
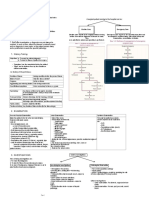
Ulcer HX & PEx
Ulcer HX & PEx
You might also like
- Behind The Knife ABSITE Podcast CompanionDocument270 pagesBehind The Knife ABSITE Podcast CompanionMuhammad Zeeshan88% (33)
- Doctor's Order & Lab ResultsDocument4 pagesDoctor's Order & Lab ResultsKaloy Kamao100% (1)
- General Surgery IntroductionDocument1 pageGeneral Surgery IntroductionAndrew BonusNo ratings yet
- MSK LECTURE 1-1Document53 pagesMSK LECTURE 1-1seemabfarwauaeNo ratings yet
- Pain 1 PDFDocument37 pagesPain 1 PDFSamwel EmadNo ratings yet
- Examination of Head and Neck SwellingsDocument22 pagesExamination of Head and Neck SwellingsObehi EromoseleNo ratings yet
- Pressure UlcersDocument43 pagesPressure UlcersZubda Butt100% (2)
- The Sensory System and Pain Syndromes: VTH Year, Dentistry, 30.09.2008 Department of Neurology Semmelweis UniversityDocument53 pagesThe Sensory System and Pain Syndromes: VTH Year, Dentistry, 30.09.2008 Department of Neurology Semmelweis Universitymonica ortizNo ratings yet
- SarcoidosisDocument17 pagesSarcoidosisapi-678326591No ratings yet
- Diabetic FootDocument37 pagesDiabetic FootSeleno GlauberNo ratings yet
- Decubitus Ulcer: Presenters: Angod, Lady Aizahlyn I. Apat, Joselle Janina F. Araune, Trixie Mariel EDocument32 pagesDecubitus Ulcer: Presenters: Angod, Lady Aizahlyn I. Apat, Joselle Janina F. Araune, Trixie Mariel EXaxa AngodNo ratings yet
- 4.penyembuhan LukaDocument52 pages4.penyembuhan LukaFajar Satria Rahmaditya100% (1)
- Rheumatoid HandDocument67 pagesRheumatoid HandSayantika DharNo ratings yet
- Bed Sore 48Document45 pagesBed Sore 48Sedaka DonaldsonNo ratings yet
- Rheumatic and Granulomatous Diseases: By:LeañoDocument3 pagesRheumatic and Granulomatous Diseases: By:LeañoTJ OberioNo ratings yet
- Snake Bite - FaishalDocument12 pagesSnake Bite - FaishalYaya UtamiNo ratings yet
- Approach To Joint Pain (October 2022)Document56 pagesApproach To Joint Pain (October 2022)imranmohammad968No ratings yet
- Examination of Ulcer, Sinus & FistulaDocument8 pagesExamination of Ulcer, Sinus & FistulaManas RanjanNo ratings yet
- Diagnosis Penyakit Kulit: PraharsiniDocument25 pagesDiagnosis Penyakit Kulit: PraharsiniKrishna PriyakaNo ratings yet
- Diagnosis Penyakit Kulit: PraharsiniDocument25 pagesDiagnosis Penyakit Kulit: PraharsiniSheryl ElitaNo ratings yet
- Matary Cases - 2013 (WWW - Afriqa Sat - Com)Document154 pagesMatary Cases - 2013 (WWW - Afriqa Sat - Com)Ahmed AttiaNo ratings yet
- DR Mohit Gulati (PT)Document62 pagesDR Mohit Gulati (PT)Shubha DiwakarNo ratings yet
- Cutaneous Ulcers HFHDocument52 pagesCutaneous Ulcers HFHEmmanuel Papa AcquahNo ratings yet
- Wound Care Management 1Document99 pagesWound Care Management 1Jan Oliver YaresNo ratings yet
- Examination of Ulcer PDFDocument2 pagesExamination of Ulcer PDFHadid AliNo ratings yet
- MCN Rheumatic FeverDocument1 pageMCN Rheumatic FeverBSN 1-N CASTRO, RicciNo ratings yet
- NSTP ReviewerDocument4 pagesNSTP ReviewerTrexy NorialNo ratings yet
- General Surgery (Revision)Document78 pagesGeneral Surgery (Revision)AmrAsser KhattabNo ratings yet
- Tugas Kelompok Ii Askep Systemic Lupus Erythematosus (SLE) Anggota KelompokDocument37 pagesTugas Kelompok Ii Askep Systemic Lupus Erythematosus (SLE) Anggota KelompokRizka Nada AudivaNo ratings yet
- 4.penyembuhan LukaDocument52 pages4.penyembuhan LukaazisaaidrNo ratings yet
- Approach To Bone MalignancyDocument38 pagesApproach To Bone MalignancyAna S.NazrulNo ratings yet
- Fractures and Dislocation: ArnadiDocument30 pagesFractures and Dislocation: ArnadiNizai Rama DeswiraNo ratings yet
- Chapter 1Document6 pagesChapter 1Greely Mae GumunotNo ratings yet
- SheetDocument10 pagesSheetsushmakar pNo ratings yet
- Superficial Swellings (Final Draft) - 2Document12 pagesSuperficial Swellings (Final Draft) - 2jqgjwgnnwkNo ratings yet
- Complex Wounds 2020Document38 pagesComplex Wounds 2020Ài ZìjǐNo ratings yet
- Vetero-Legal WoundsDocument26 pagesVetero-Legal WoundsAhmadx Hassan100% (4)
- Section Slides 2Document52 pagesSection Slides 2drsafwatismailNo ratings yet
- Surgery RevisionDocument158 pagesSurgery RevisionDr-Irfan HabibNo ratings yet
- 8 PACES CasesDocument14 pages8 PACES CasesManisanthosh KumarNo ratings yet
- Herpes Zoster: Bing-Rong ZHOUDocument43 pagesHerpes Zoster: Bing-Rong ZHOUMichael Jansen Sulaiman100% (1)
- Mod 7 & 8 Study GuidesDocument11 pagesMod 7 & 8 Study GuidesFerd RuizNo ratings yet
- Osteomyelitis - Kaye WilkinsDocument50 pagesOsteomyelitis - Kaye WilkinsWindy MentariNo ratings yet
- 14 - Bone Tumors (Ubdated)Document23 pages14 - Bone Tumors (Ubdated)khalifasweadNo ratings yet
- Osteomyelitis: Pediatric Surgery Department Andreev D.ADocument83 pagesOsteomyelitis: Pediatric Surgery Department Andreev D.AlimeddyNo ratings yet
- D.D of Oral Ulcers PDFDocument64 pagesD.D of Oral Ulcers PDFmohamedtolan9000No ratings yet
- 1 Scenario: Group 14Document48 pages1 Scenario: Group 14Alvi Kamal FikriNo ratings yet
- Lecture TextDocument25 pagesLecture TextruchikaNo ratings yet
- PemicuDocument34 pagesPemicuCindy SugandaNo ratings yet
- Osteosarcoma & Ewin's SarcomaDocument34 pagesOsteosarcoma & Ewin's SarcomaAbdulMushibNo ratings yet
- Osteomyelitis - Kaye WilkinsDocument50 pagesOsteomyelitis - Kaye WilkinsWindy MentariNo ratings yet
- EPISTAXISDocument2 pagesEPISTAXISRUTH RosilinNo ratings yet
- OSCE EverythingDocument24 pagesOSCE EverythingkendymillNo ratings yet
- History TakingDocument130 pagesHistory Takingvwpwh86gfhNo ratings yet
- SYRINGOMYELIADocument31 pagesSYRINGOMYELIAPreeti SharmaNo ratings yet
- Diagnostics II - Class 1Document8 pagesDiagnostics II - Class 1محمد محمود الأنصاريNo ratings yet
- OsteomyelitisDocument52 pagesOsteomyelitisaggieedwin3No ratings yet
- Degenerative Joint Prof AngelaDocument87 pagesDegenerative Joint Prof AngelaPatrick MuljonoNo ratings yet
- Complications of FractureDocument19 pagesComplications of FractureEsome Sharma100% (1)
- How To Evaluate A Case of LeprosyDocument35 pagesHow To Evaluate A Case of LeprosyBarath Kumar SinghNo ratings yet
- Common CasesDocument44 pagesCommon CasesRebecca WongNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Emilok Marketing Plan 2017Document38 pagesEmilok Marketing Plan 2017maawi2002yahoocomNo ratings yet
- Vincenta Review IJNDDocument21 pagesVincenta Review IJNDDimahya chanelNo ratings yet
- # Davidson - Review # GastroenterologyDocument30 pages# Davidson - Review # Gastroenterologyemtiaz zamanNo ratings yet
- Pentagastrin TestDocument13 pagesPentagastrin TestMustafa KhandgawiNo ratings yet
- Food Peptic Ulcer DietDocument2 pagesFood Peptic Ulcer Dietammaramaryam6463No ratings yet
- Peptic Ulcer DiseaseDocument18 pagesPeptic Ulcer DiseasechetankumarbhumireddyNo ratings yet
- Momentact: 400 MG Fi Lm-Coated TabletsDocument4 pagesMomentact: 400 MG Fi Lm-Coated TabletsRaja HashimNo ratings yet
- Contoh CJRDocument16 pagesContoh CJRmmerry743No ratings yet
- 2nd Year PracticalDocument7 pages2nd Year PracticalRAMZAAN EDUCATIONNo ratings yet
- Nto Uchenna Note On GI SecretionsDocument10 pagesNto Uchenna Note On GI SecretionsNwaoha Chibuzor AnthonyNo ratings yet
- 2000 - GI - Endo InterpretationDocument19 pages2000 - GI - Endo InterpretationambaNo ratings yet
- Stomach-Esophagus MedCosmos Surgery - MCQDocument39 pagesStomach-Esophagus MedCosmos Surgery - MCQMike G100% (1)
- AmlapittaDocument4 pagesAmlapittaSupriya Abhijit PhadkeNo ratings yet
- Rofecoxib Inhibits Heterotopic Ossification AfterDocument146 pagesRofecoxib Inhibits Heterotopic Ossification AfterHaqqi IslamiNo ratings yet
- 50 Item Gastrointestinal Health Problems Test DrillDocument14 pages50 Item Gastrointestinal Health Problems Test DrillFilipino Nurses Central100% (2)
- PG Thesis in MedicineDocument5 pagesPG Thesis in Medicinewbeqtpmef100% (1)
- A Comparison of Efficacy Between Rebamipide and Omeprazole in The Treatment of Nsaids GastropathyDocument6 pagesA Comparison of Efficacy Between Rebamipide and Omeprazole in The Treatment of Nsaids GastropathyNurulAlviFauzianaNo ratings yet
- (INS-SA-EN) Ichroma H.pylori SA - Rev02 - 180710Document3 pages(INS-SA-EN) Ichroma H.pylori SA - Rev02 - 180710nam7124119No ratings yet
- Complementary Therapies in Clinical PracticeDocument7 pagesComplementary Therapies in Clinical PracticeChetan AmberkarNo ratings yet
- Aspirin Drug StudyDocument2 pagesAspirin Drug StudyEdelweiss Marie CayetanoNo ratings yet
- Gastritis - Etiology and Diagnosis - UpToDateDocument10 pagesGastritis - Etiology and Diagnosis - UpToDateLizbeth Navarrete SierraNo ratings yet
- KNH 413 - Case Study 14Document17 pagesKNH 413 - Case Study 14api-301118772No ratings yet
- Intestinal Perforation: BackgroundDocument5 pagesIntestinal Perforation: BackgroundpricillyaNo ratings yet
- Dr. Nurhasanah, SP - Gk-Terapi Gizi Pada Gangguan Saluran CernaDocument49 pagesDr. Nurhasanah, SP - Gk-Terapi Gizi Pada Gangguan Saluran Cernaaditya fikri auliaNo ratings yet
- BACTE-LEC-FINALS-1 DraftDocument15 pagesBACTE-LEC-FINALS-1 DraftJaneNo ratings yet
- Histamine and Antihistamines: Learning ObjectivesDocument6 pagesHistamine and Antihistamines: Learning ObjectivesaNo ratings yet
- The Nursing Assessment of Peptic UlcerDocument14 pagesThe Nursing Assessment of Peptic UlcerVelia suwandiNo ratings yet
- 106 Finals Reviewer Quizlet and NurselabsDocument62 pages106 Finals Reviewer Quizlet and NurselabsCreciabullecerNo ratings yet
























































































Download as pdf or txt
You might also like
- Behind The Knife ABSITE Podcast CompanionDocument270 pagesBehind The Knife ABSITE Podcast CompanionMuhammad Zeeshan88% (33)
- Doctor's Order & Lab ResultsDocument4 pagesDoctor's Order & Lab ResultsKaloy Kamao100% (1)
- General Surgery IntroductionDocument1 pageGeneral Surgery IntroductionAndrew BonusNo ratings yet
- MSK LECTURE 1-1Document53 pagesMSK LECTURE 1-1seemabfarwauaeNo ratings yet
- Pain 1 PDFDocument37 pagesPain 1 PDFSamwel EmadNo ratings yet
- Examination of Head and Neck SwellingsDocument22 pagesExamination of Head and Neck SwellingsObehi EromoseleNo ratings yet
- Pressure UlcersDocument43 pagesPressure UlcersZubda Butt100% (2)
- The Sensory System and Pain Syndromes: VTH Year, Dentistry, 30.09.2008 Department of Neurology Semmelweis UniversityDocument53 pagesThe Sensory System and Pain Syndromes: VTH Year, Dentistry, 30.09.2008 Department of Neurology Semmelweis Universitymonica ortizNo ratings yet
- SarcoidosisDocument17 pagesSarcoidosisapi-678326591No ratings yet
- Diabetic FootDocument37 pagesDiabetic FootSeleno GlauberNo ratings yet
- Decubitus Ulcer: Presenters: Angod, Lady Aizahlyn I. Apat, Joselle Janina F. Araune, Trixie Mariel EDocument32 pagesDecubitus Ulcer: Presenters: Angod, Lady Aizahlyn I. Apat, Joselle Janina F. Araune, Trixie Mariel EXaxa AngodNo ratings yet
- 4.penyembuhan LukaDocument52 pages4.penyembuhan LukaFajar Satria Rahmaditya100% (1)
- Rheumatoid HandDocument67 pagesRheumatoid HandSayantika DharNo ratings yet
- Bed Sore 48Document45 pagesBed Sore 48Sedaka DonaldsonNo ratings yet
- Rheumatic and Granulomatous Diseases: By:LeañoDocument3 pagesRheumatic and Granulomatous Diseases: By:LeañoTJ OberioNo ratings yet
- Snake Bite - FaishalDocument12 pagesSnake Bite - FaishalYaya UtamiNo ratings yet
- Approach To Joint Pain (October 2022)Document56 pagesApproach To Joint Pain (October 2022)imranmohammad968No ratings yet
- Examination of Ulcer, Sinus & FistulaDocument8 pagesExamination of Ulcer, Sinus & FistulaManas RanjanNo ratings yet
- Diagnosis Penyakit Kulit: PraharsiniDocument25 pagesDiagnosis Penyakit Kulit: PraharsiniKrishna PriyakaNo ratings yet
- Diagnosis Penyakit Kulit: PraharsiniDocument25 pagesDiagnosis Penyakit Kulit: PraharsiniSheryl ElitaNo ratings yet
- Matary Cases - 2013 (WWW - Afriqa Sat - Com)Document154 pagesMatary Cases - 2013 (WWW - Afriqa Sat - Com)Ahmed AttiaNo ratings yet
- DR Mohit Gulati (PT)Document62 pagesDR Mohit Gulati (PT)Shubha DiwakarNo ratings yet
- Cutaneous Ulcers HFHDocument52 pagesCutaneous Ulcers HFHEmmanuel Papa AcquahNo ratings yet
- Wound Care Management 1Document99 pagesWound Care Management 1Jan Oliver YaresNo ratings yet
- Examination of Ulcer PDFDocument2 pagesExamination of Ulcer PDFHadid AliNo ratings yet
- MCN Rheumatic FeverDocument1 pageMCN Rheumatic FeverBSN 1-N CASTRO, RicciNo ratings yet
- NSTP ReviewerDocument4 pagesNSTP ReviewerTrexy NorialNo ratings yet
- General Surgery (Revision)Document78 pagesGeneral Surgery (Revision)AmrAsser KhattabNo ratings yet
- Tugas Kelompok Ii Askep Systemic Lupus Erythematosus (SLE) Anggota KelompokDocument37 pagesTugas Kelompok Ii Askep Systemic Lupus Erythematosus (SLE) Anggota KelompokRizka Nada AudivaNo ratings yet
- 4.penyembuhan LukaDocument52 pages4.penyembuhan LukaazisaaidrNo ratings yet
- Approach To Bone MalignancyDocument38 pagesApproach To Bone MalignancyAna S.NazrulNo ratings yet
- Fractures and Dislocation: ArnadiDocument30 pagesFractures and Dislocation: ArnadiNizai Rama DeswiraNo ratings yet
- Chapter 1Document6 pagesChapter 1Greely Mae GumunotNo ratings yet
- SheetDocument10 pagesSheetsushmakar pNo ratings yet
- Superficial Swellings (Final Draft) - 2Document12 pagesSuperficial Swellings (Final Draft) - 2jqgjwgnnwkNo ratings yet
- Complex Wounds 2020Document38 pagesComplex Wounds 2020Ài ZìjǐNo ratings yet
- Vetero-Legal WoundsDocument26 pagesVetero-Legal WoundsAhmadx Hassan100% (4)
- Section Slides 2Document52 pagesSection Slides 2drsafwatismailNo ratings yet
- Surgery RevisionDocument158 pagesSurgery RevisionDr-Irfan HabibNo ratings yet
- 8 PACES CasesDocument14 pages8 PACES CasesManisanthosh KumarNo ratings yet
- Herpes Zoster: Bing-Rong ZHOUDocument43 pagesHerpes Zoster: Bing-Rong ZHOUMichael Jansen Sulaiman100% (1)
- Mod 7 & 8 Study GuidesDocument11 pagesMod 7 & 8 Study GuidesFerd RuizNo ratings yet
- Osteomyelitis - Kaye WilkinsDocument50 pagesOsteomyelitis - Kaye WilkinsWindy MentariNo ratings yet
- 14 - Bone Tumors (Ubdated)Document23 pages14 - Bone Tumors (Ubdated)khalifasweadNo ratings yet
- Osteomyelitis: Pediatric Surgery Department Andreev D.ADocument83 pagesOsteomyelitis: Pediatric Surgery Department Andreev D.AlimeddyNo ratings yet
- D.D of Oral Ulcers PDFDocument64 pagesD.D of Oral Ulcers PDFmohamedtolan9000No ratings yet
- 1 Scenario: Group 14Document48 pages1 Scenario: Group 14Alvi Kamal FikriNo ratings yet
- Lecture TextDocument25 pagesLecture TextruchikaNo ratings yet
- PemicuDocument34 pagesPemicuCindy SugandaNo ratings yet
- Osteosarcoma & Ewin's SarcomaDocument34 pagesOsteosarcoma & Ewin's SarcomaAbdulMushibNo ratings yet
- Osteomyelitis - Kaye WilkinsDocument50 pagesOsteomyelitis - Kaye WilkinsWindy MentariNo ratings yet
- EPISTAXISDocument2 pagesEPISTAXISRUTH RosilinNo ratings yet
- OSCE EverythingDocument24 pagesOSCE EverythingkendymillNo ratings yet
- History TakingDocument130 pagesHistory Takingvwpwh86gfhNo ratings yet
- SYRINGOMYELIADocument31 pagesSYRINGOMYELIAPreeti SharmaNo ratings yet
- Diagnostics II - Class 1Document8 pagesDiagnostics II - Class 1محمد محمود الأنصاريNo ratings yet
- OsteomyelitisDocument52 pagesOsteomyelitisaggieedwin3No ratings yet
- Degenerative Joint Prof AngelaDocument87 pagesDegenerative Joint Prof AngelaPatrick MuljonoNo ratings yet
- Complications of FractureDocument19 pagesComplications of FractureEsome Sharma100% (1)
- How To Evaluate A Case of LeprosyDocument35 pagesHow To Evaluate A Case of LeprosyBarath Kumar SinghNo ratings yet
- Common CasesDocument44 pagesCommon CasesRebecca WongNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Emilok Marketing Plan 2017Document38 pagesEmilok Marketing Plan 2017maawi2002yahoocomNo ratings yet
- Vincenta Review IJNDDocument21 pagesVincenta Review IJNDDimahya chanelNo ratings yet
- # Davidson - Review # GastroenterologyDocument30 pages# Davidson - Review # Gastroenterologyemtiaz zamanNo ratings yet
- Pentagastrin TestDocument13 pagesPentagastrin TestMustafa KhandgawiNo ratings yet
- Food Peptic Ulcer DietDocument2 pagesFood Peptic Ulcer Dietammaramaryam6463No ratings yet
- Peptic Ulcer DiseaseDocument18 pagesPeptic Ulcer DiseasechetankumarbhumireddyNo ratings yet
- Momentact: 400 MG Fi Lm-Coated TabletsDocument4 pagesMomentact: 400 MG Fi Lm-Coated TabletsRaja HashimNo ratings yet
- Contoh CJRDocument16 pagesContoh CJRmmerry743No ratings yet
- 2nd Year PracticalDocument7 pages2nd Year PracticalRAMZAAN EDUCATIONNo ratings yet
- Nto Uchenna Note On GI SecretionsDocument10 pagesNto Uchenna Note On GI SecretionsNwaoha Chibuzor AnthonyNo ratings yet
- 2000 - GI - Endo InterpretationDocument19 pages2000 - GI - Endo InterpretationambaNo ratings yet
- Stomach-Esophagus MedCosmos Surgery - MCQDocument39 pagesStomach-Esophagus MedCosmos Surgery - MCQMike G100% (1)
- AmlapittaDocument4 pagesAmlapittaSupriya Abhijit PhadkeNo ratings yet
- Rofecoxib Inhibits Heterotopic Ossification AfterDocument146 pagesRofecoxib Inhibits Heterotopic Ossification AfterHaqqi IslamiNo ratings yet
- 50 Item Gastrointestinal Health Problems Test DrillDocument14 pages50 Item Gastrointestinal Health Problems Test DrillFilipino Nurses Central100% (2)
- PG Thesis in MedicineDocument5 pagesPG Thesis in Medicinewbeqtpmef100% (1)
- A Comparison of Efficacy Between Rebamipide and Omeprazole in The Treatment of Nsaids GastropathyDocument6 pagesA Comparison of Efficacy Between Rebamipide and Omeprazole in The Treatment of Nsaids GastropathyNurulAlviFauzianaNo ratings yet
- (INS-SA-EN) Ichroma H.pylori SA - Rev02 - 180710Document3 pages(INS-SA-EN) Ichroma H.pylori SA - Rev02 - 180710nam7124119No ratings yet
- Complementary Therapies in Clinical PracticeDocument7 pagesComplementary Therapies in Clinical PracticeChetan AmberkarNo ratings yet
- Aspirin Drug StudyDocument2 pagesAspirin Drug StudyEdelweiss Marie CayetanoNo ratings yet
- Gastritis - Etiology and Diagnosis - UpToDateDocument10 pagesGastritis - Etiology and Diagnosis - UpToDateLizbeth Navarrete SierraNo ratings yet
- KNH 413 - Case Study 14Document17 pagesKNH 413 - Case Study 14api-301118772No ratings yet
- Intestinal Perforation: BackgroundDocument5 pagesIntestinal Perforation: BackgroundpricillyaNo ratings yet
- Dr. Nurhasanah, SP - Gk-Terapi Gizi Pada Gangguan Saluran CernaDocument49 pagesDr. Nurhasanah, SP - Gk-Terapi Gizi Pada Gangguan Saluran Cernaaditya fikri auliaNo ratings yet
- BACTE-LEC-FINALS-1 DraftDocument15 pagesBACTE-LEC-FINALS-1 DraftJaneNo ratings yet
- Histamine and Antihistamines: Learning ObjectivesDocument6 pagesHistamine and Antihistamines: Learning ObjectivesaNo ratings yet
- The Nursing Assessment of Peptic UlcerDocument14 pagesThe Nursing Assessment of Peptic UlcerVelia suwandiNo ratings yet
- 106 Finals Reviewer Quizlet and NurselabsDocument62 pages106 Finals Reviewer Quizlet and NurselabsCreciabullecerNo ratings yet