Download as pdf or txt
You might also like
- Eagle Research Remedy Maker ManualDocument20 pagesEagle Research Remedy Maker Manualsigilum_dei67% (3)
- Bladder CancerDocument21 pagesBladder CancerJaime JaimexNo ratings yet
- PART 2 Coran Pediatric Surgery, 7th Ed PDFDocument350 pagesPART 2 Coran Pediatric Surgery, 7th Ed PDFRamona Cerasela Petreaca100% (4)
- Donor Milk Banking and Breastfeeding in NorwayDocument6 pagesDonor Milk Banking and Breastfeeding in NorwayFrieta Diaz AstutiNo ratings yet
- Impact of Right Waste Disposal To The Residents of Barangay 171, CaloocanDocument12 pagesImpact of Right Waste Disposal To The Residents of Barangay 171, CaloocanAljay Mirandilla100% (1)
- AR 2009-2010 WebDocument36 pagesAR 2009-2010 WebOsu OphthalmologyNo ratings yet
- Seeking SafetyDocument17 pagesSeeking Safetyapi-24985177883% (6)
- Genes: Thyroid Cancer in The Pediatric PopulationDocument20 pagesGenes: Thyroid Cancer in The Pediatric PopulationgalihidolamuNo ratings yet
- Papillary Thyroid CarcinomaDocument9 pagesPapillary Thyroid CarcinomaELinkTulusNo ratings yet
- Zoltick 2011Document8 pagesZoltick 2011jedan185No ratings yet
- Thyroid Nodule PDFDocument21 pagesThyroid Nodule PDFrima oktariniNo ratings yet
- Papillary Thyroid CarcinomaDocument17 pagesPapillary Thyroid CarcinomaEster Sibarani100% (2)
- Tumores CerebralesDocument24 pagesTumores CerebralesRocio LedesmaNo ratings yet
- 2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentDocument9 pages2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentCharley WangNo ratings yet
- Onco Ch68 Colorectal CarcinaomaDocument21 pagesOnco Ch68 Colorectal CarcinaomaZazaNo ratings yet
- Papillary Thyroid Cancer: Genetic Alterations and Molecular Biomarker InvestigationsDocument11 pagesPapillary Thyroid Cancer: Genetic Alterations and Molecular Biomarker InvestigationsRum Afida RasfaNo ratings yet
- 07 Central Nervous System TumorsDocument25 pages07 Central Nervous System TumorsRolando Rocha AtenciaNo ratings yet
- Psu 50318Document4 pagesPsu 50318Dr Venkatachalapathy T S Ped SurgeonNo ratings yet
- Semb 57 287Document18 pagesSemb 57 287samruizayalaNo ratings yet
- Cancer Org 2014Document18 pagesCancer Org 2014Antonieta PérezNo ratings yet
- Thyroid Cancer: Burden of Illness and Management of Disease: J o U R N A L o F C A N C e RDocument7 pagesThyroid Cancer: Burden of Illness and Management of Disease: J o U R N A L o F C A N C e REndang Rahayu Fuji LestaryNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Acc 59 s1 66Document7 pagesAcc 59 s1 66luzvi1708No ratings yet
- Thyroid Disorders: Evaluation and Management of Thyroid NodulesDocument13 pagesThyroid Disorders: Evaluation and Management of Thyroid NodulesГулпе АлексейNo ratings yet
- Pet ThyroidsDocument21 pagesPet ThyroidsdrmolinammNo ratings yet
- PTC GeneDocument17 pagesPTC GeneDr CommissionerNo ratings yet
- The Oncologist - 2007 - Chintagumpala - Retinoblastoma Review of Current ManagementDocument10 pagesThe Oncologist - 2007 - Chintagumpala - Retinoblastoma Review of Current ManagementSyaphoetraNo ratings yet
- Smith 2017Document14 pagesSmith 2017Evelynππ θσυNo ratings yet
- Childhood Cancer Literature ReviewDocument4 pagesChildhood Cancer Literature Reviewafmzjbxmbfpoox100% (1)
- Oral Cancer-GeneticsDocument18 pagesOral Cancer-GeneticsAlberto FilhoNo ratings yet
- Anaplastic Thyroid Cancer Diagnosis and ManagementDocument16 pagesAnaplastic Thyroid Cancer Diagnosis and ManagementKimberly Andrea Gramajo OrozcoNo ratings yet
- Soft Tissue Tumors6 - 0Document16 pagesSoft Tissue Tumors6 - 0Romy MinascurtaNo ratings yet
