Download as pdf or txt
You might also like
- Great Writing 4 5th Edition Great Essays Answer KeyDocument10 pagesGreat Writing 4 5th Edition Great Essays Answer KeyAseel80% (10)
- Assignment #4 Supported Student Self-Assessment (Antonia2)Document32 pagesAssignment #4 Supported Student Self-Assessment (Antonia2)SapMars 0No ratings yet
- When To Pick The Nose: Out-of-Hospital and Emergency Department Intranasal Administration of MedicationsDocument9 pagesWhen To Pick The Nose: Out-of-Hospital and Emergency Department Intranasal Administration of MedicationsepraetorianNo ratings yet
- In Cold Blood - WordDocument8 pagesIn Cold Blood - WordSalomeea Nicoleta0% (1)
- NEWHOUSE 1999 - Asthma Therapy With AerosolsDocument4 pagesNEWHOUSE 1999 - Asthma Therapy With AerosolsRafael JustinoNo ratings yet
- Kontrak Belajar Gadar Igd BaruDocument14 pagesKontrak Belajar Gadar Igd BaruAstridNo ratings yet
- PILLOW 2012 - Innovation in Surfactant Therapy II-surfactant Administration by Aerosolization.Document8 pagesPILLOW 2012 - Innovation in Surfactant Therapy II-surfactant Administration by Aerosolization.Rafael JustinoNo ratings yet
- Fmed 09 920549Document8 pagesFmed 09 920549Fernando DornelNo ratings yet
- Gibbs2020 2Document14 pagesGibbs2020 2Dan ZhouNo ratings yet
- Nebulizer ProquestDocument10 pagesNebulizer ProquestFadhli WijayaNo ratings yet
- Immediate Effects and Safety of High-Frequency Chest Wall Compression Compared To Airway Clearance Techniques in Non-Hospitalized Infants With Acute Viral BronchiolitisDocument9 pagesImmediate Effects and Safety of High-Frequency Chest Wall Compression Compared To Airway Clearance Techniques in Non-Hospitalized Infants With Acute Viral BronchiolitisBelén María Vega AladueñaNo ratings yet
- Management of Rare Causes of Pediatric Chronic Respiratory FailureDocument16 pagesManagement of Rare Causes of Pediatric Chronic Respiratory FailureISABEL SOFIA CABARCAS COGOLLONo ratings yet
- Lauder 2019Document12 pagesLauder 2019Julio AltamiranoNo ratings yet
- Conti 2016Document7 pagesConti 2016Dwi Putri SekariniNo ratings yet
- Spacers Vs Nebulizers in Children With Acute AsthmaDocument3 pagesSpacers Vs Nebulizers in Children With Acute AsthmaRichard ChandraNo ratings yet
- Neonatal Noninvasive Ventilation Techniques: Do We Really Need To Intubate?Document25 pagesNeonatal Noninvasive Ventilation Techniques: Do We Really Need To Intubate?sing terriblyNo ratings yet
- New Developments in Neonatal Respiratory MenagmentDocument7 pagesNew Developments in Neonatal Respiratory MenagmentTin TomašićNo ratings yet
- How To Choose Delivery Devices For Asthma: Leading ArticlesDocument3 pagesHow To Choose Delivery Devices For Asthma: Leading ArticlescryptoNo ratings yet
- Original Contributions: A Randomized Trial Comparing Metered Dose Inhalers and Breath Actuated NebulizersDocument8 pagesOriginal Contributions: A Randomized Trial Comparing Metered Dose Inhalers and Breath Actuated NebulizersDesmiyati AdoeNo ratings yet
- 793 FullDocument8 pages793 FullDaniele PeixotoNo ratings yet
- Research Proposal PaperDocument16 pagesResearch Proposal Paperapi-3124667550% (1)
- Schor Home Made Spacers For Asthma Prgmatic Trial Resp Med 2017Document7 pagesSchor Home Made Spacers For Asthma Prgmatic Trial Resp Med 2017andydossousNo ratings yet
