
A Case of Pelvic and Right Iliac Fossa Abscess: A Diagnostic Dilemma
A Case of Pelvic and Right Iliac Fossa Abscess: A Diagnostic Dilemma
You might also like
- Retail Standard Operating ProceduresDocument55 pagesRetail Standard Operating ProceduresGurmeet Kaur Simmy83% (12)
- Filarete Treatise On Architecture PDFDocument2 pagesFilarete Treatise On Architecture PDFKelly0% (5)
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Case of Peptic Ulcer in Recent Op/C/O Total Thyroidectomy: A Rare Case ReportDocument3 pagesA Case of Peptic Ulcer in Recent Op/C/O Total Thyroidectomy: A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Adult Abdominal Cystic Lymphangioma Revealed by Intra Peritoneal Hemorrhage A Case ReportDocument3 pagesAdult Abdominal Cystic Lymphangioma Revealed by Intra Peritoneal Hemorrhage A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Consenso Internacional Tto NivaDocument15 pagesConsenso Internacional Tto Nivadrluciano.rangelNo ratings yet
- The Management of Perianal Abscess With An Udumber Ksheer Pichu - A Case ReportDocument4 pagesThe Management of Perianal Abscess With An Udumber Ksheer Pichu - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Document Heading Doi: 10.21276/apjhs.2016.3.4s.2 Research ArticleDocument9 pagesDocument Heading Doi: 10.21276/apjhs.2016.3.4s.2 Research ArticleluckystarNo ratings yet
- Exploratorylaparotomyinthe EmergencyroomDocument5 pagesExploratorylaparotomyinthe EmergencyroomBalaji MallaNo ratings yet
- Scrotal Abdomen A Case ReportDocument4 pagesScrotal Abdomen A Case ReportkiranNo ratings yet
- A Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalDocument4 pagesA Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jgo 2019 30 E40Document8 pagesJgo 2019 30 E40Jheyson Javier Barrios PereiraNo ratings yet
- 3Document8 pages3polomska.kmNo ratings yet
- US Diagnosis of Acute Appendicitis: PendahuluanDocument6 pagesUS Diagnosis of Acute Appendicitis: PendahuluanN4123 Ap UneNo ratings yet
- Abses Adalah 1332 5211 1 PBDocument5 pagesAbses Adalah 1332 5211 1 PBSayhelloTVNo ratings yet
- Gastrointestinal Perforation 2Document6 pagesGastrointestinal Perforation 2shat bidNo ratings yet
- A Clinical Study of Generalised Peritonitis and ItDocument9 pagesA Clinical Study of Generalised Peritonitis and ItafifahNo ratings yet
- Glauser Et Al (Sept 2019)Document7 pagesGlauser Et Al (Sept 2019)drpklalNo ratings yet
- MainDocument5 pagesMainSheila FSifakNo ratings yet
- Role of Limited Caecal Resection in Patients With Acute Gangrenous AppendicitisDocument6 pagesRole of Limited Caecal Resection in Patients With Acute Gangrenous AppendicitisPavan KumarNo ratings yet
- 01 Diagnosis of Acute Appendicitis Ultrasound As First-Line Imaging ModalityDocument5 pages01 Diagnosis of Acute Appendicitis Ultrasound As First-Line Imaging ModalityFelipe MayorcaNo ratings yet
- Colorectal Cancer Implantation Metastasis in HaemoDocument7 pagesColorectal Cancer Implantation Metastasis in HaemoOsi ZaidNo ratings yet
- 10 5799-Ahinjs 01 2012 04 0203-104197Document4 pages10 5799-Ahinjs 01 2012 04 0203-104197rani kadekNo ratings yet
- Glimpses On Rare Cases of Thigh Swellings - A Case SeriesDocument5 pagesGlimpses On Rare Cases of Thigh Swellings - A Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Laparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceDocument5 pagesLaparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceMudassar SattarNo ratings yet
- An Analysis of Bowel Perforation Cases at A Tertiary Care CentreDocument8 pagesAn Analysis of Bowel Perforation Cases at A Tertiary Care CentreIJAR JOURNALNo ratings yet
- Outcome of Surgical Site Infection Following Inguinal Hernia ClosureDocument4 pagesOutcome of Surgical Site Infection Following Inguinal Hernia ClosureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Prospective Comparativestudy of Open Versus Laparoscopic Appendectomy: A Single Unit StudyDocument8 pagesA Prospective Comparativestudy of Open Versus Laparoscopic Appendectomy: A Single Unit StudyIJAR JOURNALNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument5 pagesAnnals of Medicine and Surgery: SciencedirectMishel Rodriguez GuzmanNo ratings yet
- Rare Sigmoid Abdominal Wall Fistula After Appendectomy: A Case ReportDocument6 pagesRare Sigmoid Abdominal Wall Fistula After Appendectomy: A Case Reportjlcano1210No ratings yet
- Neuroendocrine Tumor of The ApDocument6 pagesNeuroendocrine Tumor of The ApVenus PlanetNo ratings yet
- A Clinical Study of Clavien-Dindo Classification of Postoperative Complications Following Major Abdominal Surgeries in A Tertiary Care CentreDocument4 pagesA Clinical Study of Clavien-Dindo Classification of Postoperative Complications Following Major Abdominal Surgeries in A Tertiary Care CentreInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hernia InguinalisDocument7 pagesHernia InguinalisabduNo ratings yet
- ArticleText 56455 1 10 20200603Document8 pagesArticleText 56455 1 10 20200603Kurniamervinanda KurniaNo ratings yet
- Subtotal Thyroidectomy For Giant Goiters Under Local Anesthesia: Experience With 15 NigeriansDocument5 pagesSubtotal Thyroidectomy For Giant Goiters Under Local Anesthesia: Experience With 15 Nigerianssantri safiraNo ratings yet
- Abdelhameed Et Al (June 2019)Document6 pagesAbdelhameed Et Al (June 2019)drpklalNo ratings yet
- Assessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryDocument8 pagesAssessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryIJAR JOURNALNo ratings yet
- A Clinical Study of Incisional Hernia and Management: Research ArticleDocument4 pagesA Clinical Study of Incisional Hernia and Management: Research ArticleAMBUJ KUMAR SONINo ratings yet
- Mucinous Neoplasm of Appendix TreatmentDocument3 pagesMucinous Neoplasm of Appendix TreatmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparative Analysis of Clinical Outcomes of Open Appendectomy and Laparoscopic AppendectomyDocument6 pagesComparative Analysis of Clinical Outcomes of Open Appendectomy and Laparoscopic AppendectomyIJRASETPublicationsNo ratings yet
- Absence Liver DullnessDocument8 pagesAbsence Liver DullnessqweqweqwNo ratings yet
- Burden of Adhesions in Abdominal and Pelvic SurgeryDocument15 pagesBurden of Adhesions in Abdominal and Pelvic SurgeryDian AdiNo ratings yet
- Is The Combination of An Abdominoplasty With A Cesarean Section Safe A New Concept of Beauty LaborDocument2 pagesIs The Combination of An Abdominoplasty With A Cesarean Section Safe A New Concept of Beauty LaborChristina VasquezNo ratings yet
- 8 Mai 2020Document3 pages8 Mai 2020Radu MiricaNo ratings yet
- 10 Pseudocyst Simple Treatment 2017Document3 pages10 Pseudocyst Simple Treatment 2017solikin ikinNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case ReportsFhy Ghokiel AbiezNo ratings yet
- Jurnal 5Document4 pagesJurnal 5Roro Khairiyah AmaliaNo ratings yet
- 91-Article Text-348-2-10-20200304Document4 pages91-Article Text-348-2-10-20200304muhammadnurul asmiNo ratings yet
- Adult Intussusception - An Uncommon Condition and Challenging Management 2021Document8 pagesAdult Intussusception - An Uncommon Condition and Challenging Management 2021吳醫師No ratings yet
- Synthetic Versus Biological Mesh in Laparoscopic and Open Ventral Hérnia RepairDocument9 pagesSynthetic Versus Biological Mesh in Laparoscopic and Open Ventral Hérnia RepairRhuan AntonioNo ratings yet
- Laparoscopic Compared With Open Surgery TOADocument7 pagesLaparoscopic Compared With Open Surgery TOARizka AdiNo ratings yet
- Assessment of Alveolar Bone Augmentation in Intrabony Defects Employing Platelet-Rich Fibrin (PRF) Membrane and Sticky Bone (Injectable-PRF & Demineralized Freeze-Dried Bone Graft) - A Case ReportDocument4 pagesAssessment of Alveolar Bone Augmentation in Intrabony Defects Employing Platelet-Rich Fibrin (PRF) Membrane and Sticky Bone (Injectable-PRF & Demineralized Freeze-Dried Bone Graft) - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 11 I January 2023Document4 pages11 I January 2023IJRASETPublicationsNo ratings yet
- Consensus Statements On Pre-Invasive Vulvar LesionsDocument16 pagesConsensus Statements On Pre-Invasive Vulvar LesionsChristian Leonardo Molina HinojosaNo ratings yet
- ArticleText 56455 1 10 20200603Document8 pagesArticleText 56455 1 10 20200603YosuaNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case Reportsyongky sugandaNo ratings yet
- AfrJPaediatrSurg114293-1394417 035224Document4 pagesAfrJPaediatrSurg114293-1394417 035224mia rachmiNo ratings yet
- Liver Abscess: Catheter Drainage V/s Needle AspirationDocument6 pagesLiver Abscess: Catheter Drainage V/s Needle AspirationMishel Rodriguez GuzmanNo ratings yet
- The Rare TravellersDocument3 pagesThe Rare TravellersPedro TrigoNo ratings yet
- Clinical and Radiological Investigations To Predict Difficult Laparoscopic CholecystectomyDocument5 pagesClinical and Radiological Investigations To Predict Difficult Laparoscopic CholecystectomySuyash GhadgeNo ratings yet
- Treatment of Intra-Abdominal Hydatid Cyst Using Modified PAIR Technique: Single Center ExperiencesDocument5 pagesTreatment of Intra-Abdominal Hydatid Cyst Using Modified PAIR Technique: Single Center ExperiencesSandu AlexandraNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Intrusion Detection and Prevention Systems for Ad-Hoc NetworksDocument8 pagesIntrusion Detection and Prevention Systems for Ad-Hoc NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemDocument6 pagesFuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Innovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piDocument8 pagesInnovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Geotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioDocument10 pagesGeotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsDocument6 pagesA Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachDocument16 pagesThe Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoDocument7 pagesIntegration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionDocument9 pagesAnalysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Importance of Early Intervention of Traumatic Cataract in ChildrenDocument5 pagesImportance of Early Intervention of Traumatic Cataract in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportDocument4 pagesDiode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Breaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsDocument14 pagesBreaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonDocument11 pagesOccupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Disseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsDocument15 pagesDisseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparison of JavaScript Frontend Frameworks - Angular, React, and VueDocument8 pagesComparison of JavaScript Frontend Frameworks - Angular, React, and VueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Organizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaDocument10 pagesOrganizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship of Total Quality Management Practices and Project Performance With Risk Management As Mediator: A Study of East Coast Rail Link Project in MalaysiaDocument19 pagesThe Relationship of Total Quality Management Practices and Project Performance With Risk Management As Mediator: A Study of East Coast Rail Link Project in MalaysiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Investigation Model To Combat Computer Gaming Delinquency in South Africa, Server-Based Gaming, and Illegal Online GamingDocument15 pagesAn Investigation Model To Combat Computer Gaming Delinquency in South Africa, Server-Based Gaming, and Illegal Online GamingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integrating Multimodal Deep Learning For Enhanced News Sentiment Analysis and Market Movement ForecastingDocument8 pagesIntegrating Multimodal Deep Learning For Enhanced News Sentiment Analysis and Market Movement ForecastingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Influence of Artificial Intelligence On Employment Trends in The United States (US)Document5 pagesThe Influence of Artificial Intelligence On Employment Trends in The United States (US)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Mediating Effect of Encouraging Attitude of School Principals On Personal Well-Being and Career Ethics of TeachersDocument10 pagesMediating Effect of Encouraging Attitude of School Principals On Personal Well-Being and Career Ethics of TeachersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Classifying Crop Leaf Diseases Using Different Deep Learning Models With Transfer LearningDocument8 pagesClassifying Crop Leaf Diseases Using Different Deep Learning Models With Transfer LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Total Cost of Ownership of Electric Car and Internal Combustion Engine Car With Performance NormalizationDocument11 pagesTotal Cost of Ownership of Electric Car and Internal Combustion Engine Car With Performance NormalizationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Development of Creative Thinking: Case Study of Basic Design StudioDocument9 pagesDevelopment of Creative Thinking: Case Study of Basic Design StudioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Gender-Based Violence: Engaging Children in The SolutionDocument10 pagesGender-Based Violence: Engaging Children in The SolutionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Monetary and Non-Monetary Rewards For Employees Motivation in Tanzania Public Sector: The Management PerspectivesDocument8 pagesMonetary and Non-Monetary Rewards For Employees Motivation in Tanzania Public Sector: The Management PerspectivesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Personality Factors As Predictors of The Level of Personality Functioning in Adolescence: Examining The Influence of Birth Order, Financial Status, and SexDocument10 pagesPersonality Factors As Predictors of The Level of Personality Functioning in Adolescence: Examining The Influence of Birth Order, Financial Status, and SexInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Knowledge About Halitosis and Dental and Oral Hygiene in Patients With Fixed Orthodontics at The HK Medical Center MakassarDocument4 pagesThe Relationship Between Knowledge About Halitosis and Dental and Oral Hygiene in Patients With Fixed Orthodontics at The HK Medical Center MakassarInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Synergizing For Students Success: A Collaborative Engagement of Parent-Teacher in Grade FourDocument13 pagesSynergizing For Students Success: A Collaborative Engagement of Parent-Teacher in Grade FourInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Evaluation of Causes of Visual Impairment Among Bespectacled Between The Age 18-23: A Study From Tamil Nadu, IndiaDocument3 pagesEvaluation of Causes of Visual Impairment Among Bespectacled Between The Age 18-23: A Study From Tamil Nadu, IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Comparative Analysis of Pineapples (Ananas Comosus) From Different Bioethanol Sources Available in The PhilippinesDocument39 pagesA Comparative Analysis of Pineapples (Ananas Comosus) From Different Bioethanol Sources Available in The PhilippinesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Future of Luxury Travel: Challenges and Solutions For Returning To OperationsDocument8 pagesThe Future of Luxury Travel: Challenges and Solutions For Returning To OperationsAshu SinghNo ratings yet
- The Legend of Lake TobaDocument4 pagesThe Legend of Lake TobaLilis MahmudatunNo ratings yet
- TSH The Sexuality Wheel Tool EnglishDocument2 pagesTSH The Sexuality Wheel Tool EnglishRita TorresNo ratings yet
- Two-Stage Power Decoupling For A Single-Phase Photovoltaic Inverter by Controlling The DC-Link Voltage Ripple in The DQ FrameDocument6 pagesTwo-Stage Power Decoupling For A Single-Phase Photovoltaic Inverter by Controlling The DC-Link Voltage Ripple in The DQ FrameAkbar aliNo ratings yet
- Sustainable DevelopmentDocument5 pagesSustainable DevelopmentMeera NairNo ratings yet
