
Full Download Book Goldsmiths Assisted Ventilation of The Neonate An Evidence Based Approach To Newborn Respiratory Care PDF
Full Download Book Goldsmiths Assisted Ventilation of The Neonate An Evidence Based Approach To Newborn Respiratory Care PDF
You might also like
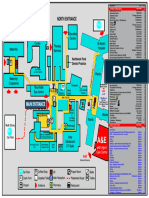
- Northwick Park Hospital Site MapDocument1 pageNorthwick Park Hospital Site MapHasaan KhanNo ratings yet
- Full Download Book Developmental Behavioral Pediatrics 5Th Edition PDFDocument41 pagesFull Download Book Developmental Behavioral Pediatrics 5Th Edition PDFmildred.jones506100% (28)
- Full Download Book Google Cloud Certified Professional Cloud Architect All in One Exam Guide PDFDocument41 pagesFull Download Book Google Cloud Certified Professional Cloud Architect All in One Exam Guide PDFmel.miller661100% (26)
- Full Download Book Google Cloud Certified Professional Cloud Architect All in One Exam Guide PDFDocument41 pagesFull Download Book Google Cloud Certified Professional Cloud Architect All in One Exam Guide PDFmel.miller661100% (26)
- Ebook Campbell Walsh Wein Handbook of Urology PDF Full Chapter PDFDocument67 pagesEbook Campbell Walsh Wein Handbook of Urology PDF Full Chapter PDFfrank.daniels751100% (33)
- Fuhrman and Zimmerman x27 S Pediatric Critical Care Sixth Edition 2021Document2,609 pagesFuhrman and Zimmerman x27 S Pediatric Critical Care Sixth Edition 2021Dr. Andre Manzan100% (3)
- The Mindful Way Through DepressionDocument2 pagesThe Mindful Way Through Depressionjulie77a0% (4)
- Date and Time Focus Data: Difficulty of BreathingDocument4 pagesDate and Time Focus Data: Difficulty of BreathingSoleil Maxwell100% (1)
- Full Download Book Rare Earth Metal Organic Framework Hybrid Materials For Luminescence Responsive Chemical Sensors PDFDocument41 pagesFull Download Book Rare Earth Metal Organic Framework Hybrid Materials For Luminescence Responsive Chemical Sensors PDFrobin.patton746100% (31)
- Full Download Book Rapid Detection of Food Adulterants and Contaminants Theory and Practice PDFDocument41 pagesFull Download Book Rapid Detection of Food Adulterants and Contaminants Theory and Practice PDFrobin.patton746100% (29)
- Full Download Book Advanced Pedot Thermoelectric Materials PDFDocument41 pagesFull Download Book Advanced Pedot Thermoelectric Materials PDFtonja.oneal380100% (29)
- Full Download Book Randomly Deployed Wireless Sensor Networks PDFDocument41 pagesFull Download Book Randomly Deployed Wireless Sensor Networks PDFrobin.patton746100% (30)
- Full Download Book Rainfall Modeling Measurement and Applications PDFDocument41 pagesFull Download Book Rainfall Modeling Measurement and Applications PDFrobin.patton746100% (31)
- Full Download Book Advanced Oxidation Processes For Effluent Treatment Plants PDFDocument41 pagesFull Download Book Advanced Oxidation Processes For Effluent Treatment Plants PDFwilliam.pilgrim541100% (31)
- Full Download Book Advanced Rare Earth Based Ceramic Nanomaterials 2 PDFDocument41 pagesFull Download Book Advanced Rare Earth Based Ceramic Nanomaterials 2 PDFtonja.oneal380100% (29)
- Full Download Book Rare Earths Industry Technological Economic and Environmental Implications PDFDocument41 pagesFull Download Book Rare Earths Industry Technological Economic and Environmental Implications PDFjoe.silva921100% (28)
- Full Download Book Advanced Rare Earth Based Ceramic Nanomaterials PDFDocument41 pagesFull Download Book Advanced Rare Earth Based Ceramic Nanomaterials PDFtonja.oneal380100% (29)
- Full Download Book Advanced Water Treatment Electrochemical Methods PDFDocument22 pagesFull Download Book Advanced Water Treatment Electrochemical Methods PDFtonja.oneal380100% (33)
