Download as pdf or txt
You might also like
- Bar Closing ChecklistDocument2 pagesBar Closing ChecklistChef Shane100% (2)
- Part 4abcDocument56 pagesPart 4abcMatthew Guevarra91% (11)
- FMCG Sector ProjectDocument66 pagesFMCG Sector ProjectTUSHAR MANDALENo ratings yet
- Some Extraordinary Facts About Obese Humans and Rats: Columbia UniversityDocument16 pagesSome Extraordinary Facts About Obese Humans and Rats: Columbia UniversityAna Sofia Almeida100% (1)
- 7-Eleven JapanDocument65 pages7-Eleven JapanInba ThamilanNo ratings yet
- Planting Plans For Your Kitchen Garden - How To Create A Vegetable, Herb and Fruit Garden in Easy Stages PDFDocument356 pagesPlanting Plans For Your Kitchen Garden - How To Create A Vegetable, Herb and Fruit Garden in Easy Stages PDFGiampaolo Pastorino100% (4)
- Cafe Market ResearchDocument9 pagesCafe Market ResearchRush YuviencoNo ratings yet
- Allergo-Immunology Hour: Food AllergyDocument32 pagesAllergo-Immunology Hour: Food AllergyJill PNo ratings yet
- Food Allergy Diagnosis and Management for PCPs Speaker GuideDocument58 pagesFood Allergy Diagnosis and Management for PCPs Speaker GuideEddy LiuNo ratings yet
- Malabsorption EnglishDocument46 pagesMalabsorption EnglishDragosAurNo ratings yet
- Coeliac Disease: DR Lei Lei WinDocument14 pagesCoeliac Disease: DR Lei Lei WinSivakumar Kathuu KarthikeyanNo ratings yet
- Eosinophillic Esophagitis-1Document29 pagesEosinophillic Esophagitis-1khan jeetNo ratings yet
- Food Allergy Vs Food Intolerance 1684503076Document33 pagesFood Allergy Vs Food Intolerance 1684503076Kevin AlexNo ratings yet
- Celiac DiseaseDocument35 pagesCeliac DiseaseRye HanaNo ratings yet
- Materi Dr. Nia OS IKA 117Document33 pagesMateri Dr. Nia OS IKA 117limgekun63No ratings yet
- Food Allergy in Childhood: Mja Practice Essentials - AllergyDocument7 pagesFood Allergy in Childhood: Mja Practice Essentials - AllergySarah Martinauli HarahapNo ratings yet
- Alergia Alimentos Manejo 2016Document17 pagesAlergia Alimentos Manejo 2016Tomàs Velarde DomínguezNo ratings yet
- Dieta Na Causa e No Manejo Do SII 2014Document11 pagesDieta Na Causa e No Manejo Do SII 2014Priscilla Ferreira Crespo GutierrezNo ratings yet
- Food Allergies (Salvat Automat)Document11 pagesFood Allergies (Salvat Automat)Dragu AndreeaNo ratings yet
- AllergyDocument7 pagesAllergyberlian29031992No ratings yet
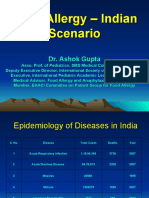
- Food Allergy - Indian ScenarioDocument28 pagesFood Allergy - Indian ScenarioAman BansalNo ratings yet
- NCM 116n Lecture Care of Clients With Problems in Gastrointestinal Function and NutritionDocument5 pagesNCM 116n Lecture Care of Clients With Problems in Gastrointestinal Function and NutritionKylle AlimosaNo ratings yet
- 10 1079@bjn2003872Document7 pages10 1079@bjn2003872skripsi kapNo ratings yet
- Dietary Treatment of Eosinophilic Esophagitis in Children: Treatment I: Current Therapeutic Options (The DDDS)Document6 pagesDietary Treatment of Eosinophilic Esophagitis in Children: Treatment I: Current Therapeutic Options (The DDDS)Haneen AljiffriNo ratings yet
- Celiac Disease Amar Araneta FinalDocument12 pagesCeliac Disease Amar Araneta FinalAlkiana SalardaNo ratings yet
- Gastrointestinal Manifestation of Food Allergy in Infants and ChildrenDocument44 pagesGastrointestinal Manifestation of Food Allergy in Infants and ChildrenSardono WidinugrohoNo ratings yet
- Malnut (Under Overnut)Document67 pagesMalnut (Under Overnut)ummu asiriNo ratings yet
- Fodmaps Presentation For WebsiteDocument20 pagesFodmaps Presentation For Websiteapi-338007586No ratings yet
