Download as docx, pdf, or txt
You might also like
- Letterhead Hospital MiriDocument9 pagesLetterhead Hospital MiriShahir HassanNo ratings yet
- 101 Chest X Ray Solutions 2013Document281 pages101 Chest X Ray Solutions 2013Mohamed Saeed El Khayat100% (4)
- Cme DianaDocument17 pagesCme DianaChris Tine ChiaNo ratings yet
- Mapping Digest 3 Maret 2014Document3 pagesMapping Digest 3 Maret 2014rakanootousanNo ratings yet
- Discharge Summary Patient's ProfilesDocument5 pagesDischarge Summary Patient's ProfilesAnonymous nSGpLONo ratings yet
- Koran Bedah Thoraks Kardiovaskular RABU, 23 OKTOBER 2013: Palem BawahDocument13 pagesKoran Bedah Thoraks Kardiovaskular RABU, 23 OKTOBER 2013: Palem BawahMuhammad Azhari AirlanggaNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document6 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Resha DermawanNo ratings yet
- Koran Bedah Thoraks Kardiovaskular Jumat, 6 September 2013Document8 pagesKoran Bedah Thoraks Kardiovaskular Jumat, 6 September 2013Ridski D. MiruNo ratings yet
- Follow Up Mauladi KADDocument9 pagesFollow Up Mauladi KADhotasioclsNo ratings yet
- Mapping Aqsha 3 Senin, 14 Maret 2022Document3 pagesMapping Aqsha 3 Senin, 14 Maret 2022Satrya DitaNo ratings yet
- No Identitas Anamnesa Pemeriksaan Pemeriksaanpenunja NG: Pasien Bona 2 RespiroDocument13 pagesNo Identitas Anamnesa Pemeriksaan Pemeriksaanpenunja NG: Pasien Bona 2 RespiroMeta Hanindita NugrohoNo ratings yet
- Mapping GH Raber Kamis 1-9-2022Document11 pagesMapping GH Raber Kamis 1-9-2022McShadiq ZikryNo ratings yet
- Fu 060423Document15 pagesFu 060423tiffanyalmndNo ratings yet
- Patient Summary (A Case of Thyroid Storm) : by DR Adeyemo H.ADocument17 pagesPatient Summary (A Case of Thyroid Storm) : by DR Adeyemo H.AAdeyemoNo ratings yet
- Koran Digestiv (MEYKE - PCC) Kamis, 20 Maret 2014Document15 pagesKoran Digestiv (MEYKE - PCC) Kamis, 20 Maret 2014Dwi Arnhilah MirandaNo ratings yet
- Mortality Meet 26-7-19Document38 pagesMortality Meet 26-7-19JYOTI AGGARWALNo ratings yet
- KoranDocument1 pageKoranAgus EndrawantoNo ratings yet
- 2 Nov 2015 OnkologyDocument1 page2 Nov 2015 OnkologyzicoparadigmaNo ratings yet
- Sept 4, 2015Document8 pagesSept 4, 2015Deity CelleNo ratings yet
- Morbidity Meeting CT Icu (1) (1) - 2 3Document33 pagesMorbidity Meeting CT Icu (1) (1) - 2 3evaNo ratings yet
- Case Presentation On Systemic Lupus Erythematosus (SLE) : Presented By: Mahitha Karimsetti 616175802018 Pharm. D InternDocument35 pagesCase Presentation On Systemic Lupus Erythematosus (SLE) : Presented By: Mahitha Karimsetti 616175802018 Pharm. D Internsrija vijjapuNo ratings yet
- Internal Medicine Case PresentationDocument114 pagesInternal Medicine Case PresentationAyen FornollesNo ratings yet
- Laporan Harian TGL 4 Agustus 2015Document7 pagesLaporan Harian TGL 4 Agustus 2015ajescoolNo ratings yet
