Download as pdf or txt
You might also like
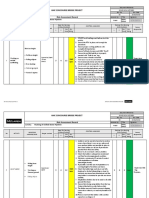
- Risk Assessment For Flushing of Chilled Water PipingDocument9 pagesRisk Assessment For Flushing of Chilled Water PipingAnandu AshokanNo ratings yet
- Mental Status Assessment: A. General Appearance The Patient Grooming WasDocument4 pagesMental Status Assessment: A. General Appearance The Patient Grooming Wassandyzgurl100% (3)
- Psychology and Abnormality Notes - CIE Psychology A-LevelDocument17 pagesPsychology and Abnormality Notes - CIE Psychology A-LevelRajasekar Krishnasamy100% (1)
- Unit IG2 Risk AssessmentDocument13 pagesUnit IG2 Risk AssessmentAbdulla KurupkarNo ratings yet
- Daat12i2p394conversion Disorder and Physical TherapyDocument4 pagesDaat12i2p394conversion Disorder and Physical Therapydonleo153100% (1)
- Chapter 15 - Health and Physical Assessment of The Adult ClientDocument65 pagesChapter 15 - Health and Physical Assessment of The Adult ClientKristian Jane de Jesus100% (1)
- Closure of Minor Skin Wounds With Sutures - UpToDate2019 PDFDocument32 pagesClosure of Minor Skin Wounds With Sutures - UpToDate2019 PDFGerii Pucllas VillarNo ratings yet
- Dubai Construction Safety RegulationsDocument38 pagesDubai Construction Safety Regulationsfannounm100% (4)
- Neurological Assessment Seminar TopicDocument19 pagesNeurological Assessment Seminar TopicKhirabdhi Tanaya SahuNo ratings yet
- Mental Status ExaminationDocument9 pagesMental Status ExaminationDolly DuttaNo ratings yet
- Mental Status EvaluationDocument7 pagesMental Status Evaluationmunir houseNo ratings yet
- Mental Status Examination - StatPearls - NCBI BookshelfDocument9 pagesMental Status Examination - StatPearls - NCBI BookshelfGRUPO DE INTERES EN PSIQUIATRIANo ratings yet
- Mental Status Examination: Level of ConsciousnessDocument4 pagesMental Status Examination: Level of Consciousnessmonica bayaoaNo ratings yet
- Assessment of Neurologic Function: Dr. Lubna DwerijDocument41 pagesAssessment of Neurologic Function: Dr. Lubna DwerijNoor MajaliNo ratings yet
- Mental Status ExaminationDocument21 pagesMental Status ExaminationAthul RajNo ratings yet
- Assessment of NeurologyDocument33 pagesAssessment of NeurologyDR. KUMARASWAMI HEALTH CENTRE COLLEGE OF NURSING KANYAKUMARINo ratings yet
- Appearance and General BehaviorDocument3 pagesAppearance and General BehaviorHardeep KaurNo ratings yet
- Mental Status ExaminationDocument35 pagesMental Status ExaminationSANU RAMASWAMY80% (10)
- The Mental Status ExaminationDocument14 pagesThe Mental Status ExaminationkamienlamNo ratings yet
- Schizophrenia Clinical Presentation - History, Physical Examination, ComplicationsDocument4 pagesSchizophrenia Clinical Presentation - History, Physical Examination, ComplicationsdilaNo ratings yet
- The Mental Status ExaminationDocument10 pagesThe Mental Status ExaminationSalvara Jane DanielNo ratings yet
- Conversion DisorderDocument2 pagesConversion DisorderThe Lullaby100% (1)
- Mental Status Examination: Table 1-6Document8 pagesMental Status Examination: Table 1-6Đức Nguyên VũNo ratings yet
- The Mental Status ExaminationDocument17 pagesThe Mental Status ExaminationperspectivebylavanyaNo ratings yet
- Mental StatusDocument6 pagesMental StatusIgor Oliveira100% (1)
- MSE1Document8 pagesMSE1Granty GarcesNo ratings yet
- Mental Status ExaminationDocument17 pagesMental Status ExaminationDharek IleshNo ratings yet
- Mental Status Examination - Bring To LectureDocument6 pagesMental Status Examination - Bring To LectureJae ChoiNo ratings yet
- Mental Status ExaminationDocument10 pagesMental Status ExaminationAljon AniesNo ratings yet
- The Mental Status ExaminationDocument15 pagesThe Mental Status ExaminationDulce RodriguezNo ratings yet
- Depersonalization ReportDocument4 pagesDepersonalization ReportLeslie Vine DelosoNo ratings yet
- Mse 1Document27 pagesMse 1Ladybelle GototosNo ratings yet
- Advance Nursing Practice Presentation On Sensory DeprivationDocument22 pagesAdvance Nursing Practice Presentation On Sensory DeprivationLaveena Aswale67% (3)
