Download as pdf or txt
You might also like
- Gender-Responsive Lgu (Gerl) Assessment ToolDocument42 pagesGender-Responsive Lgu (Gerl) Assessment ToolDyanne Kristine Almirante Sideño100% (8)
- Chronic Suppurative Otitis Media in AdultsDocument10 pagesChronic Suppurative Otitis Media in AdultsRstadam TagalogNo ratings yet
- CPG On CsomDocument8 pagesCPG On CsomRobert Ross DulayNo ratings yet
- Esophageal EmergenciesDocument15 pagesEsophageal EmergenciesOmar SolisNo ratings yet
- Review of Ingested Aspirated Foreign Bodies Art Radiographics 2015Document11 pagesReview of Ingested Aspirated Foreign Bodies Art Radiographics 2015manuel arenas floresNo ratings yet
- 39 - 2017-05-074 - DR Aftab AnwarDocument5 pages39 - 2017-05-074 - DR Aftab AnwarAftabAnwarNo ratings yet
- Foreign Body Ingestion and Aspiration in Dentistry: A Review of The Literature and Reports of Three CasesDocument8 pagesForeign Body Ingestion and Aspiration in Dentistry: A Review of The Literature and Reports of Three CasesgheaastridgayatriNo ratings yet
- Late Diagnosis of Foreign Body Aspiration in A Libyan Infant With Chronic Respiratory Problems A Challenging DiagnosisDocument4 pagesLate Diagnosis of Foreign Body Aspiration in A Libyan Infant With Chronic Respiratory Problems A Challenging DiagnosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- International Journal of Surgery Case Reports: Unusual Esophageal Foreign Body in Neonates: A Case ReportDocument4 pagesInternational Journal of Surgery Case Reports: Unusual Esophageal Foreign Body in Neonates: A Case ReportmusdalifahNo ratings yet
- Diagnostic Decision-Making Tool For ImagingDocument9 pagesDiagnostic Decision-Making Tool For ImagingGuillermo Andrés AriasNo ratings yet
- Sonography - 2024 - Deslandes - Are Sonographers The Future Gold Standard in The Diagnosis of EndometriosisDocument9 pagesSonography - 2024 - Deslandes - Are Sonographers The Future Gold Standard in The Diagnosis of EndometriosisfuwadongNo ratings yet
- Paediatric Urology - Peno-Scrotal: Case 1 Case 2Document2 pagesPaediatric Urology - Peno-Scrotal: Case 1 Case 2HardiTariqHammaNo ratings yet
- Diagnostic DecisionDocument9 pagesDiagnostic DecisionfrigandraNo ratings yet
- Safety of Intravenous Iodinated Contrast Medium inDocument6 pagesSafety of Intravenous Iodinated Contrast Medium inNealNo ratings yet
- Removal of Foreign Body (Glass of Mirror) in Esophagus With Direct LaryngoscopeDocument7 pagesRemoval of Foreign Body (Glass of Mirror) in Esophagus With Direct LaryngoscopeSafira SalsabilaNo ratings yet
- Cuerpo Extraño en El RectoDocument5 pagesCuerpo Extraño en El RectoMiguel Angel Hernandez SerratoNo ratings yet
- Case EsophagosDocument11 pagesCase EsophagosfrinadyaNo ratings yet
- J Paediatrics Child Health - 2022 - Sandy - Thyroid Nodules in Children and Adolescents Investigation and ManagementDocument6 pagesJ Paediatrics Child Health - 2022 - Sandy - Thyroid Nodules in Children and Adolescents Investigation and ManagementIqbal RifaiNo ratings yet
- Management of Foreign Body Dentures' With Esophagoscopy: A Case ReportDocument8 pagesManagement of Foreign Body Dentures' With Esophagoscopy: A Case ReportfrinadyaNo ratings yet