- List Pasien Divisi Onkologi29desDocument6 pagesList Pasien Divisi Onkologi29desDedy SupriadiNo ratings yet
- Pasien Raber Per TGL 10 November 2023 FKDocument5 pagesPasien Raber Per TGL 10 November 2023 FKmasitha yusmarNo ratings yet
- Koran Bedah Thoraks Kardiovaskular JUM'AT, 18 OKTOBER 2013: NO Ruangan Identitas & Diagnosis Hasil Pemeriksaan PenunjangDocument23 pagesKoran Bedah Thoraks Kardiovaskular JUM'AT, 18 OKTOBER 2013: NO Ruangan Identitas & Diagnosis Hasil Pemeriksaan PenunjangRennyAnggrainyNo ratings yet
- Koran Bedah Digestif, Jumat 28 Maret 2014: N o Bed Identitas Diagnosis Pemeriksaan Penunjang Terap I Lab 17/03/2014Document17 pagesKoran Bedah Digestif, Jumat 28 Maret 2014: N o Bed Identitas Diagnosis Pemeriksaan Penunjang Terap I Lab 17/03/2014fateeeNo ratings yet
- Ruang/Bed Identitas Pasien Diagnosis Hasil Pemeriksaan Terapi Darah RutinDocument17 pagesRuang/Bed Identitas Pasien Diagnosis Hasil Pemeriksaan Terapi Darah RutinBaskara HutahaeanNo ratings yet
- Mapping Aqsha 3 Senin, 08 November 2021Document10 pagesMapping Aqsha 3 Senin, 08 November 2021Febbby Mutia SafiraNo ratings yet
- Koran Bedah Plastik Senin 27 MayDocument5 pagesKoran Bedah Plastik Senin 27 MayChristophore SantosoNo ratings yet
- Koran Digestive Senin, 17 Mar 14 PALEMDocument12 pagesKoran Digestive Senin, 17 Mar 14 PALEMSigit Dwi PramonoNo ratings yet
- Decompensated Liver DX A Presenentation by Seyram LetsaDocument65 pagesDecompensated Liver DX A Presenentation by Seyram LetsaArahime Hitsugaya HatakeNo ratings yet
- Pedia NotesDocument4 pagesPedia NotesDana CastroNo ratings yet
- Follow Up Pasien Di Burn Unit: Objektif TGL 27 September 2015 (05.00) Perkembangan 26.9.2015 MasalahDocument4 pagesFollow Up Pasien Di Burn Unit: Objektif TGL 27 September 2015 (05.00) Perkembangan 26.9.2015 MasalahYovan PrakosaNo ratings yet
- Digest Mapping 2 JanDocument3 pagesDigest Mapping 2 JanAdi RiyadliNo ratings yet
- Cert Exam2018 Case StudyDocument5 pagesCert Exam2018 Case StudyRyan-Jay AbolenciaNo ratings yet
- Problem Case: DR Bakhtawar Chandio Unit 1Document34 pagesProblem Case: DR Bakhtawar Chandio Unit 1Aijaz TalaniNo ratings yet
- Amprahan PICU Jumat Sore, 26 April 2024Document13 pagesAmprahan PICU Jumat Sore, 26 April 2024alfaz zamzamiNo ratings yet
- AQSHA 2, Senin, 19 Juli 2021Document8 pagesAQSHA 2, Senin, 19 Juli 2021Dezha DetiroNo ratings yet
- List Pasien Divisi Onkologi 18 Oktober 2015Document9 pagesList Pasien Divisi Onkologi 18 Oktober 2015Denny'deden'TrisnaamijayaNo ratings yet
- WK Highorder PXDocument39 pagesWK Highorder PXwende kassahunNo ratings yet
- 4amapping 9 Okt 2018Document6 pages4amapping 9 Okt 2018Kaca NegaraNo ratings yet
- RUKMINADocument5 pagesRUKMINAaprajitaguptaNo ratings yet
- Case Based Discussion ObstetricDocument6 pagesCase Based Discussion Obstetriclim sjNo ratings yet
- Wkcase FINAL PresentationDocument51 pagesWkcase FINAL Presentationwende kassahunNo ratings yet
