Download as pdf or txt
You might also like
- Abdominal ImagingDocument6 pagesAbdominal Imagingmihaela2786No ratings yet
- 5th Year Git LectureDocument75 pages5th Year Git Lecturekasilat574No ratings yet
- CASE REPORT 3 - Acute Mesentric Venous Thrombosis With A History Recurrent DVT in Young Age A Case ReportDocument2 pagesCASE REPORT 3 - Acute Mesentric Venous Thrombosis With A History Recurrent DVT in Young Age A Case Reportm.widodo190216No ratings yet
- Lectura 8Document8 pagesLectura 8Daniela Andrea Tello GuaguaNo ratings yet
- Liver Disease: Schwartz Principles of Surgery2010Document50 pagesLiver Disease: Schwartz Principles of Surgery2010ralphNo ratings yet
- Budd-Chiari Syndrome: Michael A. Zimmerman, MD, Andrew M. Cameron, MD, PHD, R. Mark Ghobrial, MD, PHDDocument15 pagesBudd-Chiari Syndrome: Michael A. Zimmerman, MD, Andrew M. Cameron, MD, PHD, R. Mark Ghobrial, MD, PHDCarlos AlmeidaNo ratings yet
- Bruce J BarnonDocument7 pagesBruce J Barnonnasywa rahmatullailyNo ratings yet
- Role of Embolization in The Management of Splenic Trauma: Case ReportDocument3 pagesRole of Embolization in The Management of Splenic Trauma: Case ReportandreigustvNo ratings yet
- Radiology pdf1Document8 pagesRadiology pdf1benediktus_bayuNo ratings yet
- 8874 33333 1 PBDocument3 pages8874 33333 1 PBRanga PereraNo ratings yet
- Pancreatic Pseudocyst EDITEDDocument5 pagesPancreatic Pseudocyst EDITEDLaura LatifaNo ratings yet
- Asymptomatic Hepatobiliary Cystadenoma of The Hepatic Caudate Lobe A Case ReportDocument3 pagesAsymptomatic Hepatobiliary Cystadenoma of The Hepatic Caudate Lobe A Case ReportquileuteNo ratings yet
- Wozniak - Anesthesia For Open Abdominal Aortic SurgeryDocument18 pagesWozniak - Anesthesia For Open Abdominal Aortic SurgeryIbet Enriquez PalaciosNo ratings yet
- 4 2 - 181 182 PDFDocument2 pages4 2 - 181 182 PDFNam LeNo ratings yet
- An Unusual Case of Lower Gastrointestinal HemorrhaDocument3 pagesAn Unusual Case of Lower Gastrointestinal HemorrhatessalaiNo ratings yet
- Utility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotDocument3 pagesUtility of Endoscopic Ultrasound in Symptomatic Cut Corners of A ClotDjabhi SpinzzNo ratings yet
- ChangDocument3 pagesChangAmirullah AbdiNo ratings yet
- ABDOMINAL Assesory LiverDocument4 pagesABDOMINAL Assesory Liverwelly_hartonoNo ratings yet
- A Case Study of Mesenteric Ischemia by Low Flow CT ImagingDocument5 pagesA Case Study of Mesenteric Ischemia by Low Flow CT ImagingAmanda SmithNo ratings yet
- Case Report: Hepatic Artery Aneurysm.a Rare Visceral AneurysmDocument5 pagesCase Report: Hepatic Artery Aneurysm.a Rare Visceral AneurysmIJAR JOURNALNo ratings yet
- Electronic Image of The Month: A Rare Tumor of The Common Hepatic Duct Causing Biliary ObstructionDocument2 pagesElectronic Image of The Month: A Rare Tumor of The Common Hepatic Duct Causing Biliary ObstructionDeborah Anasthasia PakpahanNo ratings yet
- E-Poster Mumbai FinalDocument5 pagesE-Poster Mumbai FinalSuman SagarNo ratings yet
- Liver Trauma: Vic Vernenkar, D.O. St. Barnabas HospitalDocument24 pagesLiver Trauma: Vic Vernenkar, D.O. St. Barnabas HospitalAna CotomanNo ratings yet
- Biliary Duct ImagingDocument7 pagesBiliary Duct ImagingImam FahriNo ratings yet
- Gastroduodenal Artery Pseudoaneurysm and Aberrant Right Hepatic ArteryDocument3 pagesGastroduodenal Artery Pseudoaneurysm and Aberrant Right Hepatic ArteryGordana PuzovicNo ratings yet
- Case 12669Document15 pagesCase 12669Putrisuci AndytichaNo ratings yet
- Utd 32654 Case - Reports AydinDocument3 pagesUtd 32654 Case - Reports AydinDavid LopezNo ratings yet
- ZZ - 2006-07 - Pancreatic Pseudocyst Bleeding Associated With Massive Intraperitoneal HemorrhageDocument2 pagesZZ - 2006-07 - Pancreatic Pseudocyst Bleeding Associated With Massive Intraperitoneal HemorrhageNawzad SulayvaniNo ratings yet