- Neoreviews 2013 Keszler E237 51Document17 pagesNeoreviews 2013 Keszler E237 51Gun HawkNo ratings yet
- Clinical Controversies in Aerosol Therapy For Infants and ChildrenDocument23 pagesClinical Controversies in Aerosol Therapy For Infants and Childrencelma44No ratings yet
- Short-Acting Sedative-Analgesic Drugs Protect Against Development of Ventilator-Associated Events in Children: Secondary Analysis of The EUVAE StudyDocument8 pagesShort-Acting Sedative-Analgesic Drugs Protect Against Development of Ventilator-Associated Events in Children: Secondary Analysis of The EUVAE StudyevyNo ratings yet
- 693 FullDocument12 pages693 FullGilmer alvarez floresNo ratings yet
- FasdfyDocument8 pagesFasdfyzuliamNo ratings yet
- 1fca PDFDocument13 pages1fca PDFHalim SudonoNo ratings yet
- Comparison of Clinical Outcomes Following DeliveryDocument7 pagesComparison of Clinical Outcomes Following DeliveryRamya DivyaNo ratings yet
- Respiratory Support For Adult Patients With COVID-19Document7 pagesRespiratory Support For Adult Patients With COVID-19SekarNo ratings yet
- Acfrogau Hl2os57rysppmfbuxnkyces7slcfmgih4ufokbsvcws67id O04q8tu Qom5nztkzxybibeoqx1rbctam3lz6rd-0txb7-Brq9tgd0n9rtdfs Nzyjzjyuxqlvkcyhnywmulzu-MnkrDocument6 pagesAcfrogau Hl2os57rysppmfbuxnkyces7slcfmgih4ufokbsvcws67id O04q8tu Qom5nztkzxybibeoqx1rbctam3lz6rd-0txb7-Brq9tgd0n9rtdfs Nzyjzjyuxqlvkcyhnywmulzu-MnkrHugo LopezNo ratings yet
- Promoting NIV Using ICEMAN Methodology: Qatar Critical Care Conference AbstractDocument3 pagesPromoting NIV Using ICEMAN Methodology: Qatar Critical Care Conference AbstractMarselya GaniNo ratings yet
- Future Options For Aerosol Delivery To Children: Allergy February 1999Document8 pagesFuture Options For Aerosol Delivery To Children: Allergy February 1999Suada HalimiNo ratings yet
- Mccambridge 2017Document13 pagesMccambridge 2017Ana ValladaresNo ratings yet
- Saans - Efficacy of Multi-Powered Continuous Positive Airway Pressure DeviceDocument6 pagesSaans - Efficacy of Multi-Powered Continuous Positive Airway Pressure Deviceemailtrinaya30No ratings yet
- Pediatric Anesthesia - 2022 - Weatherall - Developing An Extubation Strategy For The Difficult Pediatric Airway Who WhenDocument8 pagesPediatric Anesthesia - 2022 - Weatherall - Developing An Extubation Strategy For The Difficult Pediatric Airway Who WhenPamela Mamani FloresNo ratings yet
- Wright Et Al 2022 PDFDocument9 pagesWright Et Al 2022 PDFRadu CiprianNo ratings yet
- Equipment Evaluation ReportDocument6 pagesEquipment Evaluation ReportemotionkuNo ratings yet
- Anti-In Ammatory Reliever Therapy in Asthma: The Evidence Mounts But More Is NeededDocument3 pagesAnti-In Ammatory Reliever Therapy in Asthma: The Evidence Mounts But More Is NeededHanavi NathanielNo ratings yet
- Pi Is 2213219820313970Document4 pagesPi Is 2213219820313970cuvinhNo ratings yet
- CEP Modified High-Flow Nasal Cannula For Children With Respiratory DistressDocument6 pagesCEP Modified High-Flow Nasal Cannula For Children With Respiratory DistressLisa MaghfirahNo ratings yet
- Aerosol Delivery 2012 PDFDocument14 pagesAerosol Delivery 2012 PDFyoyo15No ratings yet
- Intjprevmed6133-2704195 004504Document6 pagesIntjprevmed6133-2704195 004504Ade HabibieNo ratings yet
