
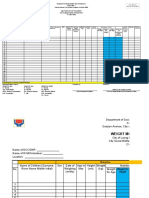
Weight Monitoring Report
Weight Monitoring Report
You might also like
- SAMPLE BNAP 2023 2025 - Template 1Document45 pagesSAMPLE BNAP 2023 2025 - Template 1Maryde Ompoy100% (7)
- Masterlist of ChildrenDocument8 pagesMasterlist of ChildrenJoena Balicao0% (1)
- SFP Masterlist, CNS Forms For LGUs NewDocument4 pagesSFP Masterlist, CNS Forms For LGUs NewJohny F. Villanueva0% (1)
- Fenton Growth Chart Girl v1Document2 pagesFenton Growth Chart Girl v1Hamba Allah75% (4)
- Fenton Growth Chart Boy v1Document2 pagesFenton Growth Chart Boy v1nurhapsari20100% (3)
- Seqota Declaration PresentationDocument17 pagesSeqota Declaration Presentationsimeneh100% (1)
- Crec Masterlist Format V7Document41 pagesCrec Masterlist Format V7John Dalton Marin VelascoNo ratings yet
- Nutritional AssessmentDocument49 pagesNutritional AssessmentIrene Grace Balcueva100% (1)
- Weight Monitoring FormDocument1 pageWeight Monitoring FormChristopher Torres50% (2)
- SFP Revised MasterlistDocument4 pagesSFP Revised MasterlistAaron Dan GlerNo ratings yet
- Nutritional Status Male Female: Nutritional Status: (Using CGS As Reference) OPT-Operation TimbangDocument6 pagesNutritional Status Male Female: Nutritional Status: (Using CGS As Reference) OPT-Operation TimbangBun AhNo ratings yet
- Enhanced CDC NS Monitoring Form Masterlist of Beneficiaries and LGU Consolidation of NS ReportDocument4 pagesEnhanced CDC NS Monitoring Form Masterlist of Beneficiaries and LGU Consolidation of NS ReportluffyNo ratings yet
- Inbound 8077990623609746721Document1 pageInbound 8077990623609746721Careh Maralit AboaboNo ratings yet
- After 120 Forms 1Document4 pagesAfter 120 Forms 1Kenneth Jean EblamoNo ratings yet
- Weight Monitoring Tool NEW For CDWDocument2 pagesWeight Monitoring Tool NEW For CDWronnie zurbitoNo ratings yet
- SF Monitorinf Form After MonthsDocument4 pagesSF Monitorinf Form After MonthsTina TalyodNo ratings yet
- DSWD FeedingDocument2 pagesDSWD FeedingNikko Rey MainitNo ratings yet
- SubredditDocument2 pagesSubredditregine abayonNo ratings yet
- BNS Form No.2Document1 pageBNS Form No.2qw8s5sb9crNo ratings yet
- Pob East Masterlist 2023Document35 pagesPob East Masterlist 2023Sylvia N. CantoriaNo ratings yet
- Barangay Health Worker Barangay Nutrition Scholar Full Weighing ReportDocument1 pageBarangay Health Worker Barangay Nutrition Scholar Full Weighing Reportjanessa rosefel franciscoNo ratings yet
- 13TH Cycle Actual MasterlistDocument65 pages13TH Cycle Actual Masterlistkasugabarangay700No ratings yet
- FC - Indacator (Weight For Age)Document4 pagesFC - Indacator (Weight For Age)Glenda Ang BacomoNo ratings yet
- FC - Indacator (Height For Age)Document4 pagesFC - Indacator (Height For Age)Glenda Ang BacomoNo ratings yet
- FC - Indacator (Weight For Height)Document4 pagesFC - Indacator (Weight For Height)Glenda Ang BacomoNo ratings yet
- Growth Excel FormatDocument3 pagesGrowth Excel FormatMelvin Cabanda EbalNo ratings yet
- Inbound 8751315594164507928Document5 pagesInbound 8751315594164507928John Francis Dave BaranganNo ratings yet
- TemplateDocument2 pagesTemplatealyana aurellanaNo ratings yet
- Linda Form OPTDocument2 pagesLinda Form OPTRaquel ParcareyNo ratings yet
- Pregnancy TrackingDocument1 pagePregnancy TrackingKylie GolindangNo ratings yet