- Full Download Book Advanced Nutrition and Human Metabolism 3 PDFDocument41 pagesFull Download Book Advanced Nutrition and Human Metabolism 3 PDFwilliam.pilgrim541100% (31)
- Full Download Book Radar Remote Sensing Applications and Challenges PDFDocument41 pagesFull Download Book Radar Remote Sensing Applications and Challenges PDFrobin.patton746100% (33)
- Full Download Book Reaction Rate Theory and Rare Events Simulations PDFDocument41 pagesFull Download Book Reaction Rate Theory and Rare Events Simulations PDFjoe.silva921100% (30)
- Full Download Book Advanced Nanomaterials For Pollutant Sensing and Environmental Catalysis PDFDocument41 pagesFull Download Book Advanced Nanomaterials For Pollutant Sensing and Environmental Catalysis PDFwilliam.pilgrim541100% (31)
- Full Download Book Advanced Nutrition and Human Metabolism 2 PDFDocument41 pagesFull Download Book Advanced Nutrition and Human Metabolism 2 PDFwilliam.pilgrim541100% (32)
- Full Download Book Advances in Additive Manufacturing Artificial Intelligence Nature Inspired and Biomanufacturing PDFDocument41 pagesFull Download Book Advances in Additive Manufacturing Artificial Intelligence Nature Inspired and Biomanufacturing PDFtonja.oneal380100% (31)
- Klaus and Fanaroffs Care of The High Risk Neonate 7Th Edition Edition Avroy A Fanaroff Full Chapter PDFDocument69 pagesKlaus and Fanaroffs Care of The High Risk Neonate 7Th Edition Edition Avroy A Fanaroff Full Chapter PDFmatezhyba100% (5)
- Avery's Diseases of The Newborn, Eleventh Edition - 2024Document1,849 pagesAvery's Diseases of The Newborn, Eleventh Edition - 2024Brillence M SammyNo ratings yet
- Nelson Essentials of Pediatrics Karen J Marcdante MD Robert M Kliegman MD Full ChapterDocument67 pagesNelson Essentials of Pediatrics Karen J Marcdante MD Robert M Kliegman MD Full Chapterbarbara.holmes539100% (12)
- (Download PDF) Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Full Chapter PDFDocument69 pages(Download PDF) Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Full Chapter PDFgoibmajkic100% (6)
- PDF Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Ebook Full ChapterDocument53 pagesPDF Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Ebook Full Chaptereugene.throgmorton306100% (4)
- Ebook Nelson Essentials of Pediatrics 2 Full Chapter PDFDocument67 pagesEbook Nelson Essentials of Pediatrics 2 Full Chapter PDFtimothy.skubis678100% (37)
- Full Download PDF of Nelson Textbook of Pediatrics 20th Edition Robert M. Kliegman - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Nelson Textbook of Pediatrics 20th Edition Robert M. Kliegman - Ebook PDF All Chaptersapuanboatin100% (6)
- 4062 Jopon 212Document48 pages4062 Jopon 212asep100% (1)
- Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Full ChapterDocument53 pagesNelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Full Chapterbarbara.holmes539100% (14)
- Ebook Pediatric Secrets PDF Full Chapter PDFDocument67 pagesEbook Pediatric Secrets PDF Full Chapter PDFsarah.pogue790100% (38)
- Full Download PDF of (Original PDF) Kendig's Disorders of The Respiratory Tract in Children 9th Edition All ChapterDocument43 pagesFull Download PDF of (Original PDF) Kendig's Disorders of The Respiratory Tract in Children 9th Edition All Chapterprillaaguil100% (6)
- 3358full Download PDF of Fuhrman and Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman - Ebook PDF All ChapterDocument69 pages3358full Download PDF of Fuhrman and Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman - Ebook PDF All Chapterposterkinwa100% (7)