- 2021 EMR High-Flow Nasal Cannula Oxygen TherapyDocument14 pages2021 EMR High-Flow Nasal Cannula Oxygen TherapyRenzoFcoLavanLopezNo ratings yet
- ASMA en ER Revision 2020Document10 pagesASMA en ER Revision 2020Marcos Chusin MontesdeocaNo ratings yet
- Face Mask Ventilation in Edentulous Patients: A Comparison of Mandibular Groove and Lower Lip PlacementDocument4 pagesFace Mask Ventilation in Edentulous Patients: A Comparison of Mandibular Groove and Lower Lip PlacementLinda Wahyu UtamiiNo ratings yet
- Difficult or Impossible Facemask Ventilation in Children With DifficultDocument10 pagesDifficult or Impossible Facemask Ventilation in Children With Difficultema moralesNo ratings yet
- Improving Care of Patients On Non Invasive Ventilation (NIV) in The General WardsDocument7 pagesImproving Care of Patients On Non Invasive Ventilation (NIV) in The General WardsrefanNo ratings yet
- Homework 2 (1) FinalDocument3 pagesHomework 2 (1) FinalJosphat MuturiNo ratings yet
- BudesonidDocument5 pagesBudesonidparamita nindyaNo ratings yet
- TI Croup Review Macdonald 1997Document3 pagesTI Croup Review Macdonald 1997mutimutimutiNo ratings yet
- Practices Using Nebuliser at HomeDocument10 pagesPractices Using Nebuliser at HomeuyaainiNo ratings yet
- 07.04.05 Venturi Face MaskDocument2 pages07.04.05 Venturi Face MaskInzamam Ul HaqNo ratings yet
- 589-Article Text-1298-1-10-20220830 PDFDocument12 pages589-Article Text-1298-1-10-20220830 PDFBella FebriantiNo ratings yet
- Acute Asthma ManagementDocument3 pagesAcute Asthma ManagementmjeanjNo ratings yet
- Sedation in BronchosDocument13 pagesSedation in BronchosEfrainNo ratings yet
- Nebulized Versus MDI Medication Administration in COVID-19 PatientsDocument3 pagesNebulized Versus MDI Medication Administration in COVID-19 Patientssalman683 gNo ratings yet
- Comment: Lancet Respir Med 2017Document2 pagesComment: Lancet Respir Med 2017Novy DitaNo ratings yet
- Post Extubation Stridor UHL Paediatric Intensive Care GuidelineDocument6 pagesPost Extubation Stridor UHL Paediatric Intensive Care Guidelineandreea.spasenieNo ratings yet
- Ppa 7 027 PDFDocument9 pagesPpa 7 027 PDFbellaNo ratings yet
- Oral Dexamethasone For Bronchiolitis A Randomized TrialDocument9 pagesOral Dexamethasone For Bronchiolitis A Randomized TrialhwelpNo ratings yet
- Antibiotics Inhalados en NavmDocument10 pagesAntibiotics Inhalados en NavmAnthony Huaman MedinaNo ratings yet
- MIEDEMA 2013 - Effect of Nasal Continuous and Biphasic Positive Airway Pressure On Lung Volume in Preterm InfantsDocument7 pagesMIEDEMA 2013 - Effect of Nasal Continuous and Biphasic Positive Airway Pressure On Lung Volume in Preterm InfantsRafael JustinoNo ratings yet
- ORENSTEIN 2002 - Cystic Fibrosis - A 2002 UpdateDocument9 pagesORENSTEIN 2002 - Cystic Fibrosis - A 2002 UpdateRafael JustinoNo ratings yet
- POLIN 2009 - Bubble CPAP - A Clash of Science Culture and ReligionDocument2 pagesPOLIN 2009 - Bubble CPAP - A Clash of Science Culture and ReligionRafael JustinoNo ratings yet
- GUPTA 2009 - A RCT of Post Extubation BCPAP Versus Infant Flow Driver CPAP in Preterm Infants With RDSDocument8 pagesGUPTA 2009 - A RCT of Post Extubation BCPAP Versus Infant Flow Driver CPAP in Preterm Infants With RDSRafael JustinoNo ratings yet