- The Role of Ultrasonography in The Evaluation of Diffuse Liver DiseaseDocument13 pagesThe Role of Ultrasonography in The Evaluation of Diffuse Liver Disease{Phantom}No ratings yet
- Spontaneous Rupture of Hepatocellular Carcinoma in A Healthy Liver: A Case ReportDocument6 pagesSpontaneous Rupture of Hepatocellular Carcinoma in A Healthy Liver: A Case ReportIJAR JOURNALNo ratings yet
- Knots and Knives - 3rd EditionsDocument4 pagesKnots and Knives - 3rd EditionsNasser AlbaddaiNo ratings yet
- 2015 Article 79Document6 pages2015 Article 79Alfeus GradyNo ratings yet
- Diagnosis and Management of Splanchnic Ischemia: Ioannis E Koutroubakis, MD, PHD, Assistant Professor of MedicineDocument12 pagesDiagnosis and Management of Splanchnic Ischemia: Ioannis E Koutroubakis, MD, PHD, Assistant Professor of MedicineIgorCotagaNo ratings yet
- Gallbladder Wall ThickeningDocument16 pagesGallbladder Wall ThickeningAnonymous FCOOcnNo ratings yet
- Case 12118: Post-Laparoscopic Cholecystectomy Abdominal Wall BilomaDocument8 pagesCase 12118: Post-Laparoscopic Cholecystectomy Abdominal Wall BilomaliaNo ratings yet
- Inferior Mesenteric Arteriovenous Fistula With Ischemic Colitis: Multidetector Computed Tomographic Angiography For DiagnosisDocument4 pagesInferior Mesenteric Arteriovenous Fistula With Ischemic Colitis: Multidetector Computed Tomographic Angiography For DiagnosisGordana PuzovicNo ratings yet
- ArcuatoDocument7 pagesArcuatoDaniela PekeNo ratings yet
- Laparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaDocument4 pagesLaparoscopic Cholecystectomy After Conservative Su - 2024 - International JournaRonald QuezadaNo ratings yet
- Erik Pancreatic TraumaDocument31 pagesErik Pancreatic TraumaIgnatius JesinNo ratings yet
- Pancreatic Pseudocyst EDITEDDocument5 pagesPancreatic Pseudocyst EDITEDLaura LatifaNo ratings yet
- Liver Review: Vic Vernenkar, D.O. St. Barnabas Hospital Bronx, NYDocument72 pagesLiver Review: Vic Vernenkar, D.O. St. Barnabas Hospital Bronx, NYLouis FortunatoNo ratings yet
- ABC Emergency Differential DiagnosisffDocument3 pagesABC Emergency Differential Diagnosisffsharu4291No ratings yet
- Jurnal DinaDocument11 pagesJurnal DinaRahma Puji LestariNo ratings yet
- Ethanol and Polyvinyl Alcohol Mixture For Transcatheter Embolization of Renal AngiomyolipomaDocument13 pagesEthanol and Polyvinyl Alcohol Mixture For Transcatheter Embolization of Renal AngiomyolipomaJeffryandiNo ratings yet
- Step 2ck Important (AutoRecovered)Document101 pagesStep 2ck Important (AutoRecovered)Aishwarya SridharNo ratings yet
- Hepatocellular Carcinoma - Diagnosis and TreatmentDocument46 pagesHepatocellular Carcinoma - Diagnosis and TreatmentSigh BalaNo ratings yet
- Chapter 10 Sonographic Approach To Acute Abdominal PainDocument13 pagesChapter 10 Sonographic Approach To Acute Abdominal PainSyed Shahrul Naz SyedNo ratings yet
- 10.1007@s00261 019 02340 5Document25 pages10.1007@s00261 019 02340 5Pablo Henrique Alves TelesNo ratings yet
- Large and Bleeding Gastroduodenal Artery Aneurysm 2024 International JournalDocument5 pagesLarge and Bleeding Gastroduodenal Artery Aneurysm 2024 International JournalRonald QuezadaNo ratings yet
- Kolangitis Case 1Document6 pagesKolangitis Case 1Dhen Mas PrimanaNo ratings yet
- Aghiz 3Document12 pagesAghiz 3nandaaa aprilNo ratings yet
- Imaging of The Porta HepatisDocument71 pagesImaging of The Porta Hepatisjskmkabongo100% (1)
- Pancreatic Adenocarcinoma Mimicking PseudocystDocument3 pagesPancreatic Adenocarcinoma Mimicking PseudocystInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ZZ - 1999-12 - Massive Intraperitoneal Hemorrhage From A Pancreatic PseudocystDocument4 pagesZZ - 1999-12 - Massive Intraperitoneal Hemorrhage From A Pancreatic PseudocystNawzad SulayvaniNo ratings yet
- Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy For Pseudomyxoma Peritonei in A Liver-Transplanted Patient: A Case ReportDocument5 pagesCytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy For Pseudomyxoma Peritonei in A Liver-Transplanted Patient: A Case Reportyerich septaNo ratings yet