- Amprahan HCU Kamis Pagi, 15 Februari 2024Document6 pagesAmprahan HCU Kamis Pagi, 15 Februari 2024alfaz zamzamiNo ratings yet
- Koran - B.saraf Senin 10 Juni 2013Document1 pageKoran - B.saraf Senin 10 Juni 2013Jhonn NaiseNo ratings yet
- MM Conference 3 FinalDocument41 pagesMM Conference 3 FinalNachchakorn DellNo ratings yet
- Koran Rabu 4 JUNI 2014Document10 pagesKoran Rabu 4 JUNI 2014Muhamad Zubair Muhamad NohNo ratings yet
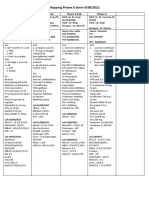
- Mapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Document2 pagesMapping Pinere 6 Senin 9/08/2021: Pinere 6 K4I Pinere 6 K3A Pinere 6 K1A Pinere 6Rina SyafritaNo ratings yet
- Post Partum DeathDocument12 pagesPost Partum DeathFerzada SajiranNo ratings yet
- Mapping New Aqsa 3 Sabtu 23 Oktober 2021Document6 pagesMapping New Aqsa 3 Sabtu 23 Oktober 2021Muhammed GhaziNo ratings yet
- Managing Covid-19 in IcuDocument77 pagesManaging Covid-19 in IcuninishahirahNo ratings yet
- Sumiarti, 41 Y.o, FW 12Document7 pagesSumiarti, 41 Y.o, FW 12Rangga LunesiaNo ratings yet
- Amprahan HCU Minggu Pagi, 18 Februari 2024Document8 pagesAmprahan HCU Minggu Pagi, 18 Februari 2024alfaz zamzamiNo ratings yet
- 20 JuniDocument2 pages20 JuniJati NugrohoNo ratings yet
- Mortality conference: ߡⰊשʑⅶⷪず कẤⵒ Reporter: CR⨀ᆙ Supervisor: CVS ⫯⸉Document42 pagesMortality conference: ߡⰊשʑⅶⷪず कẤⵒ Reporter: CR⨀ᆙ Supervisor: CVS ⫯⸉劉彩屏No ratings yet
- Case PresentationDocument40 pagesCase PresentationLaxman Lucky'sNo ratings yet
- Rekap Pasien Bedah Digestive 5 Juli 2015 Jeumpa 1Document6 pagesRekap Pasien Bedah Digestive 5 Juli 2015 Jeumpa 1achciaNo ratings yet
- Summary of Data Base: Male/ 41yo/w.25Document24 pagesSummary of Data Base: Male/ 41yo/w.25Anonymous vUEDx8No ratings yet
- Fast Facts: Treatment-Free Remission in Chronic Myeloid Leukemia: From concept to practice and beyondFrom EverandFast Facts: Treatment-Free Remission in Chronic Myeloid Leukemia: From concept to practice and beyondNo ratings yet
- Labortory Test or ManeuverDocument2 pagesLabortory Test or ManeuverJeno Luis J. ACUBNo ratings yet
- Congenital Lung MalformationsDocument115 pagesCongenital Lung MalformationsAhmad Abu KushNo ratings yet
- Pneumonia Management ProtocolDocument2 pagesPneumonia Management Protocolsky nuts100% (1)
- Blunt Thoracic Trauma - Role of Chest Radiography and Comparison With CT - Fndings and Literature ReviewDocument13 pagesBlunt Thoracic Trauma - Role of Chest Radiography and Comparison With CT - Fndings and Literature Revieworalposter PIPKRA2023No ratings yet
- A Rare Cause of Chest Pain: Spontaneous Sternum Fracture: Ibrahim Sarbay, Halil DoganDocument5 pagesA Rare Cause of Chest Pain: Spontaneous Sternum Fracture: Ibrahim Sarbay, Halil DoganYuliSsTiaNo ratings yet
- Pemeriksaan Foto Thorax Pada Anak-AnakDocument29 pagesPemeriksaan Foto Thorax Pada Anak-AnakRenaldy PamungkasNo ratings yet