- Full Download PDF of Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Edition Jerry Zimmerman - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Edition Jerry Zimmerman - Ebook PDF All Chapternaveaukatab100% (4)
- Full Download PDF of Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman - Ebook PDF All Chaptervockoairike100% (5)
- Neonatal and Pediatric Pharmacology Therapeutic Principles in Practice 4th Edition Ebook PDFDocument62 pagesNeonatal and Pediatric Pharmacology Therapeutic Principles in Practice 4th Edition Ebook PDFeleanor.gamble412100% (47)
- Full Download Book Breastfeeding A Guide For The Medical Profession PDFDocument41 pagesFull Download Book Breastfeeding A Guide For The Medical Profession PDFgeorge.pittman905100% (28)
- Full Download Book Breastfeeding A Guide For The Medical Professional PDFDocument41 pagesFull Download Book Breastfeeding A Guide For The Medical Professional PDFgeorge.pittman905100% (28)
- Merenstein Gardners Handbook of Neonatal Intensive Care E Book 8Th Edition PDF Full Chapter PDFDocument53 pagesMerenstein Gardners Handbook of Neonatal Intensive Care E Book 8Th Edition PDF Full Chapter PDFiberthschana100% (6)
- Fuhrman and Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chapter PDFDocument69 pagesFuhrman and Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chapter PDFzbychozeyad100% (6)
- (Download PDF) Pediatric Secrets 7Th Edition Richard A Polin Online Ebook All Chapter PDFDocument42 pages(Download PDF) Pediatric Secrets 7Th Edition Richard A Polin Online Ebook All Chapter PDFbree.daub373100% (10)
- Breastfeeding A Guide For The Medical Professional 9Th Edition Ruth A Lawrence Full ChapterDocument67 pagesBreastfeeding A Guide For The Medical Professional 9Th Edition Ruth A Lawrence Full Chapterjulia.swanson282100% (11)
- Pediatric PulmonolgyDocument1,242 pagesPediatric Pulmonolgybakru84No ratings yet
- Breastfeeding A Guide For The Medical Profession Ruth A Lawrence Full ChapterDocument67 pagesBreastfeeding A Guide For The Medical Profession Ruth A Lawrence Full Chapterjulia.swanson282100% (8)
- Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chapter PDFDocument69 pagesFuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chapter PDFzbychozeyad100% (6)
- Campbell Walsh Wein Handbook of Urology 1St Edition Alan W Partin MD PHD Full ChapterDocument67 pagesCampbell Walsh Wein Handbook of Urology 1St Edition Alan W Partin MD PHD Full Chapteredith.beltran702100% (7)
- Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Edition Jerry Zimmerman Full Chapter PDFDocument69 pagesFuhrman Zimmermans Pediatric Critical Care 6Th Edition Edition Jerry Zimmerman Full Chapter PDFzbychozeyad100% (6)
- Emassfile 7344Document69 pagesEmassfile 7344fuhanpaussuNo ratings yet
- Filedate 1424Document67 pagesFiledate 1424george.anderson189No ratings yet
- (Download PDF) Nelson Essentials of Pediatrics Karen J Marcdante MD Robert M Kliegman MD Full Chapter PDFDocument58 pages(Download PDF) Nelson Essentials of Pediatrics Karen J Marcdante MD Robert M Kliegman MD Full Chapter PDFgoibmajkic100% (5)
- Breastfeeding A Guide For The Medical ProfessionalDocument1,256 pagesBreastfeeding A Guide For The Medical ProfessionallinaNo ratings yet
- Ebook Fuhrman Zimmermans Pediatric Critical Care PDF Full Chapter PDFDocument67 pagesEbook Fuhrman Zimmermans Pediatric Critical Care PDF Full Chapter PDFirene.boswell292100% (36)
- Documentupload - 507download Full Ebook of Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Online PDF All ChapterDocument69 pagesDocumentupload - 507download Full Ebook of Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Online PDF All Chapterleghafowdar100% (9)
