Download as docx, pdf, or txt
You might also like
- PASSMEDICINE MRCP MCQs-PALLIATIVE MEDICINE AND END OF LIFE CAREDocument17 pagesPASSMEDICINE MRCP MCQs-PALLIATIVE MEDICINE AND END OF LIFE CAREHashim Ahmad100% (4)
- Echocardiographic Atlas of Adult Congenital Heart Disease: Hakimeh Sadeghian Zahra Savand-RoomiDocument486 pagesEchocardiographic Atlas of Adult Congenital Heart Disease: Hakimeh Sadeghian Zahra Savand-RoomiGeorgiana-Gratiela MalaescuNo ratings yet
- Cardio Pharma MeDocument23 pagesCardio Pharma Memohammed.sheeb.yesNo ratings yet
- Drugs Used in The Treatment of Cardiac Failure: Assoc. Prof. Iv. Lambev WWW - Medpharm-Sofia - EuDocument38 pagesDrugs Used in The Treatment of Cardiac Failure: Assoc. Prof. Iv. Lambev WWW - Medpharm-Sofia - EuYeshaa MiraniNo ratings yet
- 9 Drugs Affecting Angina PectorisDocument3 pages9 Drugs Affecting Angina PectoristiaraNo ratings yet
- Anti Anginal DrugsDocument60 pagesAnti Anginal DrugsPranish SawantNo ratings yet
- Case Study Number 1Document5 pagesCase Study Number 1Kevin Kyle RizarriNo ratings yet
- L6 Angina Practice EssayDocument2 pagesL6 Angina Practice EssaymoshlingmomoNo ratings yet
- CVS (HF, HTN) PharmacologyDocument99 pagesCVS (HF, HTN) PharmacologyCherenet TomaNo ratings yet
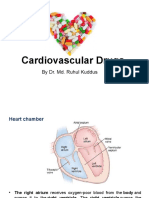
- Cardiovascular Drugs: by Dr. Md. Ruhul KuddusDocument56 pagesCardiovascular Drugs: by Dr. Md. Ruhul Kuddus53-Deepankar SutradharNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of SubmissionDocument10 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of SubmissionAnoosha FarooquiNo ratings yet
- Angiotensin Receptor Blockers (O)Document26 pagesAngiotensin Receptor Blockers (O)farmasi_hmNo ratings yet
- Cardio Lab MedsDocument11 pagesCardio Lab MedsDianne Erika MeguinesNo ratings yet
- C C C CDocument7 pagesC C C CMadel de GuzmanNo ratings yet
- Generic Name Brand Name Drug Class Mechanism of Action StructureDocument4 pagesGeneric Name Brand Name Drug Class Mechanism of Action StructurenoelkiddoNo ratings yet
- Year 2 RevisionDocument3 pagesYear 2 RevisionCozNo ratings yet
- Blood Drugs Chapter + NotesDocument23 pagesBlood Drugs Chapter + NotesNormana ZureikatNo ratings yet
- Heat Failure DrugsDocument8 pagesHeat Failure DrugsDaniel MwiluNo ratings yet
- Lec 2 Heart Failure, Angina and Arryth2Document19 pagesLec 2 Heart Failure, Angina and Arryth2Adel AlomarNo ratings yet
- Pharmacotherapy of Congestive Heart Failure (CHF)Document163 pagesPharmacotherapy of Congestive Heart Failure (CHF)Aditya rathoreNo ratings yet
- Case Presentation On Ischemic Cardiomyopathy & Ccf-1-1Document18 pagesCase Presentation On Ischemic Cardiomyopathy & Ccf-1-1Maliha aliNo ratings yet
- LEC#13 ACE InhibitotsDocument37 pagesLEC#13 ACE Inhibitotsalihyderabro166No ratings yet
- E Cart MedicationsDocument12 pagesE Cart Medicationsbalong1219No ratings yet
- Anti Hypertensive 20191211Document35 pagesAnti Hypertensive 20191211helloitsmenadNo ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- Modul Drugs Used in Congestive Heart Failure 11 Nov 2010Document12 pagesModul Drugs Used in Congestive Heart Failure 11 Nov 2010Dian NugraNo ratings yet
- ACE IsDocument37 pagesACE IsPriyanshi ShahNo ratings yet
- Antihypertensive AgentsDocument52 pagesAntihypertensive Agentssameena ramzanNo ratings yet
