Download as pdf or txt
You might also like
- Akt Notes VtsDocument50 pagesAkt Notes VtsMin Maw100% (1)
- Update On Antimalarials and Systemic Lupus Erythematosus: ReviewDocument11 pagesUpdate On Antimalarials and Systemic Lupus Erythematosus: ReviewVerónica Duménez JofréNo ratings yet
- Cba 2Document2 pagesCba 2Najib Al FatinNo ratings yet
- Barrera Hematoencefaolica y Farmacocinetica Atb SNC 2020Document37 pagesBarrera Hematoencefaolica y Farmacocinetica Atb SNC 2020Ru MNo ratings yet
- Clinical Profile of Patients Admitted With Hyponatremia in The Medical Intensive Care UnitDocument6 pagesClinical Profile of Patients Admitted With Hyponatremia in The Medical Intensive Care UnitjjpulikenNo ratings yet
- Hemodynamic Assessment and Management of Septic.7Document12 pagesHemodynamic Assessment and Management of Septic.7noopstabNo ratings yet
- 04 JorablooDocument6 pages04 Jorabloogede ekaNo ratings yet
- Hidrocortisona Vs Choque SepticoDocument12 pagesHidrocortisona Vs Choque SepticoMarisolCamposNo ratings yet
- Monitored Anesthesia Care An OverviewDocument3 pagesMonitored Anesthesia Care An OverviewLestari Chye PouedanNo ratings yet
- Comparison of Clonidine and Fentanyl As An Adjuvant To Bupivacaine in Unilateral Spinal AnaesthesiaDocument11 pagesComparison of Clonidine and Fentanyl As An Adjuvant To Bupivacaine in Unilateral Spinal AnaesthesiaYadin SabudiNo ratings yet
- Homeopathic Remedies Will Be The Pharmacological Means of Evidence For Informational MedicineDocument4 pagesHomeopathic Remedies Will Be The Pharmacological Means of Evidence For Informational MedicineMayuresh NaikNo ratings yet
- Colistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM EvidenceDocument27 pagesColistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM Evidencerac.oncologyNo ratings yet
- Guillain-Barré Syndrome: Outcome of Treatment by IVIG vs. Methylprednisolone in Pediatric Intensive Care Unit of A Tertiary Care HospitalDocument7 pagesGuillain-Barré Syndrome: Outcome of Treatment by IVIG vs. Methylprednisolone in Pediatric Intensive Care Unit of A Tertiary Care HospitalAlisa NajwaNo ratings yet
- 0 - Ceor 10 747Document13 pages0 - Ceor 10 747Ika RohaetiNo ratings yet
- Cópia de HU - ReviewDocument6 pagesCópia de HU - ReviewMarcio Lucio Candor MorillaNo ratings yet
- Jur Nal LLLLLDocument9 pagesJur Nal LLLLLsabrina nurNo ratings yet
- Antibiotico en SepsisDocument15 pagesAntibiotico en SepsisJuan RodriguezNo ratings yet
- Siadh!!!Document10 pagesSiadh!!!Febri Dwi HaryonoNo ratings yet
- PreprintCOVID - 192 - 3 IvermectinaDocument18 pagesPreprintCOVID - 192 - 3 IvermectinaOmar CruzNo ratings yet
- Hidradenitis SupuratifDocument9 pagesHidradenitis SupuratifRidho ForesNo ratings yet
- Editorials: (4), While Inducing A Longer-Lived Protein (Insulin-LikeDocument2 pagesEditorials: (4), While Inducing A Longer-Lived Protein (Insulin-LikeAriSuandiNo ratings yet
- Sepsis Treatment - Multiple ApproachesDocument5 pagesSepsis Treatment - Multiple Approachesgoutham sivasailamNo ratings yet
- Therapeutic Drug Monitoring of Biologics For Patients With Inflammatory Bowel Diseases: How, When, and For Whom?Document10 pagesTherapeutic Drug Monitoring of Biologics For Patients With Inflammatory Bowel Diseases: How, When, and For Whom?paula costa LeandroNo ratings yet
- Antibiotic Stewardship and Therapeutic Drug.10Document9 pagesAntibiotic Stewardship and Therapeutic Drug.10Khanh Ha NguyenNo ratings yet