- Developmental-Behavioral Pediatrics, Fifth Edition 2023Document1,154 pagesDevelopmental-Behavioral Pediatrics, Fifth Edition 2023bromean.cubitos-0qNo ratings yet
- Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full ChapterDocument67 pagesFuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chaptertimothy.daniels842100% (11)
- Ebook Fuhrman and Zimmermans Pediatric Critical Care PDF Full Chapter PDFDocument67 pagesEbook Fuhrman and Zimmermans Pediatric Critical Care PDF Full Chapter PDFirene.boswell292100% (36)
- Neonatology Questions and Controversies The Newborn Lung, FourthDocument372 pagesNeonatology Questions and Controversies The Newborn Lung, FourthBrotherhood of KryptonianNo ratings yet
- Ebook Fuhrman Zimmermans Pediatric Critical Care 2 Full Chapter PDFDocument67 pagesEbook Fuhrman Zimmermans Pediatric Critical Care 2 Full Chapter PDFirene.boswell292100% (36)
- Ebook Essentials of Neonatal Ventilation 1St Edition PDF Full Chapter PDFDocument67 pagesEbook Essentials of Neonatal Ventilation 1St Edition PDF Full Chapter PDFsusie.plack633100% (32)
- Essentials of Neonatal Ventilation 1St Edition Rajiv PK Editor Full ChapterDocument67 pagesEssentials of Neonatal Ventilation 1St Edition Rajiv PK Editor Full Chapterhelen.fico427100% (7)
- Smiths Anesthesia For Infants and Children 10Th Edition Peter J Davis Full Download ChapterDocument51 pagesSmiths Anesthesia For Infants and Children 10Th Edition Peter J Davis Full Download Chapterjeffrey.dunaway695100% (10)
- Full Download Book Green Sustainable Process For Chemical and Environmental Engineering and Science Sonochemical Organic Synthesis PDFDocument41 pagesFull Download Book Green Sustainable Process For Chemical and Environmental Engineering and Science Sonochemical Organic Synthesis PDFmel.miller661100% (30)
- Full Download Book Great American Diseases Their Effects On The Course of North American History PDFDocument41 pagesFull Download Book Great American Diseases Their Effects On The Course of North American History PDFmel.miller661100% (33)
- Full Download Book Green Chemistry An Inclusive Approach PDFDocument41 pagesFull Download Book Green Chemistry An Inclusive Approach PDFmel.miller661100% (32)
- TriageDocument20 pagesTriageIGDNo ratings yet
- Acr Choosing Wisely ListDocument2 pagesAcr Choosing Wisely Listapi-277297976No ratings yet
- Handing and Taking OverDocument8 pagesHanding and Taking OverDivya Thomas100% (1)
- Rajasthan Government Health Scheme: List of Empaneled Hospitals As On 12-10-2021Document5 pagesRajasthan Government Health Scheme: List of Empaneled Hospitals As On 12-10-2021Ravindra RathoreNo ratings yet
- BSC (Hons) HNDDocument2 pagesBSC (Hons) HNDAli AzanNo ratings yet
- Comparación de La Efectividad Entre Telepractica y Terapia Presencial en EscolaresDocument6 pagesComparación de La Efectividad Entre Telepractica y Terapia Presencial en EscolaressdanobeitiaNo ratings yet
- Argumentative EssayDocument15 pagesArgumentative EssaySorna KailashNo ratings yet
- Communicable Disease QuestionsDocument51 pagesCommunicable Disease QuestionsHoney Lyn AlebioNo ratings yet
- Oral Antidiabetic Drugs in Pregnancy: The Other AlternativeDocument5 pagesOral Antidiabetic Drugs in Pregnancy: The Other AlternativePene Loredana MariellaNo ratings yet
- Chain Pharmacy: Assignment by Group 6 Zunaira Ahmed QaziDocument17 pagesChain Pharmacy: Assignment by Group 6 Zunaira Ahmed QaziJimmie ClassicNo ratings yet
- Holistic Approach To Full Mouth Rehab PDFDocument5 pagesHolistic Approach To Full Mouth Rehab PDFAna AlvaradoNo ratings yet
- Personal Accident: Claim FormDocument3 pagesPersonal Accident: Claim FormAmr TarekNo ratings yet
- PME FormDocument2 pagesPME FormManvi DaveNo ratings yet
