
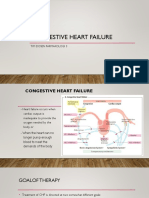
Congestive Cardiac Failure
Congestive Cardiac Failure
You might also like
- Occupational Therapy Assessments Quick TableDocument5 pagesOccupational Therapy Assessments Quick Tableredsmartie100% (3)
- Pharma ExamDocument5 pagesPharma ExamMclavin LoveNo ratings yet
- Medical Israeli Syllabus For Internal Medicine For Exam LicenseDocument4 pagesMedical Israeli Syllabus For Internal Medicine For Exam Licensemohammadeid0% (2)
- Congestive Cardiac FailureDocument27 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Drugs Used in Heart FailureDocument27 pagesDrugs Used in Heart Failurealeah morenoNo ratings yet
- Antianginal and Antiischemic DrugsDocument18 pagesAntianginal and Antiischemic DrugsNaveen KumarNo ratings yet
- Lec 2 Heart Failure, Angina and Arryth2Document19 pagesLec 2 Heart Failure, Angina and Arryth2Adel AlomarNo ratings yet
- Pharmacology ReviewersDocument5 pagesPharmacology ReviewersNeisha Halil VillarealNo ratings yet
- Pharmacology ReviersDocument5 pagesPharmacology ReviersNeisha Halil VillarealNo ratings yet
- Pharmacology IIDocument178 pagesPharmacology IIMelanieNo ratings yet
- Cardiovascular Drugs (Veterinary Pharmacology)Document44 pagesCardiovascular Drugs (Veterinary Pharmacology)DR Muhammad Abdul BasitNo ratings yet
- Anti - ArrhythmicsDocument5 pagesAnti - ArrhythmicsAnabeth F. PungtilanNo ratings yet
- Asist. Lecturer Hasan Adnan Hashim Msc. Pharmacology and ToxicologyDocument52 pagesAsist. Lecturer Hasan Adnan Hashim Msc. Pharmacology and Toxicologyمصطفى ابراهيم سعيدNo ratings yet
- Drugs For Ischemic Heart DiseaseDocument44 pagesDrugs For Ischemic Heart DiseaseMbah GapinbissiNo ratings yet
- Modul Drugs Used in Congestive Heart Failure 11 Nov 2010Document12 pagesModul Drugs Used in Congestive Heart Failure 11 Nov 2010Dian NugraNo ratings yet
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
- Lecture13-Congestive Heart Failure DrugsDocument48 pagesLecture13-Congestive Heart Failure Drugsharis.18No ratings yet
- 1.CVS DrugsDocument98 pages1.CVS DrugsHarshika KDGNo ratings yet
- Cardiovascular System 2Document8 pagesCardiovascular System 2محمد علي حميدNo ratings yet
- Heart Failure and Antidysrhythmic DrugsDocument38 pagesHeart Failure and Antidysrhythmic DrugsYza Belle RamoNo ratings yet
- Congestive Heart FailureDocument30 pagesCongestive Heart FailurePh OmarNo ratings yet
- Drugs Used in HF IIDocument40 pagesDrugs Used in HF IIJamal LudinNo ratings yet
- Drugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3Document47 pagesDrugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3DR Muhammad Abdul BasitNo ratings yet
- Cardiac Failure: by Dr. Osman BukhariDocument48 pagesCardiac Failure: by Dr. Osman BukhariIrfandy Chairi Sulaiman LubisNo ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- Heat Failure DrugsDocument8 pagesHeat Failure DrugsDaniel MwiluNo ratings yet
- Drugs For Congestive Heart FailureDocument46 pagesDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- Toxicology Lecture 6 Medical Toxicology (Chapter 4)Document22 pagesToxicology Lecture 6 Medical Toxicology (Chapter 4)Hasan iimanNo ratings yet
- 10-11 Treatment of HypertensionDocument11 pages10-11 Treatment of HypertensionHanif GandohNo ratings yet
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 pagesAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdNo ratings yet
- Heart AttackDocument36 pagesHeart AttackAngela TibigarNo ratings yet
- 4 - Anti-AnginaDocument6 pages4 - Anti-AnginaJericho De GuzmanNo ratings yet