- Baclayon Nutritional Status BaselineDocument1 pageBaclayon Nutritional Status BaselineNell CulanagNo ratings yet
- Womens Health UK - 2019 - 12Document132 pagesWomens Health UK - 2019 - 12Leonid BlyumNo ratings yet
- Revised Template of SL and ML For The 12th Cycle ImplementationDocument2 pagesRevised Template of SL and ML For The 12th Cycle Implementationronnie zurbitoNo ratings yet
- CDX Tool 2022 2023Document9 pagesCDX Tool 2022 2023Elaine P. RoqueNo ratings yet
- OPT Plus Form 1Document1 pageOPT Plus Form 1brgycoliatNo ratings yet
- Revised Template of SL and ML For The 12th Cycle Implementation 4Document2 pagesRevised Template of SL and ML For The 12th Cycle Implementation 4Emma DionedaNo ratings yet
- Child Nutritional Status Control CardDocument2 pagesChild Nutritional Status Control CardScribdTranslationsNo ratings yet
- SFP Masterlist, CNS Forms For LGUs 2021-2022Document7 pagesSFP Masterlist, CNS Forms For LGUs 2021-2022XilcaNo ratings yet
- CAÑASDocument4 pagesCAÑASRodolfo CacanantaNo ratings yet
- Bns San Gregorio Monthly Record of Stunted and Severely Stunted 0-23 Months OldDocument1 pageBns San Gregorio Monthly Record of Stunted and Severely Stunted 0-23 Months OldAivee AvenidoNo ratings yet
- Brigada Consolidation 2023Document4 pagesBrigada Consolidation 2023Hyacinth Boots BlandoNo ratings yet
- Master ListDocument2 pagesMaster ListAira ReyesNo ratings yet
- City Address: Anthropometric Data Height - CM HT For Age Weight BMIDocument1 pageCity Address: Anthropometric Data Height - CM HT For Age Weight BMICarmelo Bautista IIINo ratings yet
- Body Mass Index Bmi Nutritional Status of School LearnersDocument13 pagesBody Mass Index Bmi Nutritional Status of School LearnersGean AcabalNo ratings yet
- Division Improvisedphysical Fitness Record SheetDocument3 pagesDivision Improvisedphysical Fitness Record SheetJINKY RAMIREZNo ratings yet
- Deworming 2024 School and District ConsolidationDocument118 pagesDeworming 2024 School and District ConsolidationMadona ParallagNo ratings yet
- Division Improvisedphysical Fitness Record SheetDocument5 pagesDivision Improvisedphysical Fitness Record SheetRYAN BUDUMONo ratings yet
- Pioduran Rural Health Unit: Republic of The Philippines Province of Albay Municipality of PioduranDocument1 pagePioduran Rural Health Unit: Republic of The Philippines Province of Albay Municipality of PioduranFebNo ratings yet
- Baseline EditeddDocument85 pagesBaseline EditeddSylvia N. CantoriaNo ratings yet
- Application Form CaptivateDocument2 pagesApplication Form CaptivateRobi SuaresNo ratings yet
- Dairy and SDGs PDFDocument1 pageDairy and SDGs PDFrubel_nsuNo ratings yet
- 5004 ZoneFoodJournalDocument2 pages5004 ZoneFoodJournalyardenNo ratings yet
- Calorie Tracker Sunday MediumDocument2 pagesCalorie Tracker Sunday Mediumsofia alvesNo ratings yet
- Nutritional Status Report: School Year: Grade Level: Section: Juan Dela CruzDocument2 pagesNutritional Status Report: School Year: Grade Level: Section: Juan Dela CruzGui FawkesNo ratings yet
- A Roadmap To Reduce Stunting: EditorialDocument5 pagesA Roadmap To Reduce Stunting: EditorialWidyaNo ratings yet
- WFP 242524Document88 pagesWFP 242524fikru abrehamNo ratings yet