- Darlene Jayle S. Satumba 2-B BS in Pharmacy PHARM 143 Activity 1Document2 pagesDarlene Jayle S. Satumba 2-B BS in Pharmacy PHARM 143 Activity 1Darlene Jayle SatumbaNo ratings yet
- Outbreak InvestigationDocument47 pagesOutbreak Investigationsarguss14100% (1)
- Hospital Valuation Insights and Perspectives BVR Webinar Barbo MeindlDocument24 pagesHospital Valuation Insights and Perspectives BVR Webinar Barbo MeindlText81No ratings yet
- Contact List of Education Support TeamDocument2 pagesContact List of Education Support Teamapi-671375887No ratings yet
- Announcement BSS BTKV 2018 - SEPT PDFDocument2 pagesAnnouncement BSS BTKV 2018 - SEPT PDFtenri ashariNo ratings yet
- Psycho Social MainDocument208 pagesPsycho Social MaintintuNo ratings yet
- Kenya Kwanza Manifesto Quick QuideDocument6 pagesKenya Kwanza Manifesto Quick QuideAden Duale0% (1)
- CBDRP Reporting Form 1Document1 pageCBDRP Reporting Form 1Romer EnajeNo ratings yet
- OGMCQs LJDocument4 pagesOGMCQs LJRyan ReNo ratings yet
- Blue Book 2019 2Document173 pagesBlue Book 2019 2MNo ratings yet
- Muscles TwitchDocument9 pagesMuscles TwitchPuspapuspa SuhaniNo ratings yet
- Sources of Public Health DataDocument11 pagesSources of Public Health Datadrtaa62No ratings yet
- Cecilia Laurente - Nursing Practice and CareerDocument11 pagesCecilia Laurente - Nursing Practice and CareerPrecious100% (1)
- C - II Review of Literature: HapterDocument31 pagesC - II Review of Literature: Haptersaikiabhasco100% (1)



























































































Download as pdf or txt
You might also like
- Northwick Park Hospital Site MapDocument1 pageNorthwick Park Hospital Site MapHasaan KhanNo ratings yet
- Full Download Book Developmental Behavioral Pediatrics 5Th Edition PDFDocument41 pagesFull Download Book Developmental Behavioral Pediatrics 5Th Edition PDFmildred.jones506100% (28)
- Full Download Book Google Cloud Certified Professional Cloud Architect All in One Exam Guide PDFDocument41 pagesFull Download Book Google Cloud Certified Professional Cloud Architect All in One Exam Guide PDFmel.miller661100% (26)
- Full Download Book Google Cloud Certified Professional Cloud Architect All in One Exam Guide PDFDocument41 pagesFull Download Book Google Cloud Certified Professional Cloud Architect All in One Exam Guide PDFmel.miller661100% (26)
- Ebook Campbell Walsh Wein Handbook of Urology PDF Full Chapter PDFDocument67 pagesEbook Campbell Walsh Wein Handbook of Urology PDF Full Chapter PDFfrank.daniels751100% (33)
- Fuhrman and Zimmerman x27 S Pediatric Critical Care Sixth Edition 2021Document2,609 pagesFuhrman and Zimmerman x27 S Pediatric Critical Care Sixth Edition 2021Dr. Andre Manzan100% (3)
- The Mindful Way Through DepressionDocument2 pagesThe Mindful Way Through Depressionjulie77a0% (4)
- Date and Time Focus Data: Difficulty of BreathingDocument4 pagesDate and Time Focus Data: Difficulty of BreathingSoleil Maxwell100% (1)
- Full Download Book Rare Earth Metal Organic Framework Hybrid Materials For Luminescence Responsive Chemical Sensors PDFDocument41 pagesFull Download Book Rare Earth Metal Organic Framework Hybrid Materials For Luminescence Responsive Chemical Sensors PDFrobin.patton746100% (31)
- Full Download Book Rapid Detection of Food Adulterants and Contaminants Theory and Practice PDFDocument41 pagesFull Download Book Rapid Detection of Food Adulterants and Contaminants Theory and Practice PDFrobin.patton746100% (29)
- Full Download Book Advanced Pedot Thermoelectric Materials PDFDocument41 pagesFull Download Book Advanced Pedot Thermoelectric Materials PDFtonja.oneal380100% (29)