- Advances in Gerd: Esophageal Foreign Bodies and Food ImpactionsDocument3 pagesAdvances in Gerd: Esophageal Foreign Bodies and Food ImpactionsHalbar August KandaNo ratings yet
- Ultrasound Findings in Paediatric Cholestasis How To Image The Patient and What To Look ForDocument12 pagesUltrasound Findings in Paediatric Cholestasis How To Image The Patient and What To Look ForintanNo ratings yet
- The Cell Phone in The Twenty-First Century - Risk For Addiction or Ingestion - Case Report and Review of The LiteratureDocument2 pagesThe Cell Phone in The Twenty-First Century - Risk For Addiction or Ingestion - Case Report and Review of The LiteraturejernsssNo ratings yet
- Ding 2020Document6 pagesDing 2020Ridha Aswina DalimuntheNo ratings yet
- Art 2Document6 pagesArt 2Cristian OneaNo ratings yet
- Prenatal Diagnosis of Harlequin Ichthyosis: A Case ReportDocument4 pagesPrenatal Diagnosis of Harlequin Ichthyosis: A Case Reportcitra annisa fitriNo ratings yet
- Jurnal 3Document6 pagesJurnal 3Dheana IsmaniarNo ratings yet
- I'Alji, Hamilton, 1.0s 4ngeles, Ctrlif.: Which AreDocument4 pagesI'Alji, Hamilton, 1.0s 4ngeles, Ctrlif.: Which AreAmalorNo ratings yet
- Accidental File SwallowingDocument6 pagesAccidental File SwallowingShivani DubeyNo ratings yet
- Emergencias Respiratorias Pediatricas PDFDocument20 pagesEmergencias Respiratorias Pediatricas PDFMarco Antonio Mendoza OjedaNo ratings yet
- Literature Review Otitis MediaDocument4 pagesLiterature Review Otitis Mediaamjatzukg100% (1)
- Cute Appendicitis in Children: Emergency Department Diagnosis and ManagementDocument13 pagesCute Appendicitis in Children: Emergency Department Diagnosis and ManagementMusyawarah MelalaNo ratings yet
- Researcharticle Open Access: BackgroundDocument4 pagesResearcharticle Open Access: BackgroundMagfira Al HabsyiNo ratings yet
- 2019 - Appendicular Perforation in A NeonateDocument3 pages2019 - Appendicular Perforation in A NeonateRevivo RindaNo ratings yet
- Medscape Pediatric Foreign Body IngestionDocument15 pagesMedscape Pediatric Foreign Body IngestionFrancisca VillalobosNo ratings yet
- J of Inher Metab Disea 2023 Spiekerkoetter Genomic Newborn Screening Are We Entering A New Era of ScreeningDocument18 pagesJ of Inher Metab Disea 2023 Spiekerkoetter Genomic Newborn Screening Are We Entering A New Era of ScreeningMarianne Angela CortezNo ratings yet
- 2015 Management of Ingested Foreign Bodies in Children - A Clinical Report of The NASPGHAN Endoscopy CommitteeDocument13 pages2015 Management of Ingested Foreign Bodies in Children - A Clinical Report of The NASPGHAN Endoscopy CommitteeCarlos CuadrosNo ratings yet
- Congenital Cataract-Approach and Management ReviewDocument6 pagesCongenital Cataract-Approach and Management ReviewFirgietaPotterNo ratings yet
- Acta Ophthalmologica - 2018 - Rasul - Prevalence of Anterior Polar Cataracts in Children and Risk Factors For AmblyopiaDocument5 pagesActa Ophthalmologica - 2018 - Rasul - Prevalence of Anterior Polar Cataracts in Children and Risk Factors For AmblyopiaMarta GuerreiroNo ratings yet
- Comparison of PCR, Culturing and Pap Smear Microscopy For Accurate Diagnosis of Genital ActinomycesDocument7 pagesComparison of PCR, Culturing and Pap Smear Microscopy For Accurate Diagnosis of Genital Actinomycestitaamalinda28No ratings yet