- ABIGAIL 2010 - Diffuse Alveolar HemorrhageDocument10 pagesABIGAIL 2010 - Diffuse Alveolar HemorrhageRafael JustinoNo ratings yet
- NARASIMHAN - Pulmonary Haemorrhage in NeonatesDocument3 pagesNARASIMHAN - Pulmonary Haemorrhage in NeonatesRafael JustinoNo ratings yet
- NEWHOUSE 1999 - Asthma Therapy With AerosolsDocument4 pagesNEWHOUSE 1999 - Asthma Therapy With AerosolsRafael JustinoNo ratings yet
- BURG 2014 - Cross-Sectional Changes in Lung Volume Measured by Electrical Impedance Tomography Are Representative For The Whole Lung in Ventilated Preterm InfantsDocument8 pagesBURG 2014 - Cross-Sectional Changes in Lung Volume Measured by Electrical Impedance Tomography Are Representative For The Whole Lung in Ventilated Preterm InfantsRafael JustinoNo ratings yet
- HOUGH 2014 - Lung Recruitment and Endotracheal Suction in Ventilated Preterm Infants Measured With Electrical Impedance TomographyDocument7 pagesHOUGH 2014 - Lung Recruitment and Endotracheal Suction in Ventilated Preterm Infants Measured With Electrical Impedance TomographyRafael JustinoNo ratings yet
- ALVIRA 2017 - Can We Understand The Pathobiology of Bronchopulmonary DysplasiaDocument11 pagesALVIRA 2017 - Can We Understand The Pathobiology of Bronchopulmonary DysplasiaRafael JustinoNo ratings yet
- BURG 2016 - Effect of Minimally Invasive Surfactant Therapy On Lung Volume and Ventilation in Preterm InfantsDocument6 pagesBURG 2016 - Effect of Minimally Invasive Surfactant Therapy On Lung Volume and Ventilation in Preterm InfantsRafael JustinoNo ratings yet
- BIBAN 2012 - Exogenous Surfactant Replacement - How To Deliver ItDocument6 pagesBIBAN 2012 - Exogenous Surfactant Replacement - How To Deliver ItRafael JustinoNo ratings yet
- ISAYAMA 2017 - Revisiting The Definition of Bronchopulmonary DysplasiaDocument9 pagesISAYAMA 2017 - Revisiting The Definition of Bronchopulmonary DysplasiaRafael JustinoNo ratings yet
- MIEDEMA 2011 - Changes in Lung Volume and Ventilation During Surfactant Treatment in Ventilated Preterm InfantsDocument6 pagesMIEDEMA 2011 - Changes in Lung Volume and Ventilation During Surfactant Treatment in Ventilated Preterm InfantsRafael JustinoNo ratings yet
- Neuroprotective MgSO4Document6 pagesNeuroprotective MgSO4Rafael JustinoNo ratings yet
- SOLALIGUE 2017 - 1 Recent Advances in Our Understanding of The Mechanisms of Late Lunf Development and BPDDocument190 pagesSOLALIGUE 2017 - 1 Recent Advances in Our Understanding of The Mechanisms of Late Lunf Development and BPDRafael JustinoNo ratings yet
- LISTA 2012 - Surfactant and Mechanical VentilationDocument3 pagesLISTA 2012 - Surfactant and Mechanical VentilationRafael JustinoNo ratings yet
- Ultrasound in Obstet Gyne - 2002 - Laudy - The Fetal Lung 1 Developmental AspectsDocument7 pagesUltrasound in Obstet Gyne - 2002 - Laudy - The Fetal Lung 1 Developmental AspectsRafael JustinoNo ratings yet
- Annex 35 Guidelines of IPC and Clinical MX of SARI and PNEUMONIA TRO COVID19 3.11.2020Document4 pagesAnnex 35 Guidelines of IPC and Clinical MX of SARI and PNEUMONIA TRO COVID19 3.11.2020Yeoh Zi-NingNo ratings yet
- Assessment of S.Y. 2021-2022 Curriculum (Most Essential Learning Competencies)Document5 pagesAssessment of S.Y. 2021-2022 Curriculum (Most Essential Learning Competencies)Mary Kryss DG SangleNo ratings yet
- QN - Arsenio - Relationship Between Family Structure and The Level ofDocument36 pagesQN - Arsenio - Relationship Between Family Structure and The Level ofSir JrNo ratings yet
- NBK QN BB 2022Document6 pagesNBK QN BB 2022Ngọc DiệpNo ratings yet
- PR Number Description Status Received Date Sof ABC Po Amnt Supplier/Contractor Assignees MOPDocument11 pagesPR Number Description Status Received Date Sof ABC Po Amnt Supplier/Contractor Assignees MOPLito GarinNo ratings yet
- Review On Inflammatory DisesesDocument21 pagesReview On Inflammatory Disesesdigitalmazdoor5201No ratings yet
- Solid Waste Management: M. Sc. Environmental Science Central University of RajasthanDocument21 pagesSolid Waste Management: M. Sc. Environmental Science Central University of RajasthanAvrenim Magaro DecanoNo ratings yet
- EDU 404 Course OutlineDocument3 pagesEDU 404 Course OutlineMoses Akano OluwaseunNo ratings yet
- Sun Cobalt 8 % MsdsDocument3 pagesSun Cobalt 8 % MsdskunalNo ratings yet
- 1842 13404 1 SMDocument7 pages1842 13404 1 SMnanda wildaNo ratings yet
- Dentistry 10 00222Document18 pagesDentistry 10 00222kittyNo ratings yet
- Bachelor of Hospital ManagementDocument5 pagesBachelor of Hospital ManagementsurajyellowkiteNo ratings yet
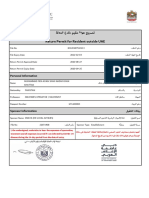
- Return Permit For Resident Outside UAEDocument3 pagesReturn Permit For Resident Outside UAEᘉᓋᘻᗗᘙ ᘉᓋᙏᓲ ᖽᐸᗁᕠᘘNo ratings yet
- Yoga Asana - Pawanmuktasana For Gas ProblemDocument2 pagesYoga Asana - Pawanmuktasana For Gas ProblemMIBNo ratings yet
- Cardiopulmonary Resuscitation For Adults Pedia and InfantsDocument35 pagesCardiopulmonary Resuscitation For Adults Pedia and InfantsAnna Carmela Pillora MelendezNo ratings yet
- Argumentative EssayDocument2 pagesArgumentative EssayIbn KathirNo ratings yet
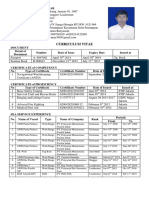
- CV Anwar - LeadermanDocument1 pageCV Anwar - LeadermanAsep Rahmat YuliantoNo ratings yet
- 7 - SDS-Gypsum-1Document1 page7 - SDS-Gypsum-1Bashar Al AliNo ratings yet
- 20 Đề Thi Thử Tốt Nghiệp Thpt Năm 2021 Môn Tiếng Anh Bám Sát Và Phát Triển Đề Minh Họa Của Bộ Gd&Đt Có Đáp ÁnDocument161 pages20 Đề Thi Thử Tốt Nghiệp Thpt Năm 2021 Môn Tiếng Anh Bám Sát Và Phát Triển Đề Minh Họa Của Bộ Gd&Đt Có Đáp ÁnNgọc HuyềnNo ratings yet
- Spatial Infant MDocument9 pagesSpatial Infant MBezan MeleseNo ratings yet
- Communication Skills: Nazia AliDocument38 pagesCommunication Skills: Nazia AliNida MughalNo ratings yet
- (Template) DVTDocument21 pages(Template) DVTPema Lamu TdkNo ratings yet
- Ethical Case StudiesDocument9 pagesEthical Case StudiesًNo ratings yet
- EENC (Early Essential Newborn Care) BREATHING BABY. Preparation Stage Not Done Partially Done Done 0 1 2Document2 pagesEENC (Early Essential Newborn Care) BREATHING BABY. Preparation Stage Not Done Partially Done Done 0 1 2Trevor UratelNo ratings yet
- NHS FPX 5004 Assessment 3 Diversity Project Kickoff PresentationDocument5 pagesNHS FPX 5004 Assessment 3 Diversity Project Kickoff Presentationfarwaamjad771No ratings yet
- Moving Meditation of SilambamDocument4 pagesMoving Meditation of SilambamGabrielNo ratings yet
- Case Study: "Burn Injury"Document24 pagesCase Study: "Burn Injury"ChAtmaRosE100% (1)