- Full Download Book Randomly Deployed Wireless Sensor Networks PDFDocument41 pagesFull Download Book Randomly Deployed Wireless Sensor Networks PDFrobin.patton746100% (30)
- Full Download Book Rainfall Modeling Measurement and Applications PDFDocument41 pagesFull Download Book Rainfall Modeling Measurement and Applications PDFrobin.patton746100% (31)
- Full Download Book Advanced Oxidation Processes For Effluent Treatment Plants PDFDocument41 pagesFull Download Book Advanced Oxidation Processes For Effluent Treatment Plants PDFwilliam.pilgrim541100% (31)
- Full Download Book Advanced Rare Earth Based Ceramic Nanomaterials 2 PDFDocument41 pagesFull Download Book Advanced Rare Earth Based Ceramic Nanomaterials 2 PDFtonja.oneal380100% (29)
- Full Download Book Rare Earths Industry Technological Economic and Environmental Implications PDFDocument41 pagesFull Download Book Rare Earths Industry Technological Economic and Environmental Implications PDFjoe.silva921100% (28)
- Full Download Book Advanced Rare Earth Based Ceramic Nanomaterials PDFDocument41 pagesFull Download Book Advanced Rare Earth Based Ceramic Nanomaterials PDFtonja.oneal380100% (29)
- Full Download Book Advanced Water Treatment Electrochemical Methods PDFDocument22 pagesFull Download Book Advanced Water Treatment Electrochemical Methods PDFtonja.oneal380100% (33)
- Full Download Book Advanced Nutrition and Human Metabolism 3 PDFDocument41 pagesFull Download Book Advanced Nutrition and Human Metabolism 3 PDFwilliam.pilgrim541100% (31)
- Full Download Book Radar Remote Sensing Applications and Challenges PDFDocument41 pagesFull Download Book Radar Remote Sensing Applications and Challenges PDFrobin.patton746100% (33)
- Full Download Book Reaction Rate Theory and Rare Events Simulations PDFDocument41 pagesFull Download Book Reaction Rate Theory and Rare Events Simulations PDFjoe.silva921100% (30)
- Full Download Book Advanced Nanomaterials For Pollutant Sensing and Environmental Catalysis PDFDocument41 pagesFull Download Book Advanced Nanomaterials For Pollutant Sensing and Environmental Catalysis PDFwilliam.pilgrim541100% (31)
- Full Download Book Advanced Nutrition and Human Metabolism 2 PDFDocument41 pagesFull Download Book Advanced Nutrition and Human Metabolism 2 PDFwilliam.pilgrim541100% (32)
- Full Download Book Advances in Additive Manufacturing Artificial Intelligence Nature Inspired and Biomanufacturing PDFDocument41 pagesFull Download Book Advances in Additive Manufacturing Artificial Intelligence Nature Inspired and Biomanufacturing PDFtonja.oneal380100% (31)
- Klaus and Fanaroffs Care of The High Risk Neonate 7Th Edition Edition Avroy A Fanaroff Full Chapter PDFDocument69 pagesKlaus and Fanaroffs Care of The High Risk Neonate 7Th Edition Edition Avroy A Fanaroff Full Chapter PDFmatezhyba100% (5)
- Avery's Diseases of The Newborn, Eleventh Edition - 2024Document1,849 pagesAvery's Diseases of The Newborn, Eleventh Edition - 2024Brillence M SammyNo ratings yet
- Nelson Essentials of Pediatrics Karen J Marcdante MD Robert M Kliegman MD Full ChapterDocument67 pagesNelson Essentials of Pediatrics Karen J Marcdante MD Robert M Kliegman MD Full Chapterbarbara.holmes539100% (12)
- (Download PDF) Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Full Chapter PDFDocument69 pages(Download PDF) Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Full Chapter PDFgoibmajkic100% (6)
- PDF Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Ebook Full ChapterDocument53 pagesPDF Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Ebook Full Chaptereugene.throgmorton306100% (4)