- Celiac Desease: By: Leila Floresca Esteban BSNIII-BDocument38 pagesCeliac Desease: By: Leila Floresca Esteban BSNIII-BScarlet100% (1)
- The Gastrointestinal RADocument3 pagesThe Gastrointestinal RAAisha SaherNo ratings yet
- Original Communication: Food Habits in 10-11-Year-Old Children With Functional Gastrointestinal DisordersDocument6 pagesOriginal Communication: Food Habits in 10-11-Year-Old Children With Functional Gastrointestinal DisordersYuriko AndreNo ratings yet
- Chronic Abdominal Pain in ChildrenDocument3 pagesChronic Abdominal Pain in ChildrenOmar M AlsalmanNo ratings yet
- Biesiekierski 2011Document7 pagesBiesiekierski 2011Luiz PauloNo ratings yet
- Food Allergy in ChildrenDocument17 pagesFood Allergy in ChildrenvyasakandarpNo ratings yet
- Food AllergyDocument27 pagesFood AllergyAbabii GhenadieNo ratings yet
- Cows Milk Protein Allergy and Other Food Hypersensitivities in InfantsDocument9 pagesCows Milk Protein Allergy and Other Food Hypersensitivities in InfantsAzalia BahatNo ratings yet
- 470 CasestudyDocument8 pages470 Casestudyapi-241667785No ratings yet
- John Hopkins IbdDocument38 pagesJohn Hopkins IbdNovita ApramadhaNo ratings yet
- Nutricion Enteral en PediatriaDocument15 pagesNutricion Enteral en PediatriaFernanda Sanchez LozanoNo ratings yet
- The Fashionable Gluten-free Diet—Wear With CautionDocument2 pagesThe Fashionable Gluten-free Diet—Wear With CautionMita AriniNo ratings yet
- Celiac DiseaseDocument12 pagesCeliac DiseaseDasagrandhi Chakradhar100% (2)
- Overview of Biomedical Treatments PresentationDocument70 pagesOverview of Biomedical Treatments PresentationSimrat AnandNo ratings yet
- EditorialDocument2 pagesEditorialMuhammad FaizanNo ratings yet
- Ajol File Journals - 246 - Articles - 170174 - Submission - Proof - 170174 2929 437393 1 10 20180423Document6 pagesAjol File Journals - 246 - Articles - 170174 - Submission - Proof - 170174 2929 437393 1 10 20180423demiana shawkyNo ratings yet
- Rakel: Textbook of Family Medicine, 7th Ed.Document4 pagesRakel: Textbook of Family Medicine, 7th Ed.Nicolás Rojas MontenegroNo ratings yet
- Eating ProblemsDocument4 pagesEating ProblemsNicolás Rojas MontenegroNo ratings yet
- Eating ProblemsDocument4 pagesEating ProblemsximerodriguezcNo ratings yet
- Food Intolerance: WIKIPEDIA-2013 & Nelson 2004Document35 pagesFood Intolerance: WIKIPEDIA-2013 & Nelson 2004niaNo ratings yet
- C D /G I: Case ReportDocument3 pagesC D /G I: Case ReportCatalina Mariana MargarintNo ratings yet
- Clinical Management of Food AllergDocument16 pagesClinical Management of Food AllergChristian MartínezNo ratings yet
- The Gluten Free Generation-2Document7 pagesThe Gluten Free Generation-2api-254031084No ratings yet
- PIIS1542356522000349Document12 pagesPIIS1542356522000349AaNo ratings yet
- The Role of The Gastroenterologist in Non-Ige Mediated Gastrointestinal Food AllergyDocument6 pagesThe Role of The Gastroenterologist in Non-Ige Mediated Gastrointestinal Food AllergyIntan Robi'ahNo ratings yet
- Final Internship PresentationDocument25 pagesFinal Internship PresentationSaira JabeenNo ratings yet
- L23 Food IntolerancesDocument30 pagesL23 Food IntolerancesJason LouNo ratings yet
- Crohn's DiseaseDocument14 pagesCrohn's Diseasevenzmartinez100% (1)
- Case Study 1Document10 pagesCase Study 1api-242123281No ratings yet
- NutrigenomicsDocument26 pagesNutrigenomicsRia RamadhaniNo ratings yet
- Non-IgE-mediated Gastrointestinal Food AllergyDocument11 pagesNon-IgE-mediated Gastrointestinal Food AllergyJose Antonio VenacostaNo ratings yet