- Prevalence of Undernutrition and Effectiveness of A Community Based Nutritional Support Programme To Reverse Stunting Among Children Under Five YearsDocument8 pagesPrevalence of Undernutrition and Effectiveness of A Community Based Nutritional Support Programme To Reverse Stunting Among Children Under Five YearsEusabia LiansianiNo ratings yet
- Management of Severe MalnutritionDocument77 pagesManagement of Severe Malnutritionfranklin ifioraNo ratings yet
- Food Cities 2022 - MzuzuDocument2 pagesFood Cities 2022 - MzuzumvulamacfieldNo ratings yet
- What Does The Nutrition Community Expect From UNICEF? by Lawrence Haddad, IFPRIDocument33 pagesWhat Does The Nutrition Community Expect From UNICEF? by Lawrence Haddad, IFPRICallie WhiteNo ratings yet
- Step 1: Formula For Calculation of Global Hunger Index ScoresDocument1 pageStep 1: Formula For Calculation of Global Hunger Index ScoresSunday FiveNo ratings yet
- Egypt Country Strategic Plan 20182023 1Document37 pagesEgypt Country Strategic Plan 20182023 1Eagle EyeNo ratings yet
- Child Growth Sustainable Economic Growth: Why We Should Invest in NutritionDocument5 pagesChild Growth Sustainable Economic Growth: Why We Should Invest in NutritionlawrencehaddadNo ratings yet
- NPS Report Year 1Document93 pagesNPS Report Year 1Open MicrodataNo ratings yet
- Nutrition in The First 1000 DaysDocument7 pagesNutrition in The First 1000 DaysYoki VirgoNo ratings yet
- Growth Assessment and Monitoring During Childhood: CommentaryDocument7 pagesGrowth Assessment and Monitoring During Childhood: CommentaryFajar SetiawanNo ratings yet
- SBI CBO Previous Year Paper 2022Document14 pagesSBI CBO Previous Year Paper 2022RAJESH REDDYNo ratings yet
- Kalimbira - Impact Nutrient Health Program in Malawi - 2009Document10 pagesKalimbira - Impact Nutrient Health Program in Malawi - 2009waitNo ratings yet
- The Brazilian Food Security Scale For Indigenous Guarani Households: Development and ValidationDocument13 pagesThe Brazilian Food Security Scale For Indigenous Guarani Households: Development and ValidationKaterina BlackNo ratings yet
- EngDocument84 pagesEngFanny Romero PalominoNo ratings yet
- Addis Ababa University College of Development Studies Center For Population StudiesDocument65 pagesAddis Ababa University College of Development Studies Center For Population StudiesMinilik Tikur SewNo ratings yet
- 2016 Nutrition Month Theme Focuses On The First 1000 DaysDocument11 pages2016 Nutrition Month Theme Focuses On The First 1000 DaysCar OrdzNo ratings yet
- Role For ODA in Combating Undernutrition - DPCDocument23 pagesRole For ODA in Combating Undernutrition - DPClawrencehaddadNo ratings yet
- Bouma 2016Document16 pagesBouma 2016Eugenia BocaNo ratings yet
- Diet and NutritionDocument42 pagesDiet and Nutritionzaza afifahNo ratings yet
- Mapua-Cwts Program Module 1 (Ay11-12)Document82 pagesMapua-Cwts Program Module 1 (Ay11-12)Diane Anieka0% (1)
- The 1000 Most Critical DaysDocument102 pagesThe 1000 Most Critical DaysloreensinkendeNo ratings yet
- First 1000 Days-Bebe-2Document48 pagesFirst 1000 Days-Bebe-2Alvin QuiranteNo ratings yet
- Essential Nutrition Actions PDFDocument144 pagesEssential Nutrition Actions PDFAmany MokhtarNo ratings yet
- Bangladesh National Conservation StrategyDocument22 pagesBangladesh National Conservation StrategySaeed ShawonNo ratings yet
- Minutes of Meeting Sept 2, 2022Document11 pagesMinutes of Meeting Sept 2, 2022roseannurakNo ratings yet














































































