Download as pdf or txt
You might also like
- Pay OnlineDocument2 pagesPay Online30dgalleNo ratings yet
- STAI 6item Scoring BekkerDocument2 pagesSTAI 6item Scoring BekkerJasleen Kaur100% (1)
- Patient Admission FormDocument2 pagesPatient Admission Formelmore kakaNo ratings yet
- Referral Control Sheet For Out Patient Consultation (RCS 1)Document3 pagesReferral Control Sheet For Out Patient Consultation (RCS 1)larie4mae4montefalcoNo ratings yet
- Claim Form GeneralDocument1 pageClaim Form GeneralTanya Rose-AppleNo ratings yet
- CPG-3rd Trimester Bleeding and Postpartum Hemorrage 2009Document107 pagesCPG-3rd Trimester Bleeding and Postpartum Hemorrage 2009lovelots1234100% (9)
- Wmedd Ein2030Document2 pagesWmedd Ein2030Chad WatsonNo ratings yet
- Bupa Global Claim Form: 1 Patient'S DetailsDocument4 pagesBupa Global Claim Form: 1 Patient'S Details123owenNo ratings yet
- Family Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsDocument2 pagesFamily Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsnomiabbasiNo ratings yet
- Tweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisDocument56 pagesTweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisAnonymous 1uVifBp6100% (1)
- Survival Probabilities - Kaplan Meier MethodDocument2 pagesSurvival Probabilities - Kaplan Meier MethodLakshmi Seth100% (1)
- Nursing AssessmentDocument10 pagesNursing AssessmentWaldrich KhanNo ratings yet
- Banguis-Romeo-A - 5 11 2024Document1 pageBanguis-Romeo-A - 5 11 2024reggie tiongsonNo ratings yet
- JFR Claim Form Leonardo PreenchidoDocument3 pagesJFR Claim Form Leonardo PreenchidoNatália André RodriguesNo ratings yet
- ApprovalDocument3 pagesApprovalabelswife87No ratings yet
- OSHC - Claims FormDocument3 pagesOSHC - Claims FormMr AkashNo ratings yet
- Referral Control Sheet For Out Patient Consultation (RCS 1)Document3 pagesReferral Control Sheet For Out Patient Consultation (RCS 1)larie4mae4montefalcoNo ratings yet
- Ercs 2Document4 pagesErcs 2Alexandre Nicole SecuyaNo ratings yet
- RSPCA Vet Fee Claim Form SecuredDocument2 pagesRSPCA Vet Fee Claim Form SecuredMihaela LetNo ratings yet
- Arcega Arnel S. 3 15 24. RevisedDocument1 pageArcega Arnel S. 3 15 24. RevisedMark BaniagaNo ratings yet
- Arcega Florence Diane R. 3 15 24. RevisedDocument1 pageArcega Florence Diane R. 3 15 24. RevisedMark BaniagaNo ratings yet
- Arcega Maria Lucia R. 3 15 24 RevisedDocument1 pageArcega Maria Lucia R. 3 15 24 RevisedMark BaniagaNo ratings yet
- Medical Services Division: Hi-Precision Diagnostics (V Luna Branch)Document1 pageMedical Services Division: Hi-Precision Diagnostics (V Luna Branch)Ren RenNo ratings yet
- Referral Control Sheet For Out-Patient Consultation (RCS 1) : Valid UntilDocument2 pagesReferral Control Sheet For Out-Patient Consultation (RCS 1) : Valid UntilClaire Melody CalumpangNo ratings yet
- Pasco, Roxanne Gean P - 6Document2 pagesPasco, Roxanne Gean P - 6Rens KSNo ratings yet
- 07BF1426 2 Original PDFDocument4 pages07BF1426 2 Original PDFAnonymous 2R8gZ9No ratings yet
- Medicare Care PolicyDocument6 pagesMedicare Care PolicyLeti StarNo ratings yet
- Japitana-Ricky 240313 115210Document2 pagesJapitana-Ricky 240313 115210Ariel CaparroNo ratings yet
- 20210308-0043-B Lur No.: Laboratory / Radiology / Ultrasound Request FormDocument1 page20210308-0043-B Lur No.: Laboratory / Radiology / Ultrasound Request FormMarvin VerdadNo ratings yet
- Generate LOADocument1 pageGenerate LOAangel.domingo0309No ratings yet