- Thyroid Cancer: Burden of Illness and Management of Disease: J o U R N A L o F C A N C e RDocument7 pagesThyroid Cancer: Burden of Illness and Management of Disease: J o U R N A L o F C A N C e RRum Afida RasfaNo ratings yet
- SCLC LancetDocument15 pagesSCLC LancetLeeTomNo ratings yet
- Pediatricneuro-Oncology: Fatema MalbariDocument17 pagesPediatricneuro-Oncology: Fatema MalbariRandy UlloaNo ratings yet
- Testicular CancerDocument12 pagesTesticular Cancerghost_724No ratings yet
- Embryonal CnsDocument13 pagesEmbryonal CnsPoly EdayanalNo ratings yet
- Paediatric Pituitary Adenomas - A Decade of ChangeDocument11 pagesPaediatric Pituitary Adenomas - A Decade of Changemelany.sanchezNo ratings yet
- Research Paper On Testicular CancerDocument5 pagesResearch Paper On Testicular Cancerfvdddmxt100% (1)
- I. Primary 1. Epithelial 2. Non-EpithelialDocument25 pagesI. Primary 1. Epithelial 2. Non-EpithelialSifu Perniagaan MayaNo ratings yet
- Holt EH - Current Evaluation of Thyroid Nodule. Med Clin N Am. 2021Document15 pagesHolt EH - Current Evaluation of Thyroid Nodule. Med Clin N Am. 2021LUCIA LOPERA LÓPEZNo ratings yet
- TERATOMADocument7 pagesTERATOMAKrishan_Bansal_2247No ratings yet
- Viatori 2012Document10 pagesViatori 2012jedan185No ratings yet
- Polyp Genetics: Coen Laurens Klos, MD Sekhar Dharmarajan, MDDocument7 pagesPolyp Genetics: Coen Laurens Klos, MD Sekhar Dharmarajan, MDMarjuani yusufNo ratings yet
- Thyroid Carcinoma: Phenotypic Features, Underlying Biology and Potential Relevance For Targeting TherapyDocument25 pagesThyroid Carcinoma: Phenotypic Features, Underlying Biology and Potential Relevance For Targeting TherapyrakaNo ratings yet
- Jurnal Kanker TestisDocument9 pagesJurnal Kanker TestisDiatni FibriNo ratings yet
- 624 PDFDocument9 pages624 PDFTri AryantiNo ratings yet
- Testis CancerDocument9 pagesTestis CancerMuhammad Tawfiq ZamriNo ratings yet
- 331-Book Chapter-3614-2-10-20210406Document20 pages331-Book Chapter-3614-2-10-20210406Yolla GitamayaNo ratings yet
- Genetic-Guidedrisk Assessmentand Managementofthyroidcancer: Mingzhao XingDocument16 pagesGenetic-Guidedrisk Assessmentand Managementofthyroidcancer: Mingzhao XingPedro Gómez RNo ratings yet
- Molecular Genetics of Colorectal CancerDocument6 pagesMolecular Genetics of Colorectal Cancermuhammad rizqi romadlonNo ratings yet
- Genetica 1Document9 pagesGenetica 1Jose Andres DiazNo ratings yet
- s40644 015 0040 6 PDFDocument14 pagess40644 015 0040 6 PDFMarco SaptennoNo ratings yet
- Ovarian Cancer - StatPearls - NCBI BookshelfDocument13 pagesOvarian Cancer - StatPearls - NCBI BookshelfeeeeeeNo ratings yet
- Cripe2017 2750523Document4 pagesCripe2017 2750523فرجني موغNo ratings yet
- Testicular Involvement of Acute Lymphoblastic Leukemia in Children and Adolescents: Diagnosis, Biology, and ManagementDocument15 pagesTesticular Involvement of Acute Lymphoblastic Leukemia in Children and Adolescents: Diagnosis, Biology, and ManagementabdullahNo ratings yet
- Sacrococcygeal Teratoma A Tumor at The Center of EmbryogenesisDocument8 pagesSacrococcygeal Teratoma A Tumor at The Center of EmbryogenesisLuis Ruelas SanchezNo ratings yet
- I. Primary 1. Epithelial 2. Non-EpithelialDocument25 pagesI. Primary 1. Epithelial 2. Non-EpithelialSifu Perniagaan MayaNo ratings yet
- Brain TumorsDocument12 pagesBrain Tumors36Kushal saNdHuNo ratings yet
- Kju 55 789Document8 pagesKju 55 789Muhammad Tawfiq ZamriNo ratings yet
- Molecular Genetics of Colorectal Cancer - UpToDateDocument35 pagesMolecular Genetics of Colorectal Cancer - UpToDateHartemes RosarioNo ratings yet