Download as xlsx, pdf, or txt
You might also like
- SAMPLE BNAP 2023 2025 - Template 1Document45 pagesSAMPLE BNAP 2023 2025 - Template 1Maryde Ompoy100% (7)
- Masterlist of ChildrenDocument8 pagesMasterlist of ChildrenJoena Balicao0% (1)
- SFP Masterlist, CNS Forms For LGUs NewDocument4 pagesSFP Masterlist, CNS Forms For LGUs NewJohny F. Villanueva0% (1)
- Fenton Growth Chart Girl v1Document2 pagesFenton Growth Chart Girl v1Hamba Allah75% (4)
- Fenton Growth Chart Boy v1Document2 pagesFenton Growth Chart Boy v1nurhapsari20100% (3)
- Seqota Declaration PresentationDocument17 pagesSeqota Declaration Presentationsimeneh100% (1)
- Crec Masterlist Format V7Document41 pagesCrec Masterlist Format V7John Dalton Marin VelascoNo ratings yet
- Nutritional AssessmentDocument49 pagesNutritional AssessmentIrene Grace Balcueva100% (1)
- Weight Monitoring FormDocument1 pageWeight Monitoring FormChristopher Torres50% (2)
- SFP Revised MasterlistDocument4 pagesSFP Revised MasterlistAaron Dan GlerNo ratings yet
- Nutritional Status Male Female: Nutritional Status: (Using CGS As Reference) OPT-Operation TimbangDocument6 pagesNutritional Status Male Female: Nutritional Status: (Using CGS As Reference) OPT-Operation TimbangBun AhNo ratings yet
- Enhanced CDC NS Monitoring Form Masterlist of Beneficiaries and LGU Consolidation of NS ReportDocument4 pagesEnhanced CDC NS Monitoring Form Masterlist of Beneficiaries and LGU Consolidation of NS ReportluffyNo ratings yet
- Inbound 8077990623609746721Document1 pageInbound 8077990623609746721Careh Maralit AboaboNo ratings yet
- After 120 Forms 1Document4 pagesAfter 120 Forms 1Kenneth Jean EblamoNo ratings yet
- Weight Monitoring Tool NEW For CDWDocument2 pagesWeight Monitoring Tool NEW For CDWronnie zurbitoNo ratings yet
- SF Monitorinf Form After MonthsDocument4 pagesSF Monitorinf Form After MonthsTina TalyodNo ratings yet
- DSWD FeedingDocument2 pagesDSWD FeedingNikko Rey MainitNo ratings yet
- SubredditDocument2 pagesSubredditregine abayonNo ratings yet
- BNS Form No.2Document1 pageBNS Form No.2qw8s5sb9crNo ratings yet
- Pob East Masterlist 2023Document35 pagesPob East Masterlist 2023Sylvia N. CantoriaNo ratings yet
- Barangay Health Worker Barangay Nutrition Scholar Full Weighing ReportDocument1 pageBarangay Health Worker Barangay Nutrition Scholar Full Weighing Reportjanessa rosefel franciscoNo ratings yet
- 13TH Cycle Actual MasterlistDocument65 pages13TH Cycle Actual Masterlistkasugabarangay700No ratings yet
- FC - Indacator (Weight For Age)Document4 pagesFC - Indacator (Weight For Age)Glenda Ang BacomoNo ratings yet
- FC - Indacator (Height For Age)Document4 pagesFC - Indacator (Height For Age)Glenda Ang BacomoNo ratings yet
- FC - Indacator (Weight For Height)Document4 pagesFC - Indacator (Weight For Height)Glenda Ang BacomoNo ratings yet
- Growth Excel FormatDocument3 pagesGrowth Excel FormatMelvin Cabanda EbalNo ratings yet
- Inbound 8751315594164507928Document5 pagesInbound 8751315594164507928John Francis Dave BaranganNo ratings yet
- TemplateDocument2 pagesTemplatealyana aurellanaNo ratings yet
- Linda Form OPTDocument2 pagesLinda Form OPTRaquel ParcareyNo ratings yet
- Pregnancy TrackingDocument1 pagePregnancy TrackingKylie GolindangNo ratings yet