- Clinical Characterization Cohort Systemic Lupus Erythematosus. PLoS One-2023Document14 pagesClinical Characterization Cohort Systemic Lupus Erythematosus. PLoS One-2023Jorge Ricardo Parra CamachoNo ratings yet
- Antibiotic Strategies in Severe Nosocomial Sepsis: Why Do We Not De-Escalate More Often?Document7 pagesAntibiotic Strategies in Severe Nosocomial Sepsis: Why Do We Not De-Escalate More Often?Anonymous 2kPiJhIlFNo ratings yet
- Bedaquiline, Delamanid, Linezolid, and Clofazimine For Treatment of Pre-Extensively Drug-Resistant Tuberculosis 2022Document9 pagesBedaquiline, Delamanid, Linezolid, and Clofazimine For Treatment of Pre-Extensively Drug-Resistant Tuberculosis 2022awaluddin andyNo ratings yet
- Hiperhidrosis ArticuloDocument8 pagesHiperhidrosis ArticuloPedro Mercado PuelloNo ratings yet
- Managing Hemoptysis What To Do or What Not To DoDocument4 pagesManaging Hemoptysis What To Do or What Not To Dodoc_next_doorNo ratings yet
- Community Acquired Bacterial Pneumonia in Adults .7Document16 pagesCommunity Acquired Bacterial Pneumonia in Adults .7velu sNo ratings yet
- Clinical Pharmacology of Antibiotics.22Document11 pagesClinical Pharmacology of Antibiotics.22Josette LeyvaNo ratings yet
- Cytokine Septic ShockDocument13 pagesCytokine Septic ShockEduardo ChanonaNo ratings yet
- News & Views: Restrictive Fluid Therapy and High-Dose Vitamin C in SepsisDocument2 pagesNews & Views: Restrictive Fluid Therapy and High-Dose Vitamin C in SepsisLAURA ALEJANDRA GONZALEZ MONTOYANo ratings yet
- CAP Treatamnet AcortadoDocument8 pagesCAP Treatamnet Acortadoapi-3707490No ratings yet
- Bug and DrugDocument12 pagesBug and DrugJair Alexander Quintero PanucoNo ratings yet
- Laprosy Research Paper (Ahmed Tanjimul Islam)Document7 pagesLaprosy Research Paper (Ahmed Tanjimul Islam)AHMED TANJIMUL ISLAMNo ratings yet
- Articulo. DIAGNOSTICO DEL PACIENTE INTOXICADODocument7 pagesArticulo. DIAGNOSTICO DEL PACIENTE INTOXICADOJosé Rafael Reyes NavaNo ratings yet
- Bmjopen 2022 065045Document6 pagesBmjopen 2022 065045pankaj daganiNo ratings yet
- Effective Hemodynamic Monitoring 2Document10 pagesEffective Hemodynamic Monitoring 2Shirley castañedaNo ratings yet
- Antibacterial Therapeutic Drug Monitoring in CerebrospinalDocument5 pagesAntibacterial Therapeutic Drug Monitoring in CerebrospinalaNo ratings yet
- Hypoalbuminemia As Surrogate and Culprit of Infections: Molecular SciencesDocument25 pagesHypoalbuminemia As Surrogate and Culprit of Infections: Molecular SciencesPutri SatrianyNo ratings yet
- Acdfne - Efectos Sistémicos y Pulmonares de Hidrocortisona en Prematuros Ventilados - Nienke HalmeijerDocument245 pagesAcdfne - Efectos Sistémicos y Pulmonares de Hidrocortisona en Prematuros Ventilados - Nienke HalmeijerChristian Isaac Rodriguez MoranNo ratings yet
- Dialog Iq: Challenge The ThinkingDocument14 pagesDialog Iq: Challenge The ThinkingMahmood Al.HarrasiNo ratings yet
- Mechanism of Action of Acupuncture in Obesity: A Perspective From The HypothalamusDocument15 pagesMechanism of Action of Acupuncture in Obesity: A Perspective From The HypothalamusMaurocoNo ratings yet
- Subphenotypes of Acute Kidney Injury 2022Document6 pagesSubphenotypes of Acute Kidney Injury 2022Juan Diego JImenez AlvizoNo ratings yet
- Volume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1Document8 pagesVolume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1fatima amaliaNo ratings yet
- Anestesia Hipertension I PDFDocument6 pagesAnestesia Hipertension I PDFDiego SolaqueNo ratings yet