- Draft Product Vision BoardDocument1 pageDraft Product Vision BoardJohn PatlolNo ratings yet
- Dissertation File FlipkartDocument6 pagesDissertation File FlipkartArtNo ratings yet
- Watergate Scandal Thesis StatementDocument7 pagesWatergate Scandal Thesis Statementafhbexrci100% (2)
- Chapter 5 Entrepreneurship by Zubair A Khan.Document27 pagesChapter 5 Entrepreneurship by Zubair A Khan.Zubair A Khan0% (1)
- Module Foundation of Education 2Document39 pagesModule Foundation of Education 2Bernardino VirgilioNo ratings yet
- Pcar 09Document104 pagesPcar 09Mark Jovince CardenasNo ratings yet
- Igcse Chemistry 3ed TR HtutsDocument2 pagesIgcse Chemistry 3ed TR HtutsMarin PesicNo ratings yet
- Comptel Business Service Tool™: Functional DescriptionDocument25 pagesComptel Business Service Tool™: Functional DescriptionIvanIvanovNo ratings yet
- First Achievement TestDocument3 pagesFirst Achievement TestJustin Shane LarotinNo ratings yet
- Xenos HunterDocument4 pagesXenos HunterBillthe Something100% (1)
- Rite of MisraimDocument8 pagesRite of MisraimOnPoint Marius100% (1)
- Along Came Love by Cheryl ZeeDocument787 pagesAlong Came Love by Cheryl ZeeFungai Wise MukaratiNo ratings yet
- Oracle Installation FilesDocument5 pagesOracle Installation FilesKabachuNo ratings yet
- Chem Lab - HalidesDocument6 pagesChem Lab - HalidesEmmaNo ratings yet
- Name: Teacher: Date: Score:: Probability Using A SpinnerDocument2 pagesName: Teacher: Date: Score:: Probability Using A SpinnerSara ShaiboonNo ratings yet
- Lesson Plan in Technology For Teaching and LearningDocument6 pagesLesson Plan in Technology For Teaching and LearningNiña Mae CabsagNo ratings yet
- Weekly Home Learning Plan: Carmen National High School Carmen, San Agustin, RomblonDocument2 pagesWeekly Home Learning Plan: Carmen National High School Carmen, San Agustin, RomblonVina Verdadero TomeNo ratings yet
- CombinepdfDocument208 pagesCombinepdfH. TэлмэнNo ratings yet
- Ra 8189Document13 pagesRa 8189Jv FerminNo ratings yet
- Phytoremediation 150123100305 Conversion Gate02Document49 pagesPhytoremediation 150123100305 Conversion Gate02Kumar MadhuNo ratings yet
- Assignment/ Tugasan - Basic Interpersonal CommunicationDocument4 pagesAssignment/ Tugasan - Basic Interpersonal CommunicationMuhamad SaifulNo ratings yet
- Life Insurance Closed Books and Related Management ChallengesDocument2 pagesLife Insurance Closed Books and Related Management ChallengesVenkatakrishnan RamachandranNo ratings yet
- Comparative Report On Fast Food Study in Thailand, Indonesia and Vietnam in 2015Document48 pagesComparative Report On Fast Food Study in Thailand, Indonesia and Vietnam in 2015Daksh SetiaNo ratings yet























































































































Download as pdf or txt
Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR1619
A Case of Pelvic and Right Iliac Fossa
Abscess: A Diagnostic Dilemma
Dr. Pratik Dash1 Dr. J.G. Vagadiya2
Second Year Resident Doctor Associate Professor
1 2
Department of General Surgery, PDU Medical Department of General Surgery, PDU Medical
College & Hospital, Rajkot College & Hospital, Rajkot
Dr. J.G. Bhatt3 Dr. Binoy Behera4
Professor & HOD Third Year Resident Doctor
3 4
Department of General Surgery, PDU Medical Departmeent of General Surgery, PDU Medical
College & Hospital, Rajkot College & Hospital, Rajkot
Dr. Hiral Chaudhary5
Senior Resident Doctor
5
Department of General Surgery, PDU Medical
College & Hospital, Rajkot
Abstract:- RIF abscess is an intriguing condition which
can possibly be life compromising. It can prompt sepsis
whenever cracked. Regularly, these abscesses are
overseen through a blend of clinical and careful surgical
intervention. Herein, we report a pelvic and RIF abscess
which was dealt laparoscopically.
Keywords:- Pelvic Abscess, Right Ileac Fossa (RIF)
Abscess.
I. INTRODUCTION
Intra-abdominal and pelvic abscesses can be created as
a result of various etiologies. Regularly, these abscesses are
overseen through a blend of medical (antibiotics) and
surgical (drainage) interventions. This is a case report of a
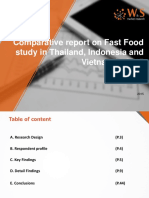
pelvic and right iliac fossa abscess which was imitating an Fig 1 CT-Scan Showing Abscess in Anterior
appendicular abscess and was depleted by laparoscopic Abdominal wall Communicating Intraperitoneally
methodology.
II. CASE REPORT
We report the instance of a 53 years old female patient
presented to our surgical emergency with pain abdomen
which was moderate to intense in nature and localised to
right ileac fossa region and was associated with fever with
nausea and vomiting. There was no history of any surgical
interventions in the past or any associated comorbidities.
Upon per abdomen examination of this patient a
6cmx4cm sized palpable lump was noted in RIF region. We
conducted a series of radiological investigations which
revealed a 69mm x 55mm sized hypodense lesion in right
lower abdominal wall muscle, extending intraperitoneally to
RIF. Another 99mm x 72mm sized intraperitoneal lesion
was noted in pelvic cavity in midline at anterior aspect. Fig 2 CT-Scan Showing Intraperitoneal Abscess
IJISRT24MAR1619 www.ijisrt.com 2061
Volume 9, Issue 3, March – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24MAR1619
Patient was then taken for diagnostic laparoscopy.