- Op - Zapanta, Annabelle PDFDocument2 pagesOp - Zapanta, Annabelle PDFWendylNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceHemantNo ratings yet
- Application For New CGHS CardDocument3 pagesApplication For New CGHS CardGautham PrasadNo ratings yet
- Cisi Id Heloisa de Melo Rabelo 2605566Document1 pageCisi Id Heloisa de Melo Rabelo 2605566Heloisa RabeloNo ratings yet
- 3 PDFDocument6 pages3 PDFJamie HurstNo ratings yet
- 20220514-0117-C CF No.: Bdo Unibank, Inc. 12/31/2022Document1 page20220514-0117-C CF No.: Bdo Unibank, Inc. 12/31/2022Faitheey EscalanteNo ratings yet
- UMESH MS OFFIC CorrectionDocument2 pagesUMESH MS OFFIC Correctionrajput sanjeevNo ratings yet
- Imprimeeeeee PDFDocument52 pagesImprimeeeeee PDFKarina BarrientosNo ratings yet
- Reimbursement Request CUAETDocument1 pageReimbursement Request CUAETqwertNo ratings yet
- Laporan Kegiatan Dan Reimbursement Biaya Pengurusan Visa AustraliaDocument5 pagesLaporan Kegiatan Dan Reimbursement Biaya Pengurusan Visa AustraliamemekbecekNo ratings yet
- Return Shipment Form 111470 GASTRO SUCREDocument2 pagesReturn Shipment Form 111470 GASTRO SUCREAndrea OrtizNo ratings yet
- Philippine Charity Sweepstakes OfficeDocument1 pagePhilippine Charity Sweepstakes OfficeRandy Ramos FloresNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceTEJA SINGHNo ratings yet
- Generate 1Document6 pagesGenerate 1angeloaiden08No ratings yet
- Aubrellian Sofia A. AcedoDocument5 pagesAubrellian Sofia A. AcedoMedical Records Manango HospitalNo ratings yet
- Submitted Under The Procedures of The Employment Dispute Resolution Plan For The United States Court of Appeals For The Ninth CircuitDocument110 pagesSubmitted Under The Procedures of The Employment Dispute Resolution Plan For The United States Court of Appeals For The Ninth CircuitEquality Case FilesNo ratings yet
- HI Transfer CertificateDocument1 pageHI Transfer CertificatethoaionlineNo ratings yet
- f10 Claim FormDocument2 pagesf10 Claim Formiceslurpie100% (1)
- Bli - Mat.form. SampleDocument2 pagesBli - Mat.form. SamplebalatejenalynNo ratings yet
- Cadence InternationalDocument2 pagesCadence Internationalminhdang03062017No ratings yet
- Vpi FormDocument2 pagesVpi FormPadma AnneNo ratings yet
- Paramount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceDocument2 pagesParamount Health Services & Insurance Tpa Private Limited: Deficiency Letter Without PrejudiceHiren PanchalNo ratings yet
- Personal Details: XXXX-XXXXDocument4 pagesPersonal Details: XXXX-XXXXSaikat SarkarNo ratings yet
- Medical Declaration Form - Less Than 50 - EnglishDocument1 pageMedical Declaration Form - Less Than 50 - EnglishMohammed GeoffreyNo ratings yet
- Re: Your Medical Card Review - : Reference Number 5361176Document7 pagesRe: Your Medical Card Review - : Reference Number 5361176Cristian NistorNo ratings yet
- CGHS ApplcaDocument5 pagesCGHS ApplcavvalliraoNo ratings yet
- Dental Care Claim Form 2010Document2 pagesDental Care Claim Form 2010Mehdi AlhaddadNo ratings yet
- Kaiser Permanente Sample BillDocument4 pagesKaiser Permanente Sample BillCandy Valentine0% (1)
- Claim FormDocument4 pagesClaim Formmuhammad haroonNo ratings yet
- Letter of Authorization (LOA) : DIAGNOSTIC/ Procedure Approval FormDocument1 pageLetter of Authorization (LOA) : DIAGNOSTIC/ Procedure Approval FormLevelyn de GranoNo ratings yet
- De Leon, Charmagne BDocument1 pageDe Leon, Charmagne BHasmin CortezNo ratings yet
- Uiopwaiver 263Document5 pagesUiopwaiver 263mike_mckeown_3No ratings yet