- 1 s2.0 S003962571630090X MainDocument14 pages1 s2.0 S003962571630090X MainBenjamin NgNo ratings yet
- Removal of Ear, Nose andDocument4 pagesRemoval of Ear, Nose andandinNo ratings yet
- Original Research Article: ISSN: 2230-9926Document7 pagesOriginal Research Article: ISSN: 2230-9926Fatma ElzaytNo ratings yet
- 0 EbfDocument10 pages0 EbfdewaprasatyaNo ratings yet
- L1 - Actinomyces and NocardiaDocument45 pagesL1 - Actinomyces and Nocardiadvph2fck6qNo ratings yet
- Supplemetary ExaminationDocument32 pagesSupplemetary ExaminationSally ElhadadNo ratings yet
- AUR in ChildrenDocument1 pageAUR in ChildrenStaporn KasemsripitakNo ratings yet
- Impact of COVID Lockdown On The Presentation of NaDocument6 pagesImpact of COVID Lockdown On The Presentation of NaSuparna Roy VarunNo ratings yet
- Review: Lucia Romani, Andrew C Steer, Margot J Whitfeld, John M KaldorDocument8 pagesReview: Lucia Romani, Andrew C Steer, Margot J Whitfeld, John M KaldorMuhammad AmrullahNo ratings yet
- Evaluation of The Predictability of Clinical and Radiological Findings in The Diagnosis of MalrotationDocument8 pagesEvaluation of The Predictability of Clinical and Radiological Findings in The Diagnosis of MalrotationElna EstherNo ratings yet
- Dental Foreign Body EngulfmentDocument4 pagesDental Foreign Body EngulfmentShivani DubeyNo ratings yet
- Jurnal AppendicitisDocument3 pagesJurnal AppendicitismaulidaangrainiNo ratings yet
- Scabies Outbreaks in Ten Care Homes For Elderly People: A Prospective Study of Clinical Features, Epidemiology, and Treatment OutcomesDocument9 pagesScabies Outbreaks in Ten Care Homes For Elderly People: A Prospective Study of Clinical Features, Epidemiology, and Treatment OutcomesyoggihermawanNo ratings yet
- Journal of Pediatric Surgery Case Reports: Moaied A. Hassan, Hasan K. Gatea, Thura K. Ja'afar, Ahmed O. Fahad TDocument3 pagesJournal of Pediatric Surgery Case Reports: Moaied A. Hassan, Hasan K. Gatea, Thura K. Ja'afar, Ahmed O. Fahad TVero MeidyNo ratings yet
- Jaundice 2Document5 pagesJaundice 2Ie DochieNo ratings yet
- Congenital Palpebral Eversion A New Conservative Management Method About Four CasesDocument10 pagesCongenital Palpebral Eversion A New Conservative Management Method About Four CasesAthenaeum Scientific PublishersNo ratings yet
- Time For A Farewell To Soap in The Eye?Document4 pagesTime For A Farewell To Soap in The Eye?yazzNo ratings yet
- 389-Article Text-469-1-10-20151016Document4 pages389-Article Text-469-1-10-20151016khaled alahmadNo ratings yet
- International Journal of Surgery Case ReportsDocument3 pagesInternational Journal of Surgery Case ReportsDr David NekouNo ratings yet
- Case Reports Esophageal Foreign Body in NeonatesDocument3 pagesCase Reports Esophageal Foreign Body in NeonatesmuhammadpanggihpangestuNo ratings yet
- Apgh 3 1Document2 pagesApgh 3 1Rashmi Ranjan BeheraNo ratings yet
- 5-Who Donates MoreDocument5 pages5-Who Donates Morescribdnotes123No ratings yet
- Class 11 - EDocument7 pagesClass 11 - EAnitha SathiaseelanNo ratings yet
- Case Report FinalDocument21 pagesCase Report FinalAyen FornollesNo ratings yet