- Ebook Nelson Essentials of Pediatrics 2 Full Chapter PDFDocument67 pagesEbook Nelson Essentials of Pediatrics 2 Full Chapter PDFtimothy.skubis678100% (37)
- Full Download PDF of Nelson Textbook of Pediatrics 20th Edition Robert M. Kliegman - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Nelson Textbook of Pediatrics 20th Edition Robert M. Kliegman - Ebook PDF All Chaptersapuanboatin100% (6)
- 4062 Jopon 212Document48 pages4062 Jopon 212asep100% (1)
- Nelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Full ChapterDocument53 pagesNelson Textbook of Pediatrics 20Th Edition Robert M Kliegman Full Chapterbarbara.holmes539100% (14)
- Ebook Pediatric Secrets PDF Full Chapter PDFDocument67 pagesEbook Pediatric Secrets PDF Full Chapter PDFsarah.pogue790100% (38)
- Full Download PDF of (Original PDF) Kendig's Disorders of The Respiratory Tract in Children 9th Edition All ChapterDocument43 pagesFull Download PDF of (Original PDF) Kendig's Disorders of The Respiratory Tract in Children 9th Edition All Chapterprillaaguil100% (6)
- 3358full Download PDF of Fuhrman and Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman - Ebook PDF All ChapterDocument69 pages3358full Download PDF of Fuhrman and Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman - Ebook PDF All Chapterposterkinwa100% (7)
- Full Download PDF of Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Edition Jerry Zimmerman - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Edition Jerry Zimmerman - Ebook PDF All Chapternaveaukatab100% (4)
- Full Download PDF of Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Fuhrman & Zimmerman's Pediatric Critical Care 6th Edition Jerry J. Zimmerman - Ebook PDF All Chaptervockoairike100% (5)
- Neonatal and Pediatric Pharmacology Therapeutic Principles in Practice 4th Edition Ebook PDFDocument62 pagesNeonatal and Pediatric Pharmacology Therapeutic Principles in Practice 4th Edition Ebook PDFeleanor.gamble412100% (47)
- Full Download Book Breastfeeding A Guide For The Medical Profession PDFDocument41 pagesFull Download Book Breastfeeding A Guide For The Medical Profession PDFgeorge.pittman905100% (28)
- Full Download Book Breastfeeding A Guide For The Medical Professional PDFDocument41 pagesFull Download Book Breastfeeding A Guide For The Medical Professional PDFgeorge.pittman905100% (28)
- Merenstein Gardners Handbook of Neonatal Intensive Care E Book 8Th Edition PDF Full Chapter PDFDocument53 pagesMerenstein Gardners Handbook of Neonatal Intensive Care E Book 8Th Edition PDF Full Chapter PDFiberthschana100% (6)
- Fuhrman and Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chapter PDFDocument69 pagesFuhrman and Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chapter PDFzbychozeyad100% (6)
- (Download PDF) Pediatric Secrets 7Th Edition Richard A Polin Online Ebook All Chapter PDFDocument42 pages(Download PDF) Pediatric Secrets 7Th Edition Richard A Polin Online Ebook All Chapter PDFbree.daub373100% (10)
- Breastfeeding A Guide For The Medical Professional 9Th Edition Ruth A Lawrence Full ChapterDocument67 pagesBreastfeeding A Guide For The Medical Professional 9Th Edition Ruth A Lawrence Full Chapterjulia.swanson282100% (11)
- Pediatric PulmonolgyDocument1,242 pagesPediatric Pulmonolgybakru84No ratings yet
- Breastfeeding A Guide For The Medical Profession Ruth A Lawrence Full ChapterDocument67 pagesBreastfeeding A Guide For The Medical Profession Ruth A Lawrence Full Chapterjulia.swanson282100% (8)
- Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chapter PDFDocument69 pagesFuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chapter PDFzbychozeyad100% (6)