- REQUISISTOS CERTIFICADOS MEDICOS POR COVID-signed-signed-signedDocument4 pagesREQUISISTOS CERTIFICADOS MEDICOS POR COVID-signed-signed-signedMarco DávilaNo ratings yet
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
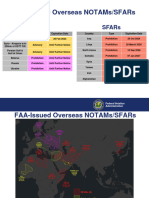
- FAA - NOTAM and SFAR - Summary - 11 December 2023Document5 pagesFAA - NOTAM and SFAR - Summary - 11 December 2023Diego PauloNo ratings yet
- Notams LLBGDocument2 pagesNotams LLBGDiego PauloNo ratings yet
- BK 150 Emergency Response Guidance 2023-2024Document107 pagesBK 150 Emergency Response Guidance 2023-2024Diego PauloNo ratings yet
- 1.1. ATIS 1.2. Speed Restrictions 11.. Ggeenneerraall: 1.3.1. RWY USAGEDocument52 pages1.1. ATIS 1.2. Speed Restrictions 11.. Ggeenneerraall: 1.3.1. RWY USAGEDiego PauloNo ratings yet
- 1.1. ATIS 1.2. Rwy Operations 11.. Ggeenneerraall: 1.2.1. Preferential Rwy System 1.2.2. RWY USAGEDocument30 pages1.1. ATIS 1.2. Rwy Operations 11.. Ggeenneerraall: 1.2.1. Preferential Rwy System 1.2.2. RWY USAGEDiego PauloNo ratings yet
- Milford Track InfoDocument8 pagesMilford Track InfoDiego PauloNo ratings yet
- What Is Deja Vu PresentationDocument8 pagesWhat Is Deja Vu PresentationSeskiara VivekaNo ratings yet
- Alcohol Treatment CenterDocument54 pagesAlcohol Treatment CenterAnonymous ntDYikdyNo ratings yet
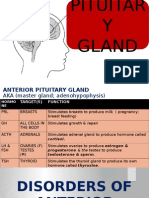
- Disorders of Pituitary GlandDocument34 pagesDisorders of Pituitary GlandninaaltheaNo ratings yet
- Module 3Document3 pagesModule 3Angie MandeoyaNo ratings yet
- Dharma Patel Resume 1Document1 pageDharma Patel Resume 1api-474249179No ratings yet
- Syllabus DraftDocument7 pagesSyllabus Draftapi-440514424No ratings yet
- Ate GlendaDocument3 pagesAte GlendaRomel Ricafort John DavidNo ratings yet
- Tepid SpongebobDocument2 pagesTepid SpongebobSean Rene Duay100% (2)
- ASSESSMENT OF EYE and EARDocument7 pagesASSESSMENT OF EYE and EARJae TyNo ratings yet
- Urinalysis Lab Conclusion: Exemplar DataDocument3 pagesUrinalysis Lab Conclusion: Exemplar Dataapi-397103674No ratings yet
- Spesifikasi CT Scan Somatom Perspective 128 SliceDocument2 pagesSpesifikasi CT Scan Somatom Perspective 128 SliceVro JackNo ratings yet
- 118 RLE Suction PDFDocument4 pages118 RLE Suction PDFclaire yowsNo ratings yet
- Hospital Bed Carena enDocument12 pagesHospital Bed Carena enj pandeyNo ratings yet
- CPD For Nurses Udp081010Document27 pagesCPD For Nurses Udp081010AzlizawatiBintiAzisAtieNo ratings yet
- Case Presentation Bipolar 1 Manic TypeDocument18 pagesCase Presentation Bipolar 1 Manic Typenailed_heart0% (1)
- Sedatives (Anxiolytic Minor Tranquilizers) and HypnoticsDocument26 pagesSedatives (Anxiolytic Minor Tranquilizers) and Hypnotics林益廷No ratings yet
- Is Our Brain Really Necessary-LorberDocument3 pagesIs Our Brain Really Necessary-Lorberbigjon1359100% (1)
- For Shall Of: If IsDocument5 pagesFor Shall Of: If IsMark ElbenNo ratings yet
- Artículo Terapia EsquemasDocument24 pagesArtículo Terapia EsquemasAna Salvador CastellanoNo ratings yet
- Models of Health and Health PromotionDocument16 pagesModels of Health and Health Promotionapi-31127039450% (2)
- Daftar PustakaDocument2 pagesDaftar PustakajacksonmpNo ratings yet
- Hemorrhagic Disease of NewbornDocument29 pagesHemorrhagic Disease of NewbornLittleThingsInside100% (1)
- Making A DiagnosisDocument6 pagesMaking A DiagnosisAndreea AndraNo ratings yet
- NRSG 428lDocument4 pagesNRSG 428lapi-2778422060% (1)
- Database - Management - System - Case - Studies Hospital1Document3 pagesDatabase - Management - System - Case - Studies Hospital1ceupritNo ratings yet