Citizen Basic Package - PO3248534977-432Document16 pages1-Senior Citizen Basic Package - PO3248534977-432Krishna Nand RaiNo ratings yet
- !null !null !6044 !makkah Medical Center !b300023 !salama Ibrahim Yousef !260524 !null !combinedreport !nullDocument3 pages!null !null !6044 !makkah Medical Center !b300023 !salama Ibrahim Yousef !260524 !null !combinedreport !nullYalla LudoNo ratings yet
- Complete Blood Picture (CBP), EDTA Whole Blood: Master - SushanthDocument3 pagesComplete Blood Picture (CBP), EDTA Whole Blood: Master - SushanthAbdul MuqeemNo ratings yet
- 1-Senior Citizen Advanced Package - PO3427386675-856Document18 pages1-Senior Citizen Advanced Package - PO3427386675-856Ravi PrakashNo ratings yet
- Prajwal AwasthiDocument3 pagesPrajwal AwasthiPrajjwal awasthiNo ratings yet
- DownloadDocument11 pagesDownloadDrGuptaaTvmNo ratings yet
- LabreportnewDocument16 pagesLabreportnewmirashaik3No ratings yet
- Medical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWDocument4 pagesMedical Laboratory Report: Haemoglobin Total Leucocyte Count Total Erythrocyte Count Platelet Count MPV PCT PDWdhavalNo ratings yet
- PdfText23 03 29T07490Document9 pagesPdfText23 03 29T07490Sudhir BhardwajNo ratings yet
- Juhi Shinde (871) 05.05.23Document6 pagesJuhi Shinde (871) 05.05.23Tushar ShindeNo ratings yet
- LabReport L14 Mrs - RAJESHWARI60YRS F 06 04 202420240406 2 E38fgDocument3 pagesLabReport L14 Mrs - RAJESHWARI60YRS F 06 04 202420240406 2 E38fgAnkit GairolaNo ratings yet
- Department of Laboratory: BiochemistryDocument3 pagesDepartment of Laboratory: Biochemistrymissarbz717No ratings yet
- LabTest 03jul2023Document5 pagesLabTest 03jul2023jkgupta0003No ratings yet
- 1-Glucose - Postprandial YOGESHDocument19 pages1-Glucose - Postprandial YOGESHMeet PatelNo ratings yet
- Report 400d0061Document18 pagesReport 400d0061Santosh BhandarkarNo ratings yet
- Lab - Report - BHAVISHKA JIDocument4 pagesLab - Report - BHAVISHKA JIYogeshKumarLoharNo ratings yet
- 240306743011M5 Avika Baweja 2 3 28 2024 8 50 51 AmDocument4 pages240306743011M5 Avika Baweja 2 3 28 2024 8 50 51 AmdrneerajpalsinghNo ratings yet
- PdfText - 2023-10-16T101203.851Document12 pagesPdfText - 2023-10-16T101203.851Sanjana AntilNo ratings yet
- Equine Clinical PathologyFrom EverandEquine Clinical PathologyRaquel M. WaltonNo ratings yet
- Gmail - Congratulation! We Are Scheduling Your Interview For The Role of CUSTOMER SERVICE EXECUTIVEDocument1 pageGmail - Congratulation! We Are Scheduling Your Interview For The Role of CUSTOMER SERVICE EXECUTIVERocky JNo ratings yet
- Horizontal Axis and Vertical Axis Wind TurbinesDocument3 pagesHorizontal Axis and Vertical Axis Wind TurbinesRocky JNo ratings yet
- MMMMDocument13 pagesMMMMRocky JNo ratings yet
- 2nd Merit List GCCDocument23 pages2nd Merit List GCCRocky JNo ratings yet
- All India Shri Shivaji Memorial Society's Polytechnic Kennedy Road, Near RTO, Pune - 411001Document11 pagesAll India Shri Shivaji Memorial Society's Polytechnic Kennedy Road, Near RTO, Pune - 411001Rocky JNo ratings yet
- ETM MCQ ALL - MCQ 479862600 ETM MCQ ALL - MCQDocument181 pagesETM MCQ ALL - MCQ 479862600 ETM MCQ ALL - MCQRocky JNo ratings yet
- PER 2015 NewDocument11 pagesPER 2015 NewRocky JNo ratings yet
- Advantages and Disadvantages of Hydraulic SystemDocument2 pagesAdvantages and Disadvantages of Hydraulic SystemRocky JNo ratings yet
- FINALDocument67 pagesFINALRocky JNo ratings yet
- Coverage Page For Black BookDocument2 pagesCoverage Page For Black BookRocky JNo ratings yet
- 2016 Winter Model Answer PaperDocument20 pages2016 Winter Model Answer PaperRocky JNo ratings yet
- Assignment No 1: Four Points)Document3 pagesAssignment No 1: Four Points)Rocky JNo ratings yet
- DATES of AEN & IEQDocument5 pagesDATES of AEN & IEQRocky JNo ratings yet
- Unit No. 04 - Quality Control and InspectionDocument198 pagesUnit No. 04 - Quality Control and InspectionRocky JNo ratings yet