- Schizophrenia Is An Extremely Complex Mental Disorder: in Fact It Is Probably Many IllnessesDocument8 pagesSchizophrenia Is An Extremely Complex Mental Disorder: in Fact It Is Probably Many IllnessesMaloutcha InfanteNo ratings yet
- PsychoneuroticDocument5 pagesPsychoneuroticJaysonDyNo ratings yet
- Behavioral Medicine Reflection PaperDocument2 pagesBehavioral Medicine Reflection PaperDIANA THERESE MALAKINo ratings yet
- Dissociative DisordersDocument5 pagesDissociative Disorderscoke_en_canNo ratings yet
- Hypochondriasis: A Clinical Presentation byDocument10 pagesHypochondriasis: A Clinical Presentation byAmbrish KumarNo ratings yet
- Schizophrenia - Practice Essentials, Background, PathophysiologyDocument10 pagesSchizophrenia - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- Mental Status Examination (MSE)Document13 pagesMental Status Examination (MSE)Pia Mae Buaya100% (1)
- Essentials of Neurological AssessmentDocument22 pagesEssentials of Neurological AssessmentSaid UstaranNo ratings yet
- Mental Health Case StudyDocument15 pagesMental Health Case Studyapi-508142358No ratings yet
- Schizophrenia and Psychotic Disorders PPT Chap 21Document46 pagesSchizophrenia and Psychotic Disorders PPT Chap 21Claudia SanchezNo ratings yet
- Mental Status ExaminationDocument56 pagesMental Status Examinationkrishna raja100% (1)
- NPIDocument16 pagesNPIBianca de Guzman100% (1)
- Group 1 Mental Status ExaminationDocument12 pagesGroup 1 Mental Status ExaminationPankaj100% (2)
- Schizoaffective DisorderDocument7 pagesSchizoaffective DisorderIsha BhusalNo ratings yet
- Provisional DiagnosisDocument10 pagesProvisional DiagnosisVanessa DiazNo ratings yet
- Schizophrenia: Recognition and Management in The ED: FeatureDocument12 pagesSchizophrenia: Recognition and Management in The ED: FeaturemirzaNo ratings yet
- SchizophreniaDocument32 pagesSchizophreniaAnushi SinghNo ratings yet
- Functional Neurological Symptoms DisorderDocument18 pagesFunctional Neurological Symptoms DisorderWaqas Ahmed UsmaniNo ratings yet
- DeliriumDocument15 pagesDeliriumRobin gruNo ratings yet
- BC UDPD First 4 Back and FrontDocument23 pagesBC UDPD First 4 Back and FrontAPOORVA PANDEYNo ratings yet
- Human Behavior Module 7 & 8 With ActivityDocument30 pagesHuman Behavior Module 7 & 8 With ActivityAceGamingFromPhNo ratings yet
- Chapter 4 Dissociative, Somatoform and Substance Use DisordersDocument9 pagesChapter 4 Dissociative, Somatoform and Substance Use DisordersDessirie EnriquezNo ratings yet
- Schizophrenia: Recognition and Management in The EDDocument12 pagesSchizophrenia: Recognition and Management in The EDAryeh DienstagNo ratings yet
- The Mental Status ExaminationDocument16 pagesThe Mental Status Examinationeloisa.abcedeNo ratings yet
- Mental Status ExaminationDocument34 pagesMental Status Examinationkimbomd100% (2)
- Unit 4 Somatoform & Dissociative DisorderDocument12 pagesUnit 4 Somatoform & Dissociative DisorderSushant NeupaneNo ratings yet
- The Voices Within: A Journey of Living with SchizophreniaFrom EverandThe Voices Within: A Journey of Living with SchizophreniaNo ratings yet
- Finding Clarity: Empowering Patients and Families Facing Schizoaffective DisorderFrom EverandFinding Clarity: Empowering Patients and Families Facing Schizoaffective DisorderNo ratings yet
- Ocd: How to Free Yourself From Obsessive Compulsive Disorder (Comprehensive Guide to Understanding, Managing, and Overcoming Intrusive Thoughts)From EverandOcd: How to Free Yourself From Obsessive Compulsive Disorder (Comprehensive Guide to Understanding, Managing, and Overcoming Intrusive Thoughts)No ratings yet
- Pathways to Healing-100 Therapeutic Worksheets for Schizophrenia and Schizoaffective Disorders: 100 structured activities for schizophrenia HealingFrom EverandPathways to Healing-100 Therapeutic Worksheets for Schizophrenia and Schizoaffective Disorders: 100 structured activities for schizophrenia HealingNo ratings yet
- Qol CopdDocument9 pagesQol CopdElsy MayjoNo ratings yet
- WHO Health Resource Tracking Integrated PlatformDocument22 pagesWHO Health Resource Tracking Integrated PlatformElsy MayjoNo ratings yet
- Theory Analysis: Dorothy E. Johnson (Behavioral Theory) According To The Chinn and Kramer ModelDocument8 pagesTheory Analysis: Dorothy E. Johnson (Behavioral Theory) According To The Chinn and Kramer ModelElsy MayjoNo ratings yet
- Review of Literature 1 EthopiaDocument17 pagesReview of Literature 1 EthopiaElsy MayjoNo ratings yet
- SEIZURESDocument18 pagesSEIZURESElsy MayjoNo ratings yet
- Note 15 Apr 2024 (2) - 1Document14 pagesNote 15 Apr 2024 (2) - 1Elsy MayjoNo ratings yet
- Acute Coronary SyndromeDocument12 pagesAcute Coronary SyndromeElsy MayjoNo ratings yet
- CARDIAC REHABILITATION WordDocument13 pagesCARDIAC REHABILITATION WordElsy MayjoNo ratings yet
- Master Plan Shock and HemorgeDocument5 pagesMaster Plan Shock and HemorgeElsy MayjoNo ratings yet
- Lesson Plan On Personality TestDocument5 pagesLesson Plan On Personality TestElsy MayjoNo ratings yet
- Rating Scale and ChecklistDocument41 pagesRating Scale and ChecklistElsy MayjoNo ratings yet
- Socioeconomic ScaleDocument5 pagesSocioeconomic ScaleElsy MayjoNo ratings yet
- Sociometry NewDocument7 pagesSociometry NewElsy MayjoNo ratings yet
- Qi ManualDocument6 pagesQi ManualDrahbNo ratings yet
- Electrical Shock TBTDocument1 pageElectrical Shock TBTVarun PillaiNo ratings yet
- Cerebral Palsy Etiology, Evaluation, and Management of The Most Common Cause For Pediatric DisabilityDocument14 pagesCerebral Palsy Etiology, Evaluation, and Management of The Most Common Cause For Pediatric DisabilityDavid ParraNo ratings yet
- Aa ABR Abd. Ac AD A&D Ad Lib ADL Adm. Ad. Spec. A.M. or A.m., AM or Am AmbDocument4 pagesAa ABR Abd. Ac AD A&D Ad Lib ADL Adm. Ad. Spec. A.M. or A.m., AM or Am AmbMichelle MontemayorNo ratings yet
- Aesculus Horse Chestnut Materia Medica HerbsDocument3 pagesAesculus Horse Chestnut Materia Medica HerbsAlejandra Guerrero100% (1)
- Problems With The PowersDocument5 pagesProblems With The PowersAlexander Ruiz Queddeng100% (1)
- 13.24 Abdominal-InjuryDocument42 pages13.24 Abdominal-InjuryMuhammad FajarNo ratings yet
- Week#1 AphroditeDocument4 pagesWeek#1 AphroditeFrancisco Javier González GNo ratings yet
- LRSES2706VDocument88 pagesLRSES2706VFernando ZentenoNo ratings yet
- Way To English 4 Unit Seven Part of The BodyDocument2 pagesWay To English 4 Unit Seven Part of The BodyAnonymous LNyFXSMNo ratings yet
- ARC Lifeguard ManualDocument300 pagesARC Lifeguard Manualdewking1988100% (1)
- Risk Assesment of Brick & Block WorkDocument3 pagesRisk Assesment of Brick & Block WorkGyanendra SrivastavaNo ratings yet
- DangerousanimalsessayDocument3 pagesDangerousanimalsessayapi-285227884No ratings yet
- Management of Traumatic Liver Injuries: DR Junaid Ahmad SofiDocument80 pagesManagement of Traumatic Liver Injuries: DR Junaid Ahmad SofiNatalindah Jokiem Woecandra T. D.No ratings yet
- A Strength & Conditioning Program For Developing Young AthletesDocument51 pagesA Strength & Conditioning Program For Developing Young AthletesAlNo ratings yet
- Wounds by Shotguns: by Dilnaaz Baig Roll No-8 Batch 2015 Ii MbbsDocument13 pagesWounds by Shotguns: by Dilnaaz Baig Roll No-8 Batch 2015 Ii Mbbsniraj_sdNo ratings yet
- KAJAL NARUTO Sasuke LinaDocument32 pagesKAJAL NARUTO Sasuke Linasanjay tamangNo ratings yet
- Head InjuryDocument26 pagesHead InjuryPriyanka Narwal100% (1)
- Asana Guide: Pose NameDocument69 pagesAsana Guide: Pose NamedriNo ratings yet
- Aspects-of-Homeopathy-Ian-Watson.07907 - 2therapeutic Index PDFDocument4 pagesAspects-of-Homeopathy-Ian-Watson.07907 - 2therapeutic Index PDFSohail Latif0% (1)
- Ramplissage Ram ChidambaramDocument6 pagesRamplissage Ram ChidambaramProsenjit BhowalNo ratings yet
- Paul Roetert - Todd S Ellenbecker - United States Tennis AssocDocument214 pagesPaul Roetert - Todd S Ellenbecker - United States Tennis AssocliougkosNo ratings yet
- TN42.1005 - Procedure Checking EndPlay in Ball Bearing PDFDocument2 pagesTN42.1005 - Procedure Checking EndPlay in Ball Bearing PDFarifuddinnurdinNo ratings yet
- Seance Reathle Entorse GenouDocument4 pagesSeance Reathle Entorse GenouCatalin EneNo ratings yet
- Manual For OSHADocument62 pagesManual For OSHAEduardson Justo100% (1)
- Duty Report: Annisa Ayu Rahmawati Nazza Rizky RamdhagamaDocument12 pagesDuty Report: Annisa Ayu Rahmawati Nazza Rizky RamdhagamasasoyNo ratings yet