- Baclayon Nutritional Status BaselineDocument1 pageBaclayon Nutritional Status BaselineNell CulanagNo ratings yet
- Womens Health UK - 2019 - 12Document132 pagesWomens Health UK - 2019 - 12Leonid BlyumNo ratings yet
- Revised Template of SL and ML For The 12th Cycle ImplementationDocument2 pagesRevised Template of SL and ML For The 12th Cycle Implementationronnie zurbitoNo ratings yet
- CDX Tool 2022 2023Document9 pagesCDX Tool 2022 2023Elaine P. RoqueNo ratings yet
- OPT Plus Form 1Document1 pageOPT Plus Form 1brgycoliatNo ratings yet
- Revised Template of SL and ML For The 12th Cycle Implementation 4Document2 pagesRevised Template of SL and ML For The 12th Cycle Implementation 4Emma DionedaNo ratings yet
- Child Nutritional Status Control CardDocument2 pagesChild Nutritional Status Control CardScribdTranslationsNo ratings yet
- SFP Masterlist, CNS Forms For LGUs 2021-2022Document7 pagesSFP Masterlist, CNS Forms For LGUs 2021-2022XilcaNo ratings yet
- CAÑASDocument4 pagesCAÑASRodolfo CacanantaNo ratings yet
- Bns San Gregorio Monthly Record of Stunted and Severely Stunted 0-23 Months OldDocument1 pageBns San Gregorio Monthly Record of Stunted and Severely Stunted 0-23 Months OldAivee AvenidoNo ratings yet
- Brigada Consolidation 2023Document4 pagesBrigada Consolidation 2023Hyacinth Boots BlandoNo ratings yet
- Master ListDocument2 pagesMaster ListAira ReyesNo ratings yet
- City Address: Anthropometric Data Height - CM HT For Age Weight BMIDocument1 pageCity Address: Anthropometric Data Height - CM HT For Age Weight BMICarmelo Bautista IIINo ratings yet
- Body Mass Index Bmi Nutritional Status of School LearnersDocument13 pagesBody Mass Index Bmi Nutritional Status of School LearnersGean AcabalNo ratings yet
- Division Improvisedphysical Fitness Record SheetDocument3 pagesDivision Improvisedphysical Fitness Record SheetJINKY RAMIREZNo ratings yet
- Deworming 2024 School and District ConsolidationDocument118 pagesDeworming 2024 School and District ConsolidationMadona ParallagNo ratings yet
- Division Improvisedphysical Fitness Record SheetDocument5 pagesDivision Improvisedphysical Fitness Record SheetRYAN BUDUMONo ratings yet
- Pioduran Rural Health Unit: Republic of The Philippines Province of Albay Municipality of PioduranDocument1 pagePioduran Rural Health Unit: Republic of The Philippines Province of Albay Municipality of PioduranFebNo ratings yet
- Baseline EditeddDocument85 pagesBaseline EditeddSylvia N. CantoriaNo ratings yet
- Application Form CaptivateDocument2 pagesApplication Form CaptivateRobi SuaresNo ratings yet
- Dairy and SDGs PDFDocument1 pageDairy and SDGs PDFrubel_nsuNo ratings yet
- 5004 ZoneFoodJournalDocument2 pages5004 ZoneFoodJournalyardenNo ratings yet
- Calorie Tracker Sunday MediumDocument2 pagesCalorie Tracker Sunday Mediumsofia alvesNo ratings yet
- Nutritional Status Report: School Year: Grade Level: Section: Juan Dela CruzDocument2 pagesNutritional Status Report: School Year: Grade Level: Section: Juan Dela CruzGui FawkesNo ratings yet
- A Roadmap To Reduce Stunting: EditorialDocument5 pagesA Roadmap To Reduce Stunting: EditorialWidyaNo ratings yet
- WFP 242524Document88 pagesWFP 242524fikru abrehamNo ratings yet