- Meds #1 NotesDocument4 pagesMeds #1 NotesAnh TrinhNo ratings yet
- Hypertension TejaDocument64 pagesHypertension TejaAnushka MaheshwariNo ratings yet
- Cardiac GlycosidesDocument8 pagesCardiac GlycosidesShan Sicat100% (1)
- Drugs Affecting Renin-Angiotensin SystemDocument23 pagesDrugs Affecting Renin-Angiotensin SystemrajeswariNo ratings yet
- Adobe Scan Aug 20, 2022Document11 pagesAdobe Scan Aug 20, 2022RsNo ratings yet
- منار كمDocument61 pagesمنار كمFemale calmNo ratings yet
- Physiology RAASDocument3 pagesPhysiology RAASAulia Mahya FaradisaNo ratings yet
- Drugs Acting On The Renin-Angiotensin-Aldosterone SystemDocument2 pagesDrugs Acting On The Renin-Angiotensin-Aldosterone SystemKate EvangelistaNo ratings yet
- Empagliflozin Related To Ketoacidosis and Early Neurological Deterioration in A Patient With Acute Ischemic StrokeDocument9 pagesEmpagliflozin Related To Ketoacidosis and Early Neurological Deterioration in A Patient With Acute Ischemic Stroke王湘淇No ratings yet
- Antianginal DrugsDocument38 pagesAntianginal Drugslemmademe204No ratings yet
- Inhibitors of AngiotensinDocument37 pagesInhibitors of AngiotensinBoyu GrtrNo ratings yet
- Antihypertensive Drugs: HypertensionDocument8 pagesAntihypertensive Drugs: Hypertensionalmastar officeNo ratings yet
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
- Pharmacology Assignment 3Document31 pagesPharmacology Assignment 3Tujiyye kooNo ratings yet
- Adrenergic Antagonist 2 (Propranolol)Document5 pagesAdrenergic Antagonist 2 (Propranolol)ziad shahinNo ratings yet
- Antianginal Drugs Lecture NotesDocument10 pagesAntianginal Drugs Lecture NotesPrincewill SeiyefaNo ratings yet
- Patogenesis Diabetic NefropatiDocument9 pagesPatogenesis Diabetic Nefropatikonas patklinNo ratings yet
- Lecture 15 - Polypeptides - 16 Oct 2006Document63 pagesLecture 15 - Polypeptides - 16 Oct 2006api-3703352No ratings yet
- CardiologyDocument20 pagesCardiologycnnc21No ratings yet
- 4 - Anti-AnginaDocument6 pages4 - Anti-AnginaJericho De GuzmanNo ratings yet
- Genxraver Girl Interrupted Usmle Step 2 Notes PDFDocument259 pagesGenxraver Girl Interrupted Usmle Step 2 Notes PDFughbuzzoffNo ratings yet
- Congestive Cardiac FailureDocument27 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- 5-Heart FailureDocument12 pages5-Heart FailureJericho De GuzmanNo ratings yet
- CONGESTIVE HEART FAILURE - New-1Document32 pagesCONGESTIVE HEART FAILURE - New-1Agus SuprionoNo ratings yet
- 10 and 11 Treatment of Hypertension and AnginaDocument10 pages10 and 11 Treatment of Hypertension and AnginaBrandon AviciiNo ratings yet
- Anti Anginal Drugs - Wards HandooutDocument24 pagesAnti Anginal Drugs - Wards HandooutDharun RanganathanNo ratings yet
- Mechanism of Action: Cerebral VasospasmDocument1 pageMechanism of Action: Cerebral VasospasmArjay Oamil GuerreroNo ratings yet
- Product Manual ChronicDocument56 pagesProduct Manual ChronicsubhojitnayekNo ratings yet
- ACE Inhibitors & Angiotensin II Antagonists: October 1997Document4 pagesACE Inhibitors & Angiotensin II Antagonists: October 1997indee533No ratings yet
- Antianginal DrugsDocument25 pagesAntianginal DrugsTamta BokoveliNo ratings yet
- CarvedilolDocument4 pagesCarvedilolGoNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Fast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteFrom EverandFast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteNo ratings yet