- Lung Tumor Localization and Visualization in ChestDocument17 pagesLung Tumor Localization and Visualization in ChestAida Fitriyane HamdaniNo ratings yet
- Comparison of Chest X-Ray Findings Between Primary and Secondary Multidrug Resistant Pulmonary TuberculosisDocument8 pagesComparison of Chest X-Ray Findings Between Primary and Secondary Multidrug Resistant Pulmonary TuberculosismahyaNo ratings yet
- Toaz - Info Radiology Fmge PRDocument19 pagesToaz - Info Radiology Fmge PRAditya Raj100% (2)
- Choose Only One Best AnswerDocument10 pagesChoose Only One Best AnswerMuhammad Farrukh ul Islam100% (1)
- Chest Radiography in Thoracic Polytrauma: Mai-Lan Ho Fernando R. GutierrezDocument14 pagesChest Radiography in Thoracic Polytrauma: Mai-Lan Ho Fernando R. GutierrezSyedNo ratings yet
- Jurnal RadiologiDocument5 pagesJurnal RadiologiKen FcNo ratings yet
- Ds 2053 Medical Examination Immigrant VisaDocument8 pagesDs 2053 Medical Examination Immigrant VisaangelgirlfabNo ratings yet
- Chest & Abdomen Mobile Radiography - DR - RanaDocument23 pagesChest & Abdomen Mobile Radiography - DR - RanaRana Abd AlmugeethNo ratings yet
- Imaging Pulmonary Infection, Classic Sign and Pattern PRESENTASIDocument84 pagesImaging Pulmonary Infection, Classic Sign and Pattern PRESENTASIMark Brown100% (1)
- Interpretation of Chest RadiographDocument7 pagesInterpretation of Chest RadiographhengkileonardNo ratings yet
- Chest X-Ray AnnaDocument51 pagesChest X-Ray Annaapi-26159412100% (1)
- X-Ray Interpretation PDFDocument41 pagesX-Ray Interpretation PDFNaveen Koval100% (2)
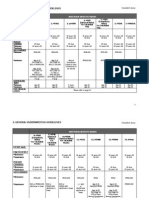
- General Underwriting Guidelines: Additional Benefits/RidersDocument5 pagesGeneral Underwriting Guidelines: Additional Benefits/RidersdikirNo ratings yet
- Readme Chestxray PDFDocument5 pagesReadme Chestxray PDFKibrom HaftuNo ratings yet
- 15 Signs in Thoracic Imaging.20Document15 pages15 Signs in Thoracic Imaging.20Don Kihot100% (1)
- JRI 13 Full PDFDocument76 pagesJRI 13 Full PDFAGNES TRIANA BASJANo ratings yet
- Chest X-Ray InterpretationDocument3 pagesChest X-Ray InterpretationHaluk AlibazogluNo ratings yet
- Pleural Effusion - Diagnosis, Treatment, and Management 1Document22 pagesPleural Effusion - Diagnosis, Treatment, and Management 1samice5No ratings yet
- Digital - PHD - Manuscript - Sunay Rodriguez PerezDocument189 pagesDigital - PHD - Manuscript - Sunay Rodriguez PerezAlberto GonzalesNo ratings yet
- Far Eastern University NRMF: Case StudyDocument63 pagesFar Eastern University NRMF: Case StudyRochÜLegaspiNo ratings yet
- Assessment of Pulmonary Edema: Principles and PracticeDocument14 pagesAssessment of Pulmonary Edema: Principles and PracticeJeanPandieNo ratings yet
- How To Read X-RayDocument8 pagesHow To Read X-RayPeterson Wachira HscNo ratings yet
- Ge 97Document310 pagesGe 97Moath ZorqanNo ratings yet