- Campbell Walsh Wein Handbook of Urology 1St Edition Alan W Partin MD PHD Full ChapterDocument67 pagesCampbell Walsh Wein Handbook of Urology 1St Edition Alan W Partin MD PHD Full Chapteredith.beltran702100% (7)
- Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Edition Jerry Zimmerman Full Chapter PDFDocument69 pagesFuhrman Zimmermans Pediatric Critical Care 6Th Edition Edition Jerry Zimmerman Full Chapter PDFzbychozeyad100% (6)
- Emassfile 7344Document69 pagesEmassfile 7344fuhanpaussuNo ratings yet
- Filedate 1424Document67 pagesFiledate 1424george.anderson189No ratings yet
- (Download PDF) Nelson Essentials of Pediatrics Karen J Marcdante MD Robert M Kliegman MD Full Chapter PDFDocument58 pages(Download PDF) Nelson Essentials of Pediatrics Karen J Marcdante MD Robert M Kliegman MD Full Chapter PDFgoibmajkic100% (5)
- Breastfeeding A Guide For The Medical ProfessionalDocument1,256 pagesBreastfeeding A Guide For The Medical ProfessionallinaNo ratings yet
- Ebook Fuhrman Zimmermans Pediatric Critical Care PDF Full Chapter PDFDocument67 pagesEbook Fuhrman Zimmermans Pediatric Critical Care PDF Full Chapter PDFirene.boswell292100% (36)
- Documentupload - 507download Full Ebook of Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Online PDF All ChapterDocument69 pagesDocumentupload - 507download Full Ebook of Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Online PDF All Chapterleghafowdar100% (9)
- Developmental-Behavioral Pediatrics, Fifth Edition 2023Document1,154 pagesDevelopmental-Behavioral Pediatrics, Fifth Edition 2023bromean.cubitos-0qNo ratings yet
- Fuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full ChapterDocument67 pagesFuhrman Zimmermans Pediatric Critical Care 6Th Edition Jerry J Zimmerman Full Chaptertimothy.daniels842100% (11)
- Ebook Fuhrman and Zimmermans Pediatric Critical Care PDF Full Chapter PDFDocument67 pagesEbook Fuhrman and Zimmermans Pediatric Critical Care PDF Full Chapter PDFirene.boswell292100% (36)
- Neonatology Questions and Controversies The Newborn Lung, FourthDocument372 pagesNeonatology Questions and Controversies The Newborn Lung, FourthBrotherhood of KryptonianNo ratings yet
- Ebook Fuhrman Zimmermans Pediatric Critical Care 2 Full Chapter PDFDocument67 pagesEbook Fuhrman Zimmermans Pediatric Critical Care 2 Full Chapter PDFirene.boswell292100% (36)
- Ebook Essentials of Neonatal Ventilation 1St Edition PDF Full Chapter PDFDocument67 pagesEbook Essentials of Neonatal Ventilation 1St Edition PDF Full Chapter PDFsusie.plack633100% (32)
- Essentials of Neonatal Ventilation 1St Edition Rajiv PK Editor Full ChapterDocument67 pagesEssentials of Neonatal Ventilation 1St Edition Rajiv PK Editor Full Chapterhelen.fico427100% (7)
- Smiths Anesthesia For Infants and Children 10Th Edition Peter J Davis Full Download ChapterDocument51 pagesSmiths Anesthesia For Infants and Children 10Th Edition Peter J Davis Full Download Chapterjeffrey.dunaway695100% (10)
- Full Download Book Green Sustainable Process For Chemical and Environmental Engineering and Science Sonochemical Organic Synthesis PDFDocument41 pagesFull Download Book Green Sustainable Process For Chemical and Environmental Engineering and Science Sonochemical Organic Synthesis PDFmel.miller661100% (30)
- Full Download Book Great American Diseases Their Effects On The Course of North American History PDFDocument41 pagesFull Download Book Great American Diseases Their Effects On The Course of North American History PDFmel.miller661100% (33)
- Full Download Book Green Chemistry An Inclusive Approach PDFDocument41 pagesFull Download Book Green Chemistry An Inclusive Approach PDFmel.miller661100% (32)
- TriageDocument20 pagesTriageIGDNo ratings yet
- Acr Choosing Wisely ListDocument2 pagesAcr Choