Download as pdf or txt
You might also like
- Bengkalis Muria - Jurnal Khusus - Hanifah Hilyah SyahDocument9 pagesBengkalis Muria - Jurnal Khusus - Hanifah Hilyah Syahreza hariansyahNo ratings yet
- Energy Audit of KCC Traction Substation, VijaywadaDocument2 pagesEnergy Audit of KCC Traction Substation, Vijaywadathailamuthu100% (1)
- Emergency and Disaster NursingDocument7 pagesEmergency and Disaster NursingencarguezpaolochelNo ratings yet
- UntitledDocument4 pagesUntitledHannah AmerolNo ratings yet
- Vascular NotesDocument5 pagesVascular NotesAstha Tusharbhai PatelNo ratings yet
- BURNSDocument14 pagesBURNSRIAH BILLANESNo ratings yet
- Gram Negative Bacilli - RespiratoryDocument4 pagesGram Negative Bacilli - RespiratoryrefuapalackyNo ratings yet
- Madrid Surg Notes IntDocument5 pagesMadrid Surg Notes IntdoctorcreepticNo ratings yet
- DV 1Document32 pagesDV 1Mujahidin ArismanNo ratings yet
- Anestesi (Farmakologi)Document15 pagesAnestesi (Farmakologi)Nurul AzizahNo ratings yet
- Burn Depth Characteristics: 1800 ALFREDDocument1 pageBurn Depth Characteristics: 1800 ALFREDNadhila A ByantNo ratings yet
- PA HyperthyroidismDocument7 pagesPA HyperthyroidismEben Alameda-PalapuzNo ratings yet
- Estimated Time of Death:: Cooling of The BodyDocument2 pagesEstimated Time of Death:: Cooling of The BodynoramalinaabdmanafNo ratings yet
- The Immortal SealDocument2 pagesThe Immortal Sealelderfc.librasNo ratings yet
- Kompre Mei 2022 BG RoyDocument74 pagesKompre Mei 2022 BG RoyputriaulianifNo ratings yet
- Pharmacology Exam 2Document3 pagesPharmacology Exam 2Joelle DwekNo ratings yet
- Pressure InjuriesDocument1 pagePressure InjuriesPaola OrtizNo ratings yet
- Inflammatory Diseases of The Skin: M. Angelica Selim, M.D. Dermatopathology Unit Pathology DepartmentDocument53 pagesInflammatory Diseases of The Skin: M. Angelica Selim, M.D. Dermatopathology Unit Pathology DepartmentIsaac MaderoNo ratings yet
- Inflammatory Diseases of The Skin: M. Angelica Selim, M.D. Dermatopathology Unit Pathology DepartmentDocument53 pagesInflammatory Diseases of The Skin: M. Angelica Selim, M.D. Dermatopathology Unit Pathology DepartmentDr Jyotiprakash ChoudhuryNo ratings yet
- The Change The World Board Game: Grammar ReviewDocument2 pagesThe Change The World Board Game: Grammar Reviewlees10088No ratings yet
- Anatomy 2Document1 pageAnatomy 2Casey Rae YanoNo ratings yet
- Bimbingan 7Document4 pagesBimbingan 7sean 102018039No ratings yet
- Bedah 2 Dr. UswaDocument36 pagesBedah 2 Dr. UswaSiq Febri SmnjtkNo ratings yet
- Ent Chanting by DR - ParasDocument34 pagesEnt Chanting by DR - ParasSaravanan DevarajNo ratings yet
- Me 1Document39 pagesMe 1Mansi BansalNo ratings yet
- Name: - LRNDocument2 pagesName: - LRNjrose fay amatNo ratings yet
- 1990s MB - SpreadDocument3 pages1990s MB - SpreadBruno SouzaNo ratings yet
- (DRM) 1.06A Papulosquamous Diseases (Dra. Paliza and Dra. Ismael)Document7 pages(DRM) 1.06A Papulosquamous Diseases (Dra. Paliza and Dra. Ismael)Jolaine ValloNo ratings yet
- OrtopedieDocument40 pagesOrtopedieNaomi CurcanuNo ratings yet
- PlatyhelminthesDocument7 pagesPlatyhelminthesAbhijeet AdhikaryNo ratings yet
- Resumen de Fonetica-Primer CuatrimestreDocument18 pagesResumen de Fonetica-Primer CuatrimestreGonzalo MenaNo ratings yet
- ArthropodsDocument2 pagesArthropodsJulia IshakNo ratings yet
- Kukel WerdDocument3 pagesKukel WerdRicky YurdanaNo ratings yet
- Integumentary SystemDocument7 pagesIntegumentary SystemJOANNA MARIE INVENTORNo ratings yet
- Most Important Questions: Digestion & Absorption Breathing & Exchange of GasesDocument112 pagesMost Important Questions: Digestion & Absorption Breathing & Exchange of GasesRana RikNo ratings yet
- Most Important Questions: Digestion & Absorption Breathing & Exchange of GasesDocument112 pagesMost Important Questions: Digestion & Absorption Breathing & Exchange of GasesRana RikNo ratings yet
- Ent Quick RecapDocument33 pagesEnt Quick Recapshanurajput0No ratings yet
- Integumentary System Reviewer PDF Skin Nail (Anatomy) 2Document1 pageIntegumentary System Reviewer PDF Skin Nail (Anatomy) 2Shiem TrabocNo ratings yet
- CP SynapsesDocument7 pagesCP Synapsespotro patoNo ratings yet
- Dermatology ConditionsDocument8 pagesDermatology ConditionsmeilunlyNo ratings yet
- Flat Raised/ Depressed Raised DepressedDocument6 pagesFlat Raised/ Depressed Raised DepressedMaida PootNo ratings yet
- All Hormones & Disorders - One ShotDocument62 pagesAll Hormones & Disorders - One Shotsalmasaleha806No ratings yet
- Poster (Healable)Document1 pagePoster (Healable)ppnidpk rsumNo ratings yet
- A Wound With Coagulative Necrosis Is Called Burn. A Burn Is A Wound in Which There Is Coagulative Necrosis of The TissueDocument17 pagesA Wound With Coagulative Necrosis Is Called Burn. A Burn Is A Wound in Which There Is Coagulative Necrosis of The Tissuewww nambisons comNo ratings yet
- PikaduraDocument4 pagesPikaduraVictor EduardoNo ratings yet
- Autonomic Nervous System 05 Class Notes MBBS Prof 2nd YearDocument27 pagesAutonomic Nervous System 05 Class Notes MBBS Prof 2nd YeardevNo ratings yet
- Gyne Notes Infections 01Document2 pagesGyne Notes Infections 01kirsten evidenteNo ratings yet
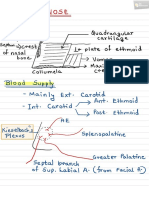
- Nose PDFDocument6 pagesNose PDFNiranjanPandeyNo ratings yet
- EarthwormDocument24 pagesEarthworm10306anshkumarNo ratings yet
- Solutions To Thomas' Calculus Early Transcendentals (9780134439020), Pg. 1031, Ex. 22 Homework Help and Answers SladerDocument1 pageSolutions To Thomas' Calculus Early Transcendentals (9780134439020), Pg. 1031, Ex. 22 Homework Help and Answers SladerNutthanon HwungsawartNo ratings yet
- Ion ChannelsDocument8 pagesIon Channelspotro patoNo ratings yet
- 7 Oragn SystemsDocument11 pages7 Oragn SystemsTobit Andre CaballoNo ratings yet
- Derma 21 Dermatoses From Physical Factors NutritionDocument5 pagesDerma 21 Dermatoses From Physical Factors NutritionKrisha BalorioNo ratings yet
- 2400 Zone v1.2 SinglesDocument4 pages2400 Zone v1.2 SinglesshimmyNo ratings yet
- Pediatric Nursing: Immediate Care For Newborn (OLD)Document8 pagesPediatric Nursing: Immediate Care For Newborn (OLD)KristaRicaAbayabayNo ratings yet
- MIX Reviewer 2022Document54 pagesMIX Reviewer 2022shaikha.amariNo ratings yet
- ANAPHY - Midterms ReviewerDocument15 pagesANAPHY - Midterms ReviewerTiffany WongNo ratings yet
- Health AssessmentDocument48 pagesHealth AssessmentVorgy Bench SantiagoNo ratings yet
- Part I Travel Documents Issued by Third Countries and Territorial Entities en 0Document124 pagesPart I Travel Documents Issued by Third Countries and Territorial Entities en 0drlazyboyNo ratings yet
- FrogDocument65 pagesFrognarayan sahNo ratings yet
- Reasoning and Logic - Lesson 2Document10 pagesReasoning and Logic - Lesson 2Nehal GaurNo ratings yet
- Bohren Et Al Lancet MH Series 4 2023Document12 pagesBohren Et Al Lancet MH Series 4 2023Thierry UhawenimanaNo ratings yet
- Vistamore SDN BHD Project Quality Plan Section 1Document8 pagesVistamore SDN BHD Project Quality Plan Section 1Wan Mohamad Noor Hj IsmailNo ratings yet
- Sheet 6 Electronics - AnswerDocument10 pagesSheet 6 Electronics - AnswerOla SamirNo ratings yet
- Therapeutic Approaches: Indian School MuscatDocument10 pagesTherapeutic Approaches: Indian School MuscatNidhee SharmaNo ratings yet
- Finance AssignmentDocument7 pagesFinance AssignmentMeshack MateNo ratings yet
- Committee Opinion No 664 Refusal of Medically.45Document8 pagesCommittee Opinion No 664 Refusal of Medically.45w yNo ratings yet
- Factors That Affect Time Management of Humanities and Social Sciences Grade 11 Senior High School StudentsDocument8 pagesFactors That Affect Time Management of Humanities and Social Sciences Grade 11 Senior High School StudentsCamile IgnacioNo ratings yet
- Cuaderno de Actividades: Programa Nacional de InglésDocument5 pagesCuaderno de Actividades: Programa Nacional de InglésIselina RNo ratings yet
- Red Bull Copy Paste NetDocument6 pagesRed Bull Copy Paste NetNives AmbrožičNo ratings yet
- Adsorption of Acetic Acid On Charcoal SurfaceDocument3 pagesAdsorption of Acetic Acid On Charcoal SurfaceFrankyFan90% (10)
- 5 Structural Geology March 2019Document117 pages5 Structural Geology March 2019thamirad100% (2)
- Total Brochure UK LoRes 0609 PDFDocument32 pagesTotal Brochure UK LoRes 0609 PDFMohammed RayanNo ratings yet
- PG Medical Admitted Candidates Combined Rank WiseDocument8 pagesPG Medical Admitted Candidates Combined Rank WiseNimesh SommanekNo ratings yet
- Comparative Study of Different Waste Biomass For Energy ApplicationDocument6 pagesComparative Study of Different Waste Biomass For Energy Applicationvitor_alberto_7No ratings yet
- I Am DepressedDocument8 pagesI Am DepressedwisgeorgekwokNo ratings yet
- Electrodes For Titration PDFDocument2 pagesElectrodes For Titration PDFjhuampeNo ratings yet
- Braintech Engineers PVT LTDDocument8 pagesBraintech Engineers PVT LTDMANVENDRA SINGHNo ratings yet
- CLC 18-10Nb: A NB Stabilized 18Cr-10Ni Austenitic Stainless Steel (347 Grade)Document4 pagesCLC 18-10Nb: A NB Stabilized 18Cr-10Ni Austenitic Stainless Steel (347 Grade)PeterWayNo ratings yet
- January: Date Company NameDocument20 pagesJanuary: Date Company NameMatthewNo ratings yet
- N-Channel Enhancement Mode MOSFET: Product SummaryDocument5 pagesN-Channel Enhancement Mode MOSFET: Product Summaryserrano.flia.coNo ratings yet
- Universiti Teknologi Mara Final Examination: Confidential AS/MAR2012/PHY310Document9 pagesUniversiti Teknologi Mara Final Examination: Confidential AS/MAR2012/PHY310luminousspaceNo ratings yet
- Course Syllabus in SuccessionDocument16 pagesCourse Syllabus in SuccessionCharina BalunsoNo ratings yet
- Embragues para Motores EstacionariosDocument12 pagesEmbragues para Motores EstacionariosJiyaYsqn100% (1)
- West Nile Virus Associated With Equid Encephalitis in Brazil, 2018Document10 pagesWest Nile Virus Associated With Equid Encephalitis in Brazil, 2018Monica Shinneider de SousaNo ratings yet
- Project Fianace 1Document46 pagesProject Fianace 17karswapnilNo ratings yet
- SAMAP 15 ProceedingsDocument84 pagesSAMAP 15 ProceedingsOm Parkash SharmaNo ratings yet
- Income Tax NotesDocument18 pagesIncome Tax NotesVikash kumarNo ratings yet
- Motives IDocument10 pagesMotives Imerin sunilNo ratings yet