- KJP 34 4 509Document25 pagesKJP 34 4 509foto pasienNo ratings yet
- Enteral1 PDFDocument10 pagesEnteral1 PDFCarlos Eduardo FerrazNo ratings yet
- 10.1515 - Labmed 2023 0085Document8 pages10.1515 - Labmed 2023 0085Arturo Eduardo Huarcaya OntiverosNo ratings yet
- 63-PRINCIPLESOFPHARMADocument16 pages63-PRINCIPLESOFPHARMAKenneth MiguelNo ratings yet
- Antimicrobial Agents and Chemotherapy-2010-Pea-4605.fullDocument6 pagesAntimicrobial Agents and Chemotherapy-2010-Pea-4605.fullGül BaktırNo ratings yet
- Bigmed As A Very Novel Method Based Onoral Immunogenetic Therapy To Prevent Andtreat Allergic Diseases Especially AsthmaDocument10 pagesBigmed As A Very Novel Method Based Onoral Immunogenetic Therapy To Prevent Andtreat Allergic Diseases Especially AsthmaGines RoaNo ratings yet
- Hypertonic (3%) Saline Vs 0.9% Saline Nebulization For Acute Viral Bronchiolitis: A Randomized Controlled TrialDocument5 pagesHypertonic (3%) Saline Vs 0.9% Saline Nebulization For Acute Viral Bronchiolitis: A Randomized Controlled TrialMukesh Kumar GuptaNo ratings yet
- 16 RaDocument10 pages16 RaNitish TankNo ratings yet
- Calcium Dobesilate in Symptomatic Treatment of Hemorrhoidal Disease: An Interventional StudyDocument3 pagesCalcium Dobesilate in Symptomatic Treatment of Hemorrhoidal Disease: An Interventional StudyN R Reddy HemanthNo ratings yet
- 2145-Article Text-10388-2-10-20210414Document5 pages2145-Article Text-10388-2-10-20210414TommyNo ratings yet
- Dupilumab EPOC NEJM 2024Document10 pagesDupilumab EPOC NEJM 2024Alan GamboaNo ratings yet
- Efficacy and Safety of Oral Administration of A Mixture of Probiotic Strains in Patients With Psoriasis: A Randomized Controlled Clinical TrialDocument7 pagesEfficacy and Safety of Oral Administration of A Mixture of Probiotic Strains in Patients With Psoriasis: A Randomized Controlled Clinical TrialHafid Adi NugrohoNo ratings yet
- Neurokinin-1 Receptor Antagonists Review of Their Role For The Prevention of Chemotherapy-Induced Nausea and Vomiting in AdultsDocument21 pagesNeurokinin-1 Receptor Antagonists Review of Their Role For The Prevention of Chemotherapy-Induced Nausea and Vomiting in Adults479 801Muhammad Luthfan AdaniNo ratings yet
- s10877 024 01146 1Document19 pagess10877 024 01146 1Kelly Enedina NunesNo ratings yet
- 10.1007@s00134 017 4935 5Document2 pages10.1007@s00134 017 4935 5Kelly Enedina NunesNo ratings yet
- Gattinoni Et Al-2024-Intensive Care MedicineDocument3 pagesGattinoni Et Al-2024-Intensive Care MedicineKelly Enedina NunesNo ratings yet
- Electrical Impedance Tomography: The Electrocardiogram For The LungsDocument3 pagesElectrical Impedance Tomography: The Electrocardiogram For The LungsKelly Enedina NunesNo ratings yet
- Towards The Automatic Detection and Correction of Abnormal Arterial Pressure WaveformsDocument4 pagesTowards The Automatic Detection and Correction of Abnormal Arterial Pressure WaveformsKelly Enedina NunesNo ratings yet
- 2020 Focused Transesophageal Echocardiography During Cardiac Arrest ResuscitationDocument10 pages2020 Focused Transesophageal Echocardiography During Cardiac Arrest Resuscitationbogeg74816No ratings yet
- Imple Remedies (Totkas) For Success, Growth and ProsperityDocument5 pagesImple Remedies (Totkas) For Success, Growth and ProsperityDmmi Fzco100% (3)
- Mas 2Document7 pagesMas 2Nofiya RuswantiNo ratings yet
- Renr Review Ras Practice Test 30Document23 pagesRenr Review Ras Practice Test 30arkelliaNo ratings yet