- Prevalence of Undernutrition and Effectiveness of A Community Based Nutritional Support Programme To Reverse Stunting Among Children Under Five YearsDocument8 pagesPrevalence of Undernutrition and Effectiveness of A Community Based Nutritional Support Programme To Reverse Stunting Among Children Under Five YearsEusabia LiansianiNo ratings yet
- Management of Severe MalnutritionDocument77 pagesManagement of Severe Malnutritionfranklin ifioraNo ratings yet
- Food Cities 2022 - MzuzuDocument2 pagesFood Cities 2022 - MzuzumvulamacfieldNo ratings yet
- What Does The Nutrition Community Expect From UNICEF? by Lawrence Haddad, IFPRIDocument33 pagesWhat Does The Nutrition Community Expect From UNICEF? by Lawrence Haddad, IFPRICallie WhiteNo ratings yet
- Step 1: Formula For Calculation of Global Hunger Index ScoresDocument1 pageStep 1: Formula For Calculation of Global Hunger Index ScoresSunday FiveNo ratings yet
- Egypt Country Strategic Plan 20182023 1Document37 pagesEgypt Country Strategic Plan 20182023 1Eagle EyeNo ratings yet
- Child Growth Sustainable Economic Growth: Why We Should Invest in NutritionDocument5 pagesChild Growth Sustainable Economic Growth: Why We Should Invest in NutritionlawrencehaddadNo ratings yet
- NPS Report Year 1Document93 pagesNPS Report Year 1Open MicrodataNo ratings yet
- Nutrition in The First 1000 DaysDocument7 pagesNutrition in The First 1000 DaysYoki VirgoNo ratings yet
- Growth Assessment and Monitoring During Childhood: CommentaryDocument7 pagesGrowth Assessment and Monitoring During Childhood: CommentaryFajar SetiawanNo ratings yet
- SBI CBO Previous Year Paper 2022Document14 pagesSBI CBO Previous Year Paper 2022RAJESH REDDYNo ratings yet
- Kalimbira - Impact Nutrient Health Program in Malawi - 2009Document10 pagesKalimbira - Impact Nutrient Health Program in Malawi - 2009waitNo ratings yet
- The Brazilian Food Security Scale For Indigenous Guarani Households: Development and ValidationDocument13 pagesThe Brazilian Food Security Scale For Indigenous Guarani Households: Development and ValidationKaterina BlackNo ratings yet
- EngDocument84 pagesEngFanny Romero PalominoNo ratings yet
- Addis Ababa University College of Development Studies Center For Population StudiesDocument65 pagesAddis Ababa University College of Development Studies Center For Population StudiesMinilik Tikur SewNo ratings yet
- 2016 Nutrition Month Theme Focuses On The First 1000 DaysDocument11 pages2016 Nutrition Month Theme Focuses On The First 1000 DaysCar OrdzNo ratings yet
- Role For ODA in Combating Undernutrition - DPCDocument23 pagesRole For ODA in Combating Undernutrition - DPClawrencehaddadNo ratings yet
- Bouma 2016Document16 pagesBouma 2016Eugenia BocaNo ratings yet
- Diet and NutritionDocument42 pagesDiet and Nutritionzaza afifahNo ratings yet
- Mapua-Cwts Program Module 1 (Ay11-12)Document82 pagesMapua-Cwts Program Module 1 (Ay11-12)Diane Anieka0% (1)
- The 1000 Most Critical DaysDocument102 pagesThe 1000 Most Critical DaysloreensinkendeNo ratings yet
- First 1000 Days-Bebe-2Document48 pagesFirst 1000 Days-Bebe-2Alvin QuiranteNo ratings yet
- Essential Nutrition Actions PDFDocument144 pagesEssential Nutrition Actions PDFAmany MokhtarNo ratings yet
- Bangladesh National Conservation StrategyDocument22 pagesBangladesh National Conservation StrategySaeed ShawonNo ratings yet
- Minutes of Meeting Sept 2, 2022Document11 pagesMinutes of Meeting Sept 2, 2022roseannurakNo ratings yet