- Name Ambreen Fazal Roll No MS-HND-17-05 Submitted To Sir Tariq IsmailDocument16 pagesName Ambreen Fazal Roll No MS-HND-17-05 Submitted To Sir Tariq IsmailHAMMAD FAZALNo ratings yet
- Parrish July 2013Document7 pagesParrish July 2013Tada MinionNo ratings yet
- Hhs Public Access: Non-Ige Mediated Food Allergy SyndromesDocument7 pagesHhs Public Access: Non-Ige Mediated Food Allergy SyndromesIvan VeriswanNo ratings yet
- Alergia Alimentaria - Pediatr - Clin - NA 2011Document17 pagesAlergia Alimentaria - Pediatr - Clin - NA 2011Alvaro Retamal MatusNo ratings yet
- Approach To VomitingDocument16 pagesApproach To VomitingDenise Castro100% (1)
- Celiac DiseaseDocument55 pagesCeliac DiseasealctheyNo ratings yet
- Enteropatia EosinofilicaDocument6 pagesEnteropatia EosinofilicaLuisa Maria LagosNo ratings yet
- Diet Chart Bone FractureDocument2 pagesDiet Chart Bone FracturemanishNo ratings yet
- Trail Beaver Valley Edition of May 29, 2012 PennywiseDocument56 pagesTrail Beaver Valley Edition of May 29, 2012 PennywisePennywise PublishingNo ratings yet
- Tle BookletDocument12 pagesTle Bookletzionselegna012808No ratings yet
- Comparative Evaluation of Performance of Snails ArchachatinaDocument6 pagesComparative Evaluation of Performance of Snails ArchachatinaImpact JournalsNo ratings yet
- Keto Garlic Cheese Bread Recipe - Wholesome YumDocument1 pageKeto Garlic Cheese Bread Recipe - Wholesome YumMarcsy Joy VáryNo ratings yet
- Goosebumps Horrorland-Book 1Document114 pagesGoosebumps Horrorland-Book 1rumaisakamran811No ratings yet
- Kopano Letsaba: Personal InformationDocument2 pagesKopano Letsaba: Personal InformationmawandeNo ratings yet
- Home MedicineDocument29 pagesHome MedicineKristopher NealNo ratings yet
- WR Olstad 2012Document21 pagesWR Olstad 2012Ruxandra SimionNo ratings yet
- MotivationDocument2 pagesMotivationCedric Jake IlagNo ratings yet
- Health and Fitness Vocab (6799)Document2 pagesHealth and Fitness Vocab (6799)yoanaloNo ratings yet
- ... Thesis About Proper Hygiene Awareness Towards Food ProductionDocument25 pages... Thesis About Proper Hygiene Awareness Towards Food ProductionAngelie UmambacNo ratings yet
- Nestlé CASEDocument3 pagesNestlé CASEAli Iqbal CheemaNo ratings yet
- Live Pig MarketsDocument25 pagesLive Pig MarketsKoffee FarmerNo ratings yet
- Chapter 15.1 EcologyDocument18 pagesChapter 15.1 Ecologysriniketan dasNo ratings yet
- Retail Marketing Mix Case Study (LucidView)Document7 pagesRetail Marketing Mix Case Study (LucidView)shemanfuckhemanNo ratings yet
- DE: A: Gerencia Negocio Categoria Codigos Descripción OfertaDocument8 pagesDE: A: Gerencia Negocio Categoria Codigos Descripción OfertaGuadalupe Guerrero JimenezNo ratings yet
- LEARNING TASK 1:read The Statement Carefully and Choose The Answer That Best Describes The StatementDocument2 pagesLEARNING TASK 1:read The Statement Carefully and Choose The Answer That Best Describes The StatementMa'am EdilynNo ratings yet
- Pricelist 2019Document106 pagesPricelist 2019Riezka SicwekEembemm CuabhiabiezzNo ratings yet
- Modul TOEFL Final Simulasi Toefl UjianDocument78 pagesModul TOEFL Final Simulasi Toefl UjianAxthaNo ratings yet
- PPAE - Siklus 2 - Eksplorasi Konsep - Rakhmadhona IDocument2 pagesPPAE - Siklus 2 - Eksplorasi Konsep - Rakhmadhona IDona FarahNo ratings yet
- 2as Files'Document105 pages2as Files'Śŋŏw Wĥíțě86% (79)
- Operations Research II An Assignment Submitted By: Submitted To: Prof. GonzalesDocument3 pagesOperations Research II An Assignment Submitted By: Submitted To: Prof. GonzalesAbegail LiguanNo ratings yet