Adhesions between omentum and abdominal wall noted
intraoperatively and adhesiolysis with drainage of 10 cc pus
was drained. Omental biopsy was suggestive of chronic
inflammatory changes. Patient was discharged on post
operative day 10, with out-patient management.
Fig 3 Intra-Op Picture of Pus Drainage from RIF Abscess
III. DISCUSSION
The pelvic abscess is a rare condition and is usually
located posteriorly [1]. However, our case was presented
deep in the pelvic region anteriorly. Pain/tenderness,
abdominal distention, fever, anorexia, tachycardia, and
leukocytosis are common symptoms of an intra-abdominal
abscess [2]. The ideal approach for pelvic abscess
management should be safe, effective, minimally invasive,
cost-effective, and it should not affect fertility as much as
possible [3] There are various approaches to draining the
pelvic abscess, including laparoscopy, laparotomy, and
imaging-guided drainage [1].
IV. CONCLUSION
Pelvic abscesses are managed mainly through a
combination of medical and surgical procedures. Here the
patient was treated laparoscopically for pelvic and RIF
abscess.
REFERENCES
[1]. Devrim Aknc, Onur Ergun, C¸ ada Topel, T¨urkmen
C¸ ift¸ci, and Okan Akhan. Pelvic abscess drainage:
outcome with factors affecting the clinical success.
Diagnostic and Interventional Radiology, 24(3):146,
2018.
[2]. Sarah A Damer. Pelvic Abscess with Presentation as
Inability to Ambulate. Spartan Medical Research
Journal, 2(2), 2018.
[3]. Seth Granberg, Knut Gjelland, and Erling Ekerhovd.
The management of pelvic abscess. Best practice &
research Clinical obstetrics & gynaecology,
23(5):667–678, 2009.
IJISRT24MAR1619 www.ijisrt.com 2062
You might also like
- Retail Standard Operating ProceduresDocument55 pagesRetail Standard Operating ProceduresGurmeet Kaur Simmy83% (12)
- Filarete Treatise On Architecture PDFDocument2 pagesFilarete Treatise On Architecture PDFKelly0% (5)
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Case of Peptic Ulcer in Recent Op/C/O Total Thyroidectomy: A Rare Case ReportDocument3 pagesA Case of Peptic Ulcer in Recent Op/C/O Total Thyroidectomy: A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Adult Abdominal Cystic Lymphangioma Revealed by Intra Peritoneal Hemorrhage A Case ReportDocument3 pagesAdult Abdominal Cystic Lymphangioma Revealed by Intra Peritoneal Hemorrhage A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Consenso Internacional Tto NivaDocument15 pagesConsenso Internacional Tto Nivadrluciano.rangelNo ratings yet
- The Management of Perianal Abscess With An Udumber Ksheer Pichu - A Case ReportDocument4 pagesThe Management of Perianal Abscess With An Udumber Ksheer Pichu - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Document Heading Doi: 10.21276/apjhs.2016.3.4s.2 Research ArticleDocument9 pagesDocument Heading Doi: 10.21276/apjhs.2016.3.4s.2 Research ArticleluckystarNo ratings yet
- Exploratorylaparotomyinthe EmergencyroomDocument5 pagesExploratorylaparotomyinthe EmergencyroomBalaji MallaNo ratings yet
- Scrotal Abdomen A Case ReportDocument4 pagesScrotal Abdomen A Case ReportkiranNo ratings yet
- A Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalDocument4 pagesA Prospective Observational Study On Scola For Ventral Hernia With Diastasis Recti - Our Experience at A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jgo 2019 30 E40Document8 pagesJgo 2019 30 E40Jheyson Javier Barrios PereiraNo ratings yet
- 3Document8 pages3polomska.kmNo ratings yet
- US Diagnosis of Acute Appendicitis: PendahuluanDocument6 pagesUS Diagnosis of Acute Appendicitis: PendahuluanN4123 Ap UneNo ratings yet
- Abses Adalah 1332 5211 1 PBDocument5 pagesAbses Adalah 1332 5211 1 PBSayhelloTVNo ratings yet
- Gastrointestinal Perforation 2Document6 pagesGastrointestinal Perforation 2shat bidNo ratings yet
- A Clinical Study of Generalised Peritonitis and ItDocument9 pagesA Clinical Study of Generalised Peritonitis and ItafifahNo ratings yet
- Glauser Et Al (Sept 2019)Document7 pagesGlauser Et Al (Sept 2019)drpklalNo ratings yet
- MainDocument5 pagesMainSheila FSifakNo ratings yet
- Role of Limited Caecal Resection in Patients With Acute Gangrenous AppendicitisDocument6 pagesRole of Limited Caecal Resection in Patients With Acute Gangrenous AppendicitisPavan KumarNo ratings yet
- 01 Diagnosis of Acute Appendicitis Ultrasound As First-Line Imaging ModalityDocument5 pages01 Diagnosis of Acute Appendicitis Ultrasound As First-Line Imaging ModalityFelipe MayorcaNo ratings yet
- Colorectal Cancer Implantation Metastasis in HaemoDocument7 pagesColorectal Cancer Implantation Metastasis in HaemoOsi ZaidNo ratings yet
- 10 5799-Ahinjs 01 2012 04 0203-104197Document4 pages10 5799-Ahinjs 01 2012 04 0203-104197rani kadekNo ratings yet
- Glimpses On Rare Cases of Thigh Swellings - A Case SeriesDocument5 pagesGlimpses On Rare Cases of Thigh Swellings - A Case SeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Laparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceDocument5 pagesLaparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceMudassar SattarNo ratings yet
- An Analysis of Bowel Perforation Cases at A Tertiary Care CentreDocument8 pagesAn Analysis of Bowel Perforation Cases at A Tertiary Care CentreIJAR JOURNALNo ratings yet
- Outcome of Surgical Site Infection Following Inguinal Hernia ClosureDocument4 pagesOutcome of Surgical Site Infection Following Inguinal Hernia ClosureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Prospective Comparativestudy of Open Versus Laparoscopic Appendectomy: A Single Unit StudyDocument8 pagesA Prospective Comparativestudy of Open Versus Laparoscopic Appendectomy: A Single Unit StudyIJAR JOURNALNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument5 pagesAnnals of Medicine and Surgery: SciencedirectMishel Rodriguez GuzmanNo ratings yet
- Rare Sigmoid Abdominal Wall Fistula After Appendectomy: A Case ReportDocument6 pagesRare Sigmoid Abdominal Wall Fistula After Appendectomy: A Case Reportjlcano1210No ratings yet
- Neuroendocrine Tumor of The ApDocument6 pagesNeuroendocrine Tumor of The ApVenus PlanetNo ratings yet
- A Clinical Study of Clavien-Dindo Classification of Postoperative Complications Following Major Abdominal Surgeries in A Tertiary Care CentreDocument4 pagesA Clinical Study of Clavien-Dindo Classification of Postoperative Complications Following Major Abdominal Surgeries in A Tertiary Care CentreInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hernia InguinalisDocument7 pagesHernia InguinalisabduNo ratings yet
- ArticleText 56455 1 10 20200603Document8 pagesArticleText 56455 1 10 20200603Kurniamervinanda KurniaNo ratings yet
- Subtotal Thyroidectomy For Giant Goiters Under Local Anesthesia: Experience With 15 NigeriansDocument5 pagesSubtotal Thyroidectomy For Giant Goiters Under Local Anesthesia: Experience With 15 Nigerianssantri safiraNo ratings yet
- Abdelhameed Et Al (June 2019)Document6 pagesAbdelhameed Et Al (June 2019)drpklalNo ratings yet
- Assessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryDocument8 pagesAssessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryIJAR JOURNALNo ratings yet
- A Clinical Study of Incisional Hernia and Management: Research ArticleDocument4 pagesA Clinical Study of Incisional Hernia and Management: Research ArticleAMBUJ KUMAR SONINo ratings yet
- Mucinous Neoplasm of Appendix TreatmentDocument3 pagesMucinous Neoplasm of Appendix TreatmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparative Analysis of Clinical Outcomes of Open Appendectomy and Laparoscopic AppendectomyDocument6 pagesComparative Analysis of Clinical Outcomes of Open Appendectomy and Laparoscopic AppendectomyIJRASETPublicationsNo ratings yet
- Absence Liver DullnessDocument8 pagesAbsence Liver DullnessqweqweqwNo ratings yet
- Burden of Adhesions in Abdominal and Pelvic SurgeryDocument15 pagesBurden of Adhesions in Abdominal and Pelvic SurgeryDian AdiNo ratings yet
- Is The Combination of An Abdominoplasty With A Cesarean Section Safe A New Concept of Beauty LaborDocument2 pagesIs The Combination of An Abdominoplasty With A Cesarean Section Safe A New Concept of Beauty LaborChristina VasquezNo ratings yet
- 8 Mai 2020Document3 pages8 Mai 2020Radu MiricaNo ratings yet
- 10 Pseudocyst Simple Treatment 2017Document3 pages10 Pseudocyst Simple Treatment 2017solikin ikinNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case ReportsFhy Ghokiel AbiezNo ratings yet
- Jurnal 5Document4 pagesJurnal 5Roro Khairiyah AmaliaNo ratings yet
- 91-Article Text-348-2-10-20200304Document4 pages91-Article Text-348-2-10-20200304muhammadnurul asmiNo ratings yet
- Adult Intussusception - An Uncommon Condition and Challenging Management 2021Document8 pagesAdult Intussusception - An Uncommon Condition and Challenging Management 2021吳醫師No ratings yet
- Synthetic Versus Biological Mesh in Laparoscopic and Open Ventral Hérnia RepairDocument9 pagesSynthetic Versus Biological Mesh in Laparoscopic and Open Ventral Hérnia RepairRhuan AntonioNo ratings yet
- Laparoscopic Compared With Open Surgery TOADocument7 pagesLaparoscopic Compared With Open Surgery TOARizka AdiNo ratings yet
- Assessment of Alveolar Bone Augmentation in Intrabony Defects Employing Platelet-Rich Fibrin (PRF) Membrane and Sticky Bone (Injectable-PRF & Demineralized Freeze-Dried Bone Graft) - A Case ReportDocument4 pagesAssessment of Alveolar Bone Augmentation in Intrabony Defects Employing Platelet-Rich Fibrin (PRF) Membrane and Sticky Bone (Injectable-PRF & Demineralized Freeze-Dried Bone Graft) - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 11 I January 2023Document4 pages11 I January 2023IJRASETPublicationsNo ratings yet
- Consensus Statements On Pre-Invasive Vulvar LesionsDocument16 pagesConsensus Statements On Pre-Invasive Vulvar LesionsChristian Leonardo Molina HinojosaNo ratings yet
- ArticleText 56455 1 10 20200603Document8 pagesArticleText 56455 1 10 20200603YosuaNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case Reportsyongky sugandaNo ratings yet
- AfrJPaediatrSurg114293-1394417 035224Document4 pagesAfrJPaediatrSurg114293-1394417 035224mia rachmiNo ratings yet
- Liver Abscess: Catheter Drainage V/s Needle AspirationDocument6 pagesLiver Abscess: Catheter Drainage V/s Needle AspirationMishel Rodriguez GuzmanNo ratings yet
- The Rare TravellersDocument3 pagesThe Rare TravellersPedro TrigoNo ratings yet
- Clinical and Radiological Investigations To Predict Difficult Laparoscopic CholecystectomyDocument5 pagesClinical and Radiological Investigations To Predict Difficult Laparoscopic CholecystectomySuyash GhadgeNo ratings yet
- Treatment of Intra-Abdominal Hydatid Cyst Using Modified PAIR Technique: Single Center ExperiencesDocument5 pagesTreatment of Intra-Abdominal Hydatid Cyst Using Modified PAIR Technique: Single Center ExperiencesSandu AlexandraNo ratings yet
- Post-cholecystectomy Bile Duct InjuryFrom EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNo ratings yet
- Intrusion Detection and Prevention Systems for Ad-Hoc NetworksDocument8 pagesIntrusion Detection and Prevention Systems for Ad-Hoc NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemDocument6 pagesFuzzy based Tie-Line and LFC of a Two-Area Interconnected SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Innovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piDocument8 pagesInnovative Mathematical Insights through Artificial Intelligence (AI): Analysing Ramanujan Series and the Relationship between e and π\piInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Geotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioDocument10 pagesGeotechnical Assessment of Selected Lateritic Soils in Southwest Nigeria for Road Construction and Development of Artificial Neural Network Mathematical Based Model for Prediction of the California Bearing RatioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsDocument6 pagesA Novel Approach to Template Filling with Automatic Speech Recognition for Healthcare ProfessionalsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachDocument16 pagesThe Effects of Liquid Density and Impeller Size with Volute Clearance on the Performance of Radial Blade Centrifugal Pumps: An Experimental ApproachInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoDocument7 pagesIntegration of Information Communication Technology, Strategic Leadership and Academic Performance in Universities in North Kivu, Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionDocument9 pagesAnalysis of Factors Obstacling Construction Work in The Tojo Una-Una Islands RegionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Importance of Early Intervention of Traumatic Cataract in ChildrenDocument5 pagesImportance of Early Intervention of Traumatic Cataract in ChildrenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportDocument4 pagesDiode Laser Therapy for Drug Induced Gingival Enlaregement: A CaseReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Breaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsDocument14 pagesBreaking Down Barriers To Inclusion: Stories of Grade Four Teachers in Maintream ClassroomsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Occupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonDocument11 pagesOccupational Safety: PPE Use and Hazard Experiences Among Welders in Valencia City, BukidnonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Disseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsDocument15 pagesDisseminating The Real-World Importance of Conjunct Studies of Acculturation, Transculturation, and Deculturation Processes: Why This Can Be A Useful Technique To Analyze Real-World ObservationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparison of JavaScript Frontend Frameworks - Angular, React, and VueDocument8 pagesComparison of JavaScript Frontend Frameworks - Angular, React, and VueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Organizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaDocument10 pagesOrganizational Factors That Influence Information Security in Smes: A Case Study of Mogadishu, SomaliaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship of Total Quality Management Practices and Project Performance With Risk Management As Mediator: A Study of East Coast Rail Link Project in MalaysiaDocument19 pagesThe Relationship of Total Quality Management Practices and Project Performance With Risk Management As Mediator: A Study of East Coast Rail Link Project in MalaysiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Investigation Model To Combat Computer Gaming Delinquency in South Africa, Server-Based Gaming, and Illegal Online GamingDocument15 pagesAn Investigation Model To Combat Computer Gaming Delinquency in South Africa, Server-Based Gaming, and Illegal Online GamingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Integrating Multimodal Deep Learning For Enhanced News Sentiment Analysis and Market Movement ForecastingDocument8 pagesIntegrating Multimodal Deep Learning For Enhanced News Sentiment Analysis and Market Movement ForecastingInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Influence of Artificial Intelligence On Employment Trends in The United States (US)Document5 pagesThe Influence of Artificial Intelligence On Employment Trends in The United States (US)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Mediating Effect of Encouraging Attitude of School Principals On Personal Well-Being and Career Ethics of TeachersDocument10 pagesMediating Effect of Encouraging Attitude of School Principals On Personal Well-Being and Career Ethics of TeachersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Classifying Crop Leaf Diseases Using Different Deep Learning Models With Transfer LearningDocument8 pagesClassifying Crop Leaf Diseases Using Different Deep Learning Models With Transfer LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Total Cost of Ownership of Electric Car and Internal Combustion Engine Car With Performance NormalizationDocument11 pagesTotal Cost of Ownership of Electric Car and Internal Combustion Engine Car With Performance NormalizationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Development of Creative Thinking: Case Study of Basic Design StudioDocument9 pagesDevelopment of Creative Thinking: Case Study of Basic Design StudioInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Gender-Based Violence: Engaging Children in The SolutionDocument10 pagesGender-Based Violence: Engaging Children in The SolutionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Monetary and Non-Monetary Rewards For Employees Motivation in Tanzania Public Sector: The Management PerspectivesDocument8 pagesMonetary and Non-Monetary Rewards For Employees Motivation in Tanzania Public Sector: The Management PerspectivesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Personality Factors As Predictors of The Level of Personality Functioning in Adolescence: Examining The Influence of Birth Order, Financial Status, and SexDocument10 pagesPersonality Factors As Predictors of The Level of Personality Functioning in Adolescence: Examining The Influence of Birth Order, Financial Status, and SexInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Knowledge About Halitosis and Dental and Oral Hygiene in Patients With Fixed Orthodontics at The HK Medical Center MakassarDocument4 pagesThe Relationship Between Knowledge About Halitosis and Dental and Oral Hygiene in Patients With Fixed Orthodontics at The HK Medical Center MakassarInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Synergizing For Students Success: A Collaborative Engagement of Parent-Teacher in Grade FourDocument13 pagesSynergizing For Students Success: A Collaborative Engagement of Parent-Teacher in Grade FourInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Evaluation of Causes of Visual Impairment Among Bespectacled Between The Age 18-23: A Study From Tamil Nadu, IndiaDocument3 pagesEvaluation of Causes of Visual Impairment Among Bespectacled Between The Age 18-23: A Study From Tamil Nadu, IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Comparative Analysis of Pineapples (Ananas Comosus) From Different Bioethanol Sources Available in The PhilippinesDocument39 pagesA Comparative Analysis of Pineapples (Ananas Comosus) From Different Bioethanol Sources Available in The PhilippinesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Future of Luxury Travel: Challenges and Solutions For Returning To OperationsDocument8 pagesThe Future of Luxury Travel: Challenges and Solutions For Returning To OperationsAshu SinghNo ratings yet
- The Legend of Lake TobaDocument4 pagesThe Legend of Lake TobaLilis MahmudatunNo ratings yet
- TSH The Sexuality Wheel Tool EnglishDocument2 pagesTSH The Sexuality Wheel Tool EnglishRita TorresNo ratings yet
- Two-Stage Power Decoupling For A Single-Phase Photovoltaic Inverter by Controlling The DC-Link Voltage Ripple in The DQ FrameDocument6 pagesTwo-Stage Power Decoupling For A Single-Phase Photovoltaic Inverter by Controlling The DC-Link Voltage Ripple in The DQ FrameAkbar aliNo ratings yet
- Sustainable DevelopmentDocument5 pagesSustainable DevelopmentMeera NairNo ratings yet
- Draft Product Vision BoardDocument1 pageDraft Product Vision BoardJohn PatlolNo ratings yet
- Dissertation File FlipkartDocument6 pagesDissertation File FlipkartArtNo ratings yet
- Watergate Scandal Thesis StatementDocument7 pagesWatergate Scandal Thesis Statementafhbexrci100% (2)
- Chapter 5 Entrepreneurship by Zubair A Khan.Document27 pagesChapter 5 Entrepreneurship by Zubair A Khan.Zubair A Khan0% (1)
- Module Foundation of Education 2Document39 pagesModule Foundation of Education 2Bernardino VirgilioNo ratings yet
- Pcar 09Document104 pagesPcar 09Mark Jovince CardenasNo ratings yet
- Igcse Chemistry 3ed TR HtutsDocument2 pagesIgcse Chemistry 3ed TR HtutsMarin PesicNo ratings yet
- Comptel Business Service Tool™: Functional DescriptionDocument25 pagesComptel Business Service Tool™: Functional DescriptionIvanIvanovNo ratings yet
- First Achievement TestDocument3 pagesFirst Achievement TestJustin Shane LarotinNo ratings yet
- Xenos HunterDocument4 pagesXenos HunterBillthe Something100% (1)
- Rite of MisraimDocument8 pagesRite of MisraimOnPoint Marius100% (1)
- Along Came Love by Cheryl ZeeDocument787 pagesAlong Came Love by Cheryl ZeeFungai Wise MukaratiNo ratings yet
- Oracle Installation FilesDocument5 pagesOracle Installation FilesKabachuNo ratings yet
- Chem Lab - HalidesDocument6 pagesChem Lab - HalidesEmmaNo ratings yet
- Name: Teacher: Date: Score:: Probability Using A SpinnerDocument2 pagesName: Teacher: Date: Score:: Probability Using A SpinnerSara ShaiboonNo ratings yet
- Lesson Plan in Technology For Teaching and LearningDocument6 pagesLesson Plan in Technology For Teaching and LearningNiña Mae CabsagNo ratings yet
- Weekly Home Learning Plan: Carmen National High School Carmen, San Agustin, RomblonDocument2 pagesWeekly Home Learning Plan: Carmen National High School Carmen, San Agustin, RomblonVina Verdadero TomeNo ratings yet
- CombinepdfDocument208 pagesCombinepdfH. TэлмэнNo ratings yet
- Ra 8189Document13 pagesRa 8189Jv FerminNo ratings yet
- Phytoremediation 150123100305 Conversion Gate02Document49 pagesPhytoremediation 150123100305 Conversion Gate02Kumar MadhuNo ratings yet
- Assignment/ Tugasan - Basic Interpersonal CommunicationDocument4 pagesAssignment/ Tugasan - Basic Interpersonal CommunicationMuhamad SaifulNo ratings yet
- Life Insurance Closed Books and Related Management ChallengesDocument2 pagesLife Insurance Closed Books and Related Management ChallengesVenkatakrishnan RamachandranNo ratings yet
- Comparative Report On Fast Food Study in Thailand, Indonesia and Vietnam in 2015Document48 pagesComparative Report On Fast Food Study in Thailand, Indonesia and Vietnam in 2015Daksh SetiaNo ratings yet