- 5-Heart FailureDocument12 pages5-Heart FailureJericho De GuzmanNo ratings yet
- Antihypertensive AgentsDocument52 pagesAntihypertensive Agentssameena ramzanNo ratings yet
- Heart Failure TutorialDocument1 pageHeart Failure TutorialAbdul MosheenNo ratings yet
- Arrhythmia 2Document31 pagesArrhythmia 2rittvedNo ratings yet
- Drugs Used in The Treatment of Cardiac Failure: Assoc. Prof. Iv. Lambev WWW - Medpharm-Sofia - EuDocument38 pagesDrugs Used in The Treatment of Cardiac Failure: Assoc. Prof. Iv. Lambev WWW - Medpharm-Sofia - EuYeshaa MiraniNo ratings yet
- Pharma of Heart FailureDocument12 pagesPharma of Heart FailureBaqir BroNo ratings yet
- Pharmacology Chapter 42 p-3Document19 pagesPharmacology Chapter 42 p-3sho bartNo ratings yet
- Cardiac PharmDocument6 pagesCardiac PharmJohn SmithNo ratings yet
- CONGESTIVE HEART FAILURE - New-1Document32 pagesCONGESTIVE HEART FAILURE - New-1Agus SuprionoNo ratings yet
- 2.drugsusedforthetreatmentofmi 121112230936 Phpapp02Document38 pages2.drugsusedforthetreatmentofmi 121112230936 Phpapp02omar khanNo ratings yet
- Cardio Pharma MeDocument23 pagesCardio Pharma Memohammed.sheeb.yesNo ratings yet
- Cardio CHF Angina Drugs MegDocument3 pagesCardio CHF Angina Drugs MegJhonny pingolNo ratings yet
- Cad CommerDocument2 pagesCad CommerWhatDoYouSeriesNo ratings yet
- Drugs Acting On Cardio Vascular SystemDocument16 pagesDrugs Acting On Cardio Vascular SystemANUSHYA B PSGRKCWNo ratings yet
- Wesam R KadhumDocument31 pagesWesam R Kadhumwisam_1by1No ratings yet
- 13.angina and Anti-Anginal DrugsDocument60 pages13.angina and Anti-Anginal Drugsbilalsiddique5365No ratings yet
- Antiarrhythmic Drugs FinalDocument31 pagesAntiarrhythmic Drugs FinalAmanuel Maru50% (2)
- Lec.5 Drugs For Heart FailureDocument19 pagesLec.5 Drugs For Heart FailureAbuzar DawarNo ratings yet
- CHFDocument11 pagesCHFGwendolyn Talahiban LusaraNo ratings yet
- Some Important Points To RememberDocument3 pagesSome Important Points To RememberTaman HoangNo ratings yet
- Lec 3 Heart FailureDocument25 pagesLec 3 Heart FailureDelete AccountNo ratings yet
- Beta Blockers and Calcium Channel BlockersDocument34 pagesBeta Blockers and Calcium Channel Blockersnevena.stankovic986No ratings yet
- Cholinergic System: e CarbamatesDocument26 pagesCholinergic System: e CarbamatesAcai BoncaiNo ratings yet
- Drugs Affecting The Cardiovascular SystemDocument70 pagesDrugs Affecting The Cardiovascular SystemRayne Bonifacio100% (2)
- What Are The Toxicities of Amiodarone?: CardiologyDocument33 pagesWhat Are The Toxicities of Amiodarone?: Cardiologylakshminivas PingaliNo ratings yet
- Pharmacotherapy of Congestive Heart Failure (CHF)Document163 pagesPharmacotherapy of Congestive Heart Failure (CHF)Aditya rathoreNo ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- Congestive Heart FailureDocument17 pagesCongestive Heart FailureLyana StarkNo ratings yet
- Heart Failure New SlidesDocument41 pagesHeart Failure New SlidesjawadNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Causality Assessment of ADRsDocument45 pagesCausality Assessment of ADRsKrupasagar Pn PalegarNo ratings yet
- Congestive Cardiac FailureDocument27 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Antiprotozoal DrugsDocument46 pagesAntiprotozoal DrugsKrupasagar Pn PalegarNo ratings yet
- Anti InflammatoryDocument20 pagesAnti InflammatoryKrupasagar Pn PalegarNo ratings yet
- AceclofenacDocument17 pagesAceclofenacKrupasagar Pn PalegarNo ratings yet
- BMJ 2022 074216.fullDocument20 pagesBMJ 2022 074216.fullArmando OrtegaNo ratings yet
- Alzheimers-Disease-Genetics-Fact-Sheet 0Document8 pagesAlzheimers-Disease-Genetics-Fact-Sheet 0api-285676076No ratings yet
- Diagnosis of Anaplastic Thyroid Carcinoma On Fine Needle Aspiration Cytology - A Rare Case ReportDocument5 pagesDiagnosis of Anaplastic Thyroid Carcinoma On Fine Needle Aspiration Cytology - A Rare Case ReportEditor_IAIMNo ratings yet
- Severe Dapsone Hypersensitivity Syndrome: Case ReportDocument3 pagesSevere Dapsone Hypersensitivity Syndrome: Case ReportFlorencia PalimbongNo ratings yet
- 6 - Physiology MCQ of General PhysiologyDocument20 pages6 - Physiology MCQ of General PhysiologymohammedNo ratings yet
- Dementia & Alzheimer's Care: Planning and Preparing For The Road AheadDocument14 pagesDementia & Alzheimer's Care: Planning and Preparing For The Road AheadblurrmieNo ratings yet
- 12 Cranial NervesDocument21 pages12 Cranial Nerveseha_9213423No ratings yet
- Amikacin Drug StudyDocument2 pagesAmikacin Drug StudyRussel Kate SulangNo ratings yet
- Otalgia & TinnitusDocument19 pagesOtalgia & Tinnitushonda matizNo ratings yet
- Neuropathology of Epilepsy: Epilepsy-Related Deaths and SUDEPDocument11 pagesNeuropathology of Epilepsy: Epilepsy-Related Deaths and SUDEPTeuku AvicennaNo ratings yet
- Mesenteric Venous Thrombosis 2Document5 pagesMesenteric Venous Thrombosis 2cbnhvpqpgrNo ratings yet
- Bacterial Vaginosis: A Synthesis of The Literature On Etiology, Prevalence, Risk Factors, and Relationship With Chlamydia and Gonorrhea InfectionsDocument10 pagesBacterial Vaginosis: A Synthesis of The Literature On Etiology, Prevalence, Risk Factors, and Relationship With Chlamydia and Gonorrhea InfectionsElison J PanggaloNo ratings yet
- Respiratory and CardiovascularDocument133 pagesRespiratory and CardiovascularHawraa FadhilNo ratings yet
- Thoracic PainDocument36 pagesThoracic PainLuciana ThioNo ratings yet
- Pharmacology Scheme 3rd Prof - by Hafiz Muhammad Attaullah & Aqib RazzaqDocument39 pagesPharmacology Scheme 3rd Prof - by Hafiz Muhammad Attaullah & Aqib Razzaqpham.chopraNo ratings yet
- Enucleation in Companion Animals Feb 2008 Ivj PDFDocument6 pagesEnucleation in Companion Animals Feb 2008 Ivj PDFZayna QhastalaniNo ratings yet
- DNS ENT Case Write UpDocument8 pagesDNS ENT Case Write UpShafiq ZahariNo ratings yet
- Qstream-1 2Document55 pagesQstream-1 2Vijay100% (1)
- Tolvaptan-Drug StudyDocument1 pageTolvaptan-Drug Studykaycelyn jimenez100% (2)
- Addison's DiseaseDocument4 pagesAddison's DiseasedrtpkNo ratings yet
- Translate Acute Mesenteric IschemiaDocument13 pagesTranslate Acute Mesenteric IschemiaFadhli Aufar KasyfiNo ratings yet
- Liver, Biliary Tract and Pancreas PathologyDocument50 pagesLiver, Biliary Tract and Pancreas PathologybonadnadineNo ratings yet
- Cardiacassessmentppt 170323092148Document48 pagesCardiacassessmentppt 170323092148sasNo ratings yet
- Free Radicals and AmaDocument5 pagesFree Radicals and AmaOlga RodriguesNo ratings yet
- Biomedicine & Pharmacotherapy: ReviewDocument14 pagesBiomedicine & Pharmacotherapy: Reviewmr dexterNo ratings yet
- Amiodarone Atrial Fibrillation BerberinDocument10 pagesAmiodarone Atrial Fibrillation Berberinharold jitschak bueno de mesquitaNo ratings yet
- Uswatun Hasanah-195037-2a Rmik (KKPMT)Document4 pagesUswatun Hasanah-195037-2a Rmik (KKPMT)Uswatun HasanahNo ratings yet
- Case 2 Hydrocephalus Group 4Document27 pagesCase 2 Hydrocephalus Group 4younggirldavidNo ratings yet




























































































Download as pdf or txt
You might also like
- Occupational Therapy Assessments Quick TableDocument5 pagesOccupational Therapy Assessments Quick Tableredsmartie100% (3)
- Pharma ExamDocument5 pagesPharma ExamMclavin LoveNo ratings yet
- Medical Israeli Syllabus For Internal Medicine For Exam LicenseDocument4 pagesMedical Israeli Syllabus For Internal Medicine For Exam Licensemohammadeid0% (2)
- Congestive Cardiac FailureDocument27 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Drugs Used in Heart FailureDocument27 pagesDrugs Used in Heart Failurealeah morenoNo ratings yet
- Antianginal and Antiischemic DrugsDocument18 pagesAntianginal and Antiischemic DrugsNaveen KumarNo ratings yet
- Lec 2 Heart Failure, Angina and Arryth2Document19 pagesLec 2 Heart Failure, Angina and Arryth2Adel AlomarNo ratings yet
- Pharmacology ReviewersDocument5 pagesPharmacology ReviewersNeisha Halil VillarealNo ratings yet
- Pharmacology ReviersDocument5 pagesPharmacology ReviersNeisha Halil VillarealNo ratings yet
- Pharmacology IIDocument178 pagesPharmacology IIMelanieNo ratings yet
- Cardiovascular Drugs (Veterinary Pharmacology)Document44 pagesCardiovascular Drugs (Veterinary Pharmacology)DR Muhammad Abdul BasitNo ratings yet
- Anti - ArrhythmicsDocument5 pagesAnti - ArrhythmicsAnabeth F. PungtilanNo ratings yet
- Asist. Lecturer Hasan Adnan Hashim Msc. Pharmacology and ToxicologyDocument52 pagesAsist. Lecturer Hasan Adnan Hashim Msc. Pharmacology and Toxicologyمصطفى ابراهيم سعيدNo ratings yet
- Drugs For Ischemic Heart DiseaseDocument44 pagesDrugs For Ischemic Heart DiseaseMbah GapinbissiNo ratings yet
- Modul Drugs Used in Congestive Heart Failure 11 Nov 2010Document12 pagesModul Drugs Used in Congestive Heart Failure 11 Nov 2010Dian NugraNo ratings yet
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
- Lecture13-Congestive Heart Failure DrugsDocument48 pagesLecture13-Congestive Heart Failure Drugsharis.18No ratings yet
- 1.CVS DrugsDocument98 pages1.CVS DrugsHarshika KDGNo ratings yet
- Cardiovascular System 2Document8 pagesCardiovascular System 2محمد علي حميدNo ratings yet
- Heart Failure and Antidysrhythmic DrugsDocument38 pagesHeart Failure and Antidysrhythmic DrugsYza Belle RamoNo ratings yet
- Congestive Heart FailureDocument30 pagesCongestive Heart FailurePh OmarNo ratings yet
- Drugs Used in HF IIDocument40 pagesDrugs Used in HF IIJamal LudinNo ratings yet
- Drugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3Document47 pagesDrugs For Heart Failure & Angina: Department of Pharmacology Liming Zhou 2010,3DR Muhammad Abdul BasitNo ratings yet
- Cardiac Failure: by Dr. Osman BukhariDocument48 pagesCardiac Failure: by Dr. Osman BukhariIrfandy Chairi Sulaiman LubisNo ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- Heat Failure DrugsDocument8 pagesHeat Failure DrugsDaniel MwiluNo ratings yet
- Drugs For Congestive Heart FailureDocument46 pagesDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- Toxicology Lecture 6 Medical Toxicology (Chapter 4)Document22 pagesToxicology Lecture 6 Medical Toxicology (Chapter 4)Hasan iimanNo ratings yet
- 10-11 Treatment of HypertensionDocument11 pages10-11 Treatment of HypertensionHanif GandohNo ratings yet
- Anti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistDocument25 pagesAnti-Anginal and Antiischemic Drugs: Dr. Pradeepa H D Clinical PharmacologistpradeephdNo ratings yet
- Heart AttackDocument36 pagesHeart AttackAngela TibigarNo ratings yet