- OsceDocument11 pagesOscedocali11No ratings yet
- HA Transes LEC 1Document14 pagesHA Transes LEC 1honti018No ratings yet
- Diuretic DrugsDocument62 pagesDiuretic DrugsAbdul WahabNo ratings yet
- 3 Animal Physiology Cie Preu Biology QPDocument17 pages3 Animal Physiology Cie Preu Biology QPPaulius SungailaNo ratings yet
- General Population (No Diabetes or CKD) Diabetes or CKD PresentDocument2 pagesGeneral Population (No Diabetes or CKD) Diabetes or CKD PresentLalu Ranova100% (1)
- Dr. Limpin - Epidemiology of SmokingDocument32 pagesDr. Limpin - Epidemiology of SmokingAnil Kumar Jr.No ratings yet
- Long Presentation HEMORRHAGE AND SHOCKDocument33 pagesLong Presentation HEMORRHAGE AND SHOCKJoy JoycNo ratings yet
- Program Zilele UMF 2016 Sesiune Doctoranzi-Cadre DidDocument22 pagesProgram Zilele UMF 2016 Sesiune Doctoranzi-Cadre DidCătălin ŞuteuNo ratings yet
- Gallstone Disease and The Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Observational StudiesDocument7 pagesGallstone Disease and The Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Observational StudiesAfkar30No ratings yet
- Medical Auditing Training: CPMA®: Practical Application WorkbookDocument32 pagesMedical Auditing Training: CPMA®: Practical Application WorkbookAnthony El HageNo ratings yet
- Hypertrophic CardiomyopathyDocument57 pagesHypertrophic CardiomyopathycynNo ratings yet
- Gastric Outlet ObstructionDocument10 pagesGastric Outlet ObstructionMpanso Ahmad AlhijjNo ratings yet
- Normal Adult 12-Lead ECGDocument2 pagesNormal Adult 12-Lead ECGIlonaNo ratings yet
- Relevant Equine Renal Anatomy, Physiology and Mechanisms of AKI ReviewDocument12 pagesRelevant Equine Renal Anatomy, Physiology and Mechanisms of AKI ReviewMarilú ValdepeñaNo ratings yet
- 3Document13 pages3Urologi Unpad Februari 2023No ratings yet
- Rincian Kewenangan Klinis AnakDocument6 pagesRincian Kewenangan Klinis AnakUchiha ItachiNo ratings yet
- WEEK 8 LAB EXERCISE - CVS & Bood VesselsDocument6 pagesWEEK 8 LAB EXERCISE - CVS & Bood VesselsJoselito JardielNo ratings yet
- Checklist For Cardiac AssessmentDocument3 pagesChecklist For Cardiac AssessmentCake ManNo ratings yet
- MS Practice QuizDocument42 pagesMS Practice QuizMarah PacioNo ratings yet
- Catatan KodingDocument51 pagesCatatan KodingYudhawan AgamNo ratings yet
- Aortic DissectionDocument2 pagesAortic DissectionTiffney NesakumarNo ratings yet
- Obstetric Disorders and Critical Illness - 2022 - Clinics in Chest MedicineDocument18 pagesObstetric Disorders and Critical Illness - 2022 - Clinics in Chest MedicineGustavo ParedesNo ratings yet
- Beta BlockerDocument8 pagesBeta BlockerZiedTriki100% (1)
- Echobasics, Sys FXNDocument5 pagesEchobasics, Sys FXNJing CruzNo ratings yet
- 1 s2.0 S1930043324001298 MainDocument6 pages1 s2.0 S1930043324001298 Mainaakash singhNo ratings yet
- Pancreas MRI Planning - Indications For MRI Pancreas Scan - MRI Pancreas ProtocolsDocument8 pagesPancreas MRI Planning - Indications For MRI Pancreas Scan - MRI Pancreas ProtocolsgshunnarNo ratings yet
- Dissertation Submitted To The: KNR University of Health Sciences, WarangalDocument55 pagesDissertation Submitted To The: KNR University of Health Sciences, Warangalmarri manasaNo ratings yet
- Amboss - GITDocument16 pagesAmboss - GITAllysahNo ratings yet