- Diagnostic Imaging Pathways Article PDFDocument12 pagesDiagnostic Imaging Pathways Article PDFchald ald smithNo ratings yet
- Mesenteric Artery Ischemia PDFDocument30 pagesMesenteric Artery Ischemia PDFMerfat MahyobeNo ratings yet
- BookDocument21 pagesBookShaastieNo ratings yet
- Upper Gastrointestinal Bleeding (UGIB) : Practice EssentialsDocument52 pagesUpper Gastrointestinal Bleeding (UGIB) : Practice EssentialsrishaNo ratings yet
- The Hebrew and Greek Scriptures ComparedDocument805 pagesThe Hebrew and Greek Scriptures Comparedreha-kauba100% (1)
- Zeal IngredientsDocument4 pagesZeal IngredientsRob HarnageNo ratings yet
- Engine: Machine Energy Mechanical EnergyDocument79 pagesEngine: Machine Energy Mechanical Energyshubhamvpathade03No ratings yet
- Rocks and Minerals Webquest Justin PowersDocument2 pagesRocks and Minerals Webquest Justin Powersapi-264089789100% (1)
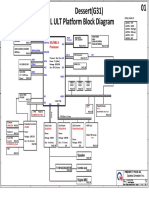
- Quanta G31a Dag31amb6d0 Y61x-6l Rev 1aDocument49 pagesQuanta G31a Dag31amb6d0 Y61x-6l Rev 1aKrystian PalaciosNo ratings yet
- Calibracion Motor Aceleracion 320CDocument12 pagesCalibracion Motor Aceleracion 320CJoan CardonaNo ratings yet
- Foundation Settlements: Settlement of Shallow Foundation in Cohesive SoilDocument16 pagesFoundation Settlements: Settlement of Shallow Foundation in Cohesive SoilBashdar M. TahirNo ratings yet
- Knürr DCM: ® Modular Rack Platform - For Future-Proof Data CentersDocument36 pagesKnürr DCM: ® Modular Rack Platform - For Future-Proof Data CentersAlex GuyNo ratings yet
- Human Activity Detection Using Deep - 2-1Document8 pagesHuman Activity Detection Using Deep - 2-1Riky Tri YunardiNo ratings yet
- Preparing For EnemaDocument11 pagesPreparing For Enemapassion26100% (1)
- Pre-Lab InformationDocument8 pagesPre-Lab InformationSusnata SamantaNo ratings yet
- Readers Theater For Grade OneDocument9 pagesReaders Theater For Grade OneglaidzNo ratings yet
- Alchemist Guide ProductionsDocument23 pagesAlchemist Guide ProductionsNovi NovianNo ratings yet
- Lesson Plann Highschool FullDocument3 pagesLesson Plann Highschool Fullapi-329957578No ratings yet
- Osteoporosis: Osteoporosis - Devashish Kumar 27701913031 (4th Year, 7 Sem) 27701913031Document12 pagesOsteoporosis: Osteoporosis - Devashish Kumar 27701913031 (4th Year, 7 Sem) 27701913031amish rajNo ratings yet
- AsDocument777 pagesAsCristhian QuimizNo ratings yet
- SONY AA-2U Chassis ServiceManualLiteDocument11 pagesSONY AA-2U Chassis ServiceManualLitememotecNo ratings yet
- TB Chapter1Document3 pagesTB Chapter1fayeNo ratings yet
- Beating The Bonk QuestionsDocument1 pageBeating The Bonk Questionst3xxaNo ratings yet
- MOBILE - WASTE - MANAGEMENT - in - PDF PDFDocument14 pagesMOBILE - WASTE - MANAGEMENT - in - PDF PDFAmayNo ratings yet
- UntitledDocument45 pagesUntitledaina ainaNo ratings yet
- Types of PelvisDocument23 pagesTypes of PelvisChinju Jose SajithNo ratings yet
- Site Installation Standard - Ver 20200706Document179 pagesSite Installation Standard - Ver 20200706Kyaw Kyaw WinNo ratings yet
- Buku JawapanDocument15 pagesBuku JawapanSivaashini Balamuraly RajaNo ratings yet
- BBS of All Pier Foundations of MAYARDocument16 pagesBBS of All Pier Foundations of MAYARAmanjot Singh0% (1)
- Comment Sheet No SPO 16 01289Document5 pagesComment Sheet No SPO 16 01289juel19No ratings yet
- Trade of Export - ImportDocument9 pagesTrade of Export - ImportrahulvaliyaNo ratings yet
- Vapor and Combined Power CyclesDocument33 pagesVapor and Combined Power CyclesOtuagaNo ratings yet
- PhySciSHS Q4 Week1Document46 pagesPhySciSHS Q4 Week1Roseman TumaliuanNo ratings yet
- A Study On Distribution Strategies of Hindustan Unilever Limited by Rajnikant GharatDocument31 pagesA Study On Distribution Strategies of Hindustan Unilever Limited by Rajnikant GharatRajnikant GharatNo ratings yet