- Payment ProcesDocument8 pagesPayment ProcesRocky JNo ratings yet
- ETM Question BankDocument225 pagesETM Question BankRocky JNo ratings yet
- CERTIFICATEDocument1 pageCERTIFICATERocky JNo ratings yet
- Information On Control Systems: Cascades Stream Temperature Control SystemDocument2 pagesInformation On Control Systems: Cascades Stream Temperature Control SystemRocky JNo ratings yet
- Sudject: Defence Studies: Roll No: 38 Division:Jasmine Std:IxDocument14 pagesSudject: Defence Studies: Roll No: 38 Division:Jasmine Std:IxRocky JNo ratings yet
- Analysis On Explanation TextDocument2 pagesAnalysis On Explanation Textasih dwi astutiNo ratings yet
- Promotion Letter ShwetaDocument2 pagesPromotion Letter ShwetayogeshNo ratings yet
- Toothpaste Survey FormDocument1 pageToothpaste Survey FormBimalendu Konar50% (2)
- Vespa S 125 3V Ie 150 3V Ie UPUTSTVODocument90 pagesVespa S 125 3V Ie 150 3V Ie UPUTSTVOdoughstoneNo ratings yet
- Class 11 English Notes Studyguide360Document272 pagesClass 11 English Notes Studyguide360IsnatainiNo ratings yet
- Cylone - Lab Report - FinalizeDocument19 pagesCylone - Lab Report - FinalizeSiti Khairunnur LaderlahNo ratings yet
- Planning and Facilities: Building StorageDocument31 pagesPlanning and Facilities: Building Storagequsai migdadiNo ratings yet
- Iec Inverse Protection CurvesDocument1 pageIec Inverse Protection CurvesEng-Ahmad Abo-AledousNo ratings yet
- The Development of A Heat Wave Vulnerability Index For London-2013Document10 pagesThe Development of A Heat Wave Vulnerability Index For London-2013gilberto777No ratings yet
- Workload ManagementDocument25 pagesWorkload Managementdex adecNo ratings yet
- Acceptance Criteria of Weld Defects As Per Different CodesDocument17 pagesAcceptance Criteria of Weld Defects As Per Different CodesMidhun K Chandrabose96% (25)
- Social Studies jss2 First Term EXAMSDocument5 pagesSocial Studies jss2 First Term EXAMSalmightyfavouriteNo ratings yet
- Discard ManagementDocument9 pagesDiscard ManagementDevvrath SinghNo ratings yet
- Department of Education: Learning Activity SheetDocument7 pagesDepartment of Education: Learning Activity SheetKaren May UrlandaNo ratings yet
- It's A Safe World After All : TÜV FS EngineerDocument5 pagesIt's A Safe World After All : TÜV FS Engineerizadi1979No ratings yet
- Barcode v1Document31 pagesBarcode v1Desinta OctavianiNo ratings yet
- Hospital Management System: Dept. of CSE, GECRDocument30 pagesHospital Management System: Dept. of CSE, GECRYounus KhanNo ratings yet
- Dokumen - Tips - Diagnostic Test Mapeh 10Document4 pagesDokumen - Tips - Diagnostic Test Mapeh 10charry ruayaNo ratings yet
- Science G7 Q2 LP4Document13 pagesScience G7 Q2 LP4Lovely GuintoNo ratings yet
- CCO HandbookDocument44 pagesCCO HandbookVenkata Suresh MandavaNo ratings yet
- Model: Stored Energy Solutions For A Demanding World: Dimensions MM InchDocument2 pagesModel: Stored Energy Solutions For A Demanding World: Dimensions MM Incheddywidjaya9No ratings yet
- Automatic Control Basic Course: Exercises 2021Document124 pagesAutomatic Control Basic Course: Exercises 2021Duc-Duy Pham NguyenNo ratings yet
- SDS Hardener 2750 EN 221004Document10 pagesSDS Hardener 2750 EN 221004juprykaNo ratings yet
- Case Study On A Highway Project: Environmental Impact AssesmentDocument10 pagesCase Study On A Highway Project: Environmental Impact AssesmentSRUTHI FRANCIS M.Tech Environmental Engineering 2020-2022No ratings yet
- Dec. 4 2021 Bldg. Tech ReviewDocument58 pagesDec. 4 2021 Bldg. Tech Reviewadyjoy antonioNo ratings yet
- On Light: Science Holiday Homework Made By-Aish Mishra Class-8 Diamond Roll No.-6Document9 pagesOn Light: Science Holiday Homework Made By-Aish Mishra Class-8 Diamond Roll No.-6Ansh MishraNo ratings yet
- Waste Heat RecoveryDocument37 pagesWaste Heat Recoveryommech2020No ratings yet