- Final Project KIN 1400Document10 pagesFinal Project KIN 1400Trainer HermanNo ratings yet
- CHN-Lecture Module 1 and 2Document64 pagesCHN-Lecture Module 1 and 2mirai desu100% (2)
- Clinical Audit On One Hour Sepsis Bundle in Our HospitalDocument2 pagesClinical Audit On One Hour Sepsis Bundle in Our HospitalAnonymous lAfk9gNPNo ratings yet
- Subcortical Ischemic Vascular Dementia: Helena C. Chui, MDDocument24 pagesSubcortical Ischemic Vascular Dementia: Helena C. Chui, MDEugenia FiginiNo ratings yet
- Nurse Labs Practice Test 7 PDFDocument4 pagesNurse Labs Practice Test 7 PDFNatalie Pemberton-ParrisNo ratings yet
- Epi FinalDocument481 pagesEpi FinalSana Savana Aman R100% (1)
- 3 Neonatal InfectionDocument56 pages3 Neonatal InfectiondindaamalaNo ratings yet
- 2 Merz Institute Skin Laxity LU 2summary PDFDocument5 pages2 Merz Institute Skin Laxity LU 2summary PDFMafer ArizaNo ratings yet
- Comparative Effects of Pulsed and Continuous Short Wave Diathermy On Pain and Selected Physiological Parameters Among Subjects With Chronic Knee OsteoarthritisDocument10 pagesComparative Effects of Pulsed and Continuous Short Wave Diathermy On Pain and Selected Physiological Parameters Among Subjects With Chronic Knee Osteoarthritisjansen irawanNo ratings yet
- Ebook The Brigham Intensive Review of Internal Medicine Question Answer Companion PDF Full Chapter PDFDocument67 pagesEbook The Brigham Intensive Review of Internal Medicine Question Answer Companion PDF Full Chapter PDFsara.freese515100% (36)
- L2RA Blank Form - NewDocument35 pagesL2RA Blank Form - NewAmel Rayhan AiraNo ratings yet
- Asacs - Newsletter - Apr - Jun - 2010 - Final & Rectified On 11-10-10Document24 pagesAsacs - Newsletter - Apr - Jun - 2010 - Final & Rectified On 11-10-10devainetNo ratings yet
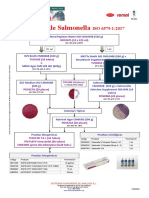
- Salmonella ISO 6579 2017Document1 pageSalmonella ISO 6579 2017Đăng Lưu100% (1)
- De Thi Hoc Sinh Gioi Lop 12 Mon Tieng Anh Nam Hoc 2018 2019Document13 pagesDe Thi Hoc Sinh Gioi Lop 12 Mon Tieng Anh Nam Hoc 2018 2019Bảo Khánh Lê MaiNo ratings yet
- Overview of DissociationDocument8 pagesOverview of DissociationDr Nisrine MoussaouiNo ratings yet
- Poster SpecCircs Anaphylaxis Treatment Algorithm ENG V20151001 HRES Site PDFDocument1 pagePoster SpecCircs Anaphylaxis Treatment Algorithm ENG V20151001 HRES Site PDFPetrarkina LauraNo ratings yet
- BEmONC - Facilitator's Handbook - 2013 April - FinalDocument286 pagesBEmONC - Facilitator's Handbook - 2013 April - FinalElizabeth Nionzima100% (2)
- Latihan Soal UTBK 2021 - Set 2Document6 pagesLatihan Soal UTBK 2021 - Set 2Zidna IlmaNo ratings yet
- Wongs Nursing Care of Infants and Children 10th Edition Hockenberry Test BankDocument14 pagesWongs Nursing Care of Infants and Children 10th Edition Hockenberry Test BankNicoleRoweanbtc100% (9)
- PostureDocument2 pagesPostureNader MorrisNo ratings yet
- Calymmatobacterium Granulomatis As Klebsiella Granulomatis Comb. NovDocument6 pagesCalymmatobacterium Granulomatis As Klebsiella Granulomatis Comb. NovErtyWitalayaL.ToruanNo ratings yet
- Functional Capacity Evaluation and Chiropractic Case ManagementDocument11 pagesFunctional Capacity Evaluation and Chiropractic Case ManagementrojexeNo ratings yet
- Causes and Control of Unfruitfulness in Fruit CropsDocument29 pagesCauses and Control of Unfruitfulness in Fruit CropsDr. Govind VishwakarmaNo ratings yet
- GoodDocument22 pagesGoodhari sharma100% (1)
- DRUG STUDY AmoxicillinDocument2 pagesDRUG STUDY AmoxicillinKhylamarie VillalunaNo ratings yet