- The Tyranny of Neuronormativity QuestionDocument16 pagesThe Tyranny of Neuronormativity QuestionSandra SandersNo ratings yet
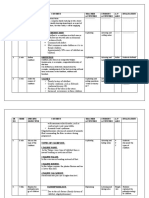
- SR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationDocument16 pagesSR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationJuhi Johnson JadhavNo ratings yet
- 2023 Pca CV Expert Panel Virtual Meeting - Pre-ReadDocument48 pages2023 Pca CV Expert Panel Virtual Meeting - Pre-ReadPashoKiatNo ratings yet
- Ce Patient and Family Education Prevention of Elder AbuseDocument1 pageCe Patient and Family Education Prevention of Elder Abuseapi-532613659No ratings yet
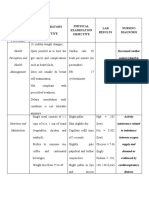
- Gordon'S Functiona L Health Pattern Nursing History Subjective Physical Examination Objective LAB Results Nursing DiagnosisDocument4 pagesGordon'S Functiona L Health Pattern Nursing History Subjective Physical Examination Objective LAB Results Nursing DiagnosischarmaineNo ratings yet
- Health Status of Manitobans ReportDocument78 pagesHealth Status of Manitobans ReportCityNewsTorontoNo ratings yet
- HESI Women's Health:Newborn DrugsDocument8 pagesHESI Women's Health:Newborn Drugsisapatrick8126No ratings yet
- JMYKo OncologyReports 2014Document12 pagesJMYKo OncologyReports 2014vikram413No ratings yet
- CHC33015-AC-HACC-Subject 4-AWB-F-v2.5Document45 pagesCHC33015-AC-HACC-Subject 4-AWB-F-v2.5Ashesh Basnet100% (6)
- Revalida Exam 200 ItemsDocument18 pagesRevalida Exam 200 Itemsxaileenx0% (1)
- Prak ParuDocument17 pagesPrak Paruhan jisungNo ratings yet
- BHS InggrisDocument5 pagesBHS InggrisDeajeng Febby AyuNo ratings yet
- Inserto Fibrinogeno SIEMENSDocument5 pagesInserto Fibrinogeno SIEMENSedson floresNo ratings yet
- Selective GrindingDocument4 pagesSelective Grindingnieta antoNo ratings yet
- STD - Infection That Are Passed From One Person To Another Through Sexual Contact. The Causes of StdsDocument3 pagesSTD - Infection That Are Passed From One Person To Another Through Sexual Contact. The Causes of StdsAngela BeatriceNo ratings yet
- Desain Penugasan KMB III Tranfer Ko EniDocument7 pagesDesain Penugasan KMB III Tranfer Ko EniAhmad NajibNo ratings yet
- Sections of Lab - EssayDocument3 pagesSections of Lab - EssayhalamanNo ratings yet
- NCP Ineffective Breathing PatternDocument4 pagesNCP Ineffective Breathing PatternSeika SouiNo ratings yet
- Mapeh7 q1 Melc4 Growthanddeelopment v1Document32 pagesMapeh7 q1 Melc4 Growthanddeelopment v1NICKY SANCHEZNo ratings yet
- HS-Series Instruction Manual 4HS / 6HS: Reciprocating CompressorDocument151 pagesHS-Series Instruction Manual 4HS / 6HS: Reciprocating CompressornavNo ratings yet
- Perceptions of Cultural Competence in The New Zealand Speech Language Therapy Profession PDFDocument14 pagesPerceptions of Cultural Competence in The New Zealand Speech Language Therapy Profession PDFsara almashabiNo ratings yet
- s40279 022 01797 7Document12 pagess40279 022 01797 7juan sebastian chaverra apraezNo ratings yet
- Original Contribution: The SHEZ StudyDocument9 pagesOriginal Contribution: The SHEZ StudyRaúl AñariNo ratings yet
- Enem 2019 Primeiro DiaDocument24 pagesEnem 2019 Primeiro DiaSouza RozNo ratings yet
- Principles of Drug ActionDocument42 pagesPrinciples of Drug ActionsharmamtechNo ratings yet