- Peran - Dokter - Gigi - Anak - Menurut - Protokol - KankerDocument13 pagesPeran - Dokter - Gigi - Anak - Menurut - Protokol - KankeratmokotomoNo ratings yet
- Management of WilmsDocument8 pagesManagement of WilmsArdhito BudhijuwonoNo ratings yet
- HandbookDocument4 pagesHandbookDr Venkatachalapathy T S Ped SurgeonNo ratings yet
- Pediatric Acute Lymphoblastic LeukemiaFrom EverandPediatric Acute Lymphoblastic LeukemiaMotohiro KatoNo ratings yet
- Standards of Care For Breeders of Companion Animals ActDocument9 pagesStandards of Care For Breeders of Companion Animals ActBCLiberalCaucusNo ratings yet
- Chapter 3 - Basic Attending Basic Attending and Listening Skills and Listening SkillsDocument9 pagesChapter 3 - Basic Attending Basic Attending and Listening Skills and Listening SkillsKrishno RaeNo ratings yet
- Nutraceuticals Leaflet ENGDocument2 pagesNutraceuticals Leaflet ENGDr. Dragos CobzariuNo ratings yet
- Asian Music Research - J.C GarciaDocument5 pagesAsian Music Research - J.C GarciaJomel GarciaNo ratings yet
- 60 Seconds Weight Loss Inspiration Book PDFDocument192 pages60 Seconds Weight Loss Inspiration Book PDFberlinczyk100% (2)
- Endodoncia Vs ImplantesDocument8 pagesEndodoncia Vs ImplantesSebastián BernalNo ratings yet
- Resolving Anticipatory Grief and Enhancing DignityDocument15 pagesResolving Anticipatory Grief and Enhancing DignityDian Oktaria SafitriNo ratings yet
- DM Prospectus v5Document50 pagesDM Prospectus v5Aura-Elena BugusNo ratings yet
- Format Catatan Harian Pemakaian Obat NovemberDocument33 pagesFormat Catatan Harian Pemakaian Obat NovemberIntan YuliaNo ratings yet
- Quiz RheumDocument20 pagesQuiz RheumAzizan HannyNo ratings yet
- Lesser Known Facts About Tryptophan Side Effects: What Are The Problems With Tryptophan?Document26 pagesLesser Known Facts About Tryptophan Side Effects: What Are The Problems With Tryptophan?stambicaNo ratings yet
- Herbal Gram Index v1-67Document86 pagesHerbal Gram Index v1-67terryvnd50% (2)
- Advil - PLUS - FA - For - Download - ENGLISHDocument2 pagesAdvil - PLUS - FA - For - Download - ENGLISHShuvroNo ratings yet
- ANAESTHESIA FOR GASTROINTESTINAL CANCER SURGERIES AutosavedDocument40 pagesANAESTHESIA FOR GASTROINTESTINAL CANCER SURGERIES AutosavedKavyasree KatamNo ratings yet
- Vocabulary Exercises: 1) Complete in The Correct WayDocument5 pagesVocabulary Exercises: 1) Complete in The Correct Waylaura1pinilla1domingNo ratings yet
- Guidelines For Nurses Performing TriageDocument4 pagesGuidelines For Nurses Performing TriagedroenNo ratings yet
- CATARACTS and GLAUCOMADocument11 pagesCATARACTS and GLAUCOMAAmoroso, Marian Corneth D.No ratings yet
- CancerDocument70 pagesCancerapi-3735995100% (1)
- 463 - Fis 313Document6 pages463 - Fis 313shuklasd3221No ratings yet
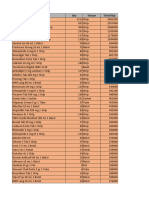
- Tugas Pareto - Elsa Irnandari - 188114130Document17 pagesTugas Pareto - Elsa Irnandari - 188114130elsaairnandari13No ratings yet
- What Is AcupunctureDocument2 pagesWhat Is AcupunctureBhaskaranNo ratings yet
- Review of Hospital Drinking Water Supply Options For KGHDocument16 pagesReview of Hospital Drinking Water Supply Options For KGHtrishincyberspaceNo ratings yet
- Mindfulness Exercise 1: Be-Still Mindfulness: (Approximately 5-10 Minutes)Document1 pageMindfulness Exercise 1: Be-Still Mindfulness: (Approximately 5-10 Minutes)blakeloganNo ratings yet
- Sulfonamide SDocument4 pagesSulfonamide SAhmed MadboulyNo ratings yet
- Vitamin b12 and Pregnancy - With ReferencesDocument2 pagesVitamin b12 and Pregnancy - With Referencesapi-271190857No ratings yet