- 4 - Anti-AnginaDocument6 pages4 - Anti-AnginaJericho De GuzmanNo ratings yet
- 5-Heart FailureDocument12 pages5-Heart FailureJericho De GuzmanNo ratings yet
- Antihypertensive AgentsDocument52 pagesAntihypertensive Agentssameena ramzanNo ratings yet
- Heart Failure TutorialDocument1 pageHeart Failure TutorialAbdul MosheenNo ratings yet
- Arrhythmia 2Document31 pagesArrhythmia 2rittvedNo ratings yet
- Drugs Used in The Treatment of Cardiac Failure: Assoc. Prof. Iv. Lambev WWW - Medpharm-Sofia - EuDocument38 pagesDrugs Used in The Treatment of Cardiac Failure: Assoc. Prof. Iv. Lambev WWW - Medpharm-Sofia - EuYeshaa MiraniNo ratings yet
- Pharma of Heart FailureDocument12 pagesPharma of Heart FailureBaqir BroNo ratings yet
- Pharmacology Chapter 42 p-3Document19 pagesPharmacology Chapter 42 p-3sho bartNo ratings yet
- Cardiac PharmDocument6 pagesCardiac PharmJohn SmithNo ratings yet
- CONGESTIVE HEART FAILURE - New-1Document32 pagesCONGESTIVE HEART FAILURE - New-1Agus SuprionoNo ratings yet
- 2.drugsusedforthetreatmentofmi 121112230936 Phpapp02Document38 pages2.drugsusedforthetreatmentofmi 121112230936 Phpapp02omar khanNo ratings yet
- Cardio Pharma MeDocument23 pagesCardio Pharma Memohammed.sheeb.yesNo ratings yet
- Cardio CHF Angina Drugs MegDocument3 pagesCardio CHF Angina Drugs MegJhonny pingolNo ratings yet
- Cad CommerDocument2 pagesCad CommerWhatDoYouSeriesNo ratings yet
- Drugs Acting On Cardio Vascular SystemDocument16 pagesDrugs Acting On Cardio Vascular SystemANUSHYA B PSGRKCWNo ratings yet
- Wesam R KadhumDocument31 pagesWesam R Kadhumwisam_1by1No ratings yet
- 13.angina and Anti-Anginal DrugsDocument60 pages13.angina and Anti-Anginal Drugsbilalsiddique5365No ratings yet
- Antiarrhythmic Drugs FinalDocument31 pagesAntiarrhythmic Drugs FinalAmanuel Maru50% (2)
- Lec.5 Drugs For Heart FailureDocument19 pagesLec.5 Drugs For Heart FailureAbuzar DawarNo ratings yet
- CHFDocument11 pagesCHFGwendolyn Talahiban LusaraNo ratings yet
- Some Important Points To RememberDocument3 pagesSome Important Points To RememberTaman HoangNo ratings yet
- Lec 3 Heart FailureDocument25 pagesLec 3 Heart FailureDelete AccountNo ratings yet
- Beta Blockers and Calcium Channel BlockersDocument34 pagesBeta Blockers and Calcium Channel Blockersnevena.stankovic986No ratings yet
- Cholinergic System: e CarbamatesDocument26 pagesCholinergic System: e CarbamatesAcai BoncaiNo ratings yet
- Drugs Affecting The Cardiovascular SystemDocument70 pagesDrugs Affecting The Cardiovascular SystemRayne Bonifacio100% (2)
- What Are The Toxicities of Amiodarone?: CardiologyDocument33 pagesWhat Are The Toxicities of Amiodarone?: Cardiologylakshminivas PingaliNo ratings yet
- Pharmacotherapy of Congestive Heart Failure (CHF)Document163 pagesPharmacotherapy of Congestive Heart Failure (CHF)Aditya rathoreNo ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- Congestive Heart FailureDocument17 pagesCongestive Heart FailureLyana StarkNo ratings yet
- Heart Failure New SlidesDocument41 pagesHeart Failure New SlidesjawadNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Causality Assessment of ADRsDocument45 pagesCausality Assessment of ADRsKrupasagar Pn PalegarNo ratings yet
- Congestive Cardiac FailureDocument27 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Antiprotozoal DrugsDocument46 pagesAntiprotozoal DrugsKrupasagar Pn PalegarNo ratings yet
- Anti InflammatoryDocument20 pagesAnti InflammatoryKrupasagar Pn PalegarNo ratings yet
- AceclofenacDocument17 pagesAceclofenacKrupasagar Pn PalegarNo ratings yet
- BMJ 2022 074216.fullDocument20 pagesBMJ 2022 074216.fullArmando OrtegaNo ratings yet
- Alzheimers-Disease-Genetics-Fact-Sheet 0Document8 pagesAlzheimers-Disease-Genetics-Fact-Sheet 0api-285676076No ratings yet
- Diagnosis of Anaplastic Thyroid Carcinoma On Fine Needle Aspiration Cytology - A Rare Case ReportDocument5 pagesDiagnosis of Anaplastic Thyroid Carcinoma On Fine Needle Aspiration Cytology - A Rare Case ReportEditor_IAIMNo ratings yet
- Severe Dapsone Hypersensitivity Syndrome: Case ReportDocument3 pagesSevere Dapsone Hypersensitivity Syndrome: Case ReportFlorencia PalimbongNo ratings yet
- 6 - Physiology MCQ of General PhysiologyDocument20 pages6 - Physiology MCQ of General PhysiologymohammedNo ratings yet
- Dementia & Alzheimer's Care: Planning and Preparing For The Road AheadDocument14 pagesDementia & Alzheimer's Care: Planning and Preparing For The Road AheadblurrmieNo ratings yet
- 12 Cranial NervesDocument21 pages12 Cranial Nerveseha_9213423No ratings yet
- Amikacin Drug StudyDocument2 pagesAmikacin Drug StudyRussel Kate SulangNo ratings yet
- Otalgia & TinnitusDocument19 pagesOtalgia & Tinnitushonda matizNo ratings yet
- Neuropathology of Epilepsy: Epilepsy-Related Deaths and SUDEPDocument11 pagesNeuropathology of Epilepsy: Epilepsy-Related Deaths and SUDEPTeuku AvicennaNo ratings yet
- Mesenteric Venous Thrombosis 2Document5 pagesMesenteric Venous Thrombosis 2cbnhvpqpgrNo ratings yet
- Bacterial Vaginosis: A Synthesis of The Literature On Etiology, Prevalence, Risk Factors, and Relationship With Chlamydia and Gonorrhea InfectionsDocument10 pagesBacterial Vaginosis: A Synthesis of The Literature On Etiology, Prevalence, Risk Factors, and Relationship With Chlamydia and Gonorrhea InfectionsElison J PanggaloNo ratings yet
- Respiratory and CardiovascularDocument133 pagesRespiratory and CardiovascularHawraa FadhilNo ratings yet
- Thoracic PainDocument36 pagesThoracic PainLuciana ThioNo ratings yet
- Pharmacology Scheme 3rd Prof - by Hafiz Muhammad Attaullah & Aqib RazzaqDocument39 pagesPharmacology Scheme 3rd Prof - by Hafiz Muhammad Attaullah & Aqib Razzaqpham.chopraNo ratings yet
- Enucleation in Companion Animals Feb 2008 Ivj PDFDocument6 pagesEnucleation in Companion Animals Feb 2008 Ivj PDFZayna QhastalaniNo ratings yet
- DNS ENT Case Write UpDocument8 pagesDNS ENT Case Write UpShafiq ZahariNo ratings yet
- Qstream-1 2Document55 pagesQstream-1 2Vijay100% (1)
- Tolvaptan-Drug StudyDocument1 pageTolvaptan-Drug Studykaycelyn jimenez100% (2)
- Addison's DiseaseDocument4 pagesAddison's DiseasedrtpkNo ratings yet
- Translate Acute Mesenteric IschemiaDocument13 pagesTranslate Acute Mesenteric IschemiaFadhli Aufar KasyfiNo ratings yet
- Liver, Biliary Tract and Pancreas PathologyDocument50 pagesLiver, Biliary Tract and Pancreas PathologybonadnadineNo ratings yet
- Cardiacassessmentppt 170323092148Document48 pagesCardiacassessmentppt 170323092148sasNo ratings yet
- Free Radicals and AmaDocument5 pagesFree Radicals and AmaOlga RodriguesNo ratings yet
- Biomedicine & Pharmacotherapy: ReviewDocument14 pagesBiomedicine & Pharmacotherapy: Reviewmr dexterNo ratings yet
- Amiodarone Atrial Fibrillation BerberinDocument10 pagesAmiodarone Atrial Fibrillation Berberinharold jitschak bueno de mesquitaNo ratings yet
- Uswatun Hasanah-195037-2a Rmik (KKPMT)Document4 pagesUswatun Hasanah-195037-2a Rmik (KKPMT)Uswatun HasanahNo ratings yet
- Case 2 Hydrocephalus Group 4Document27 pagesCase 2 Hydrocephalus Group 4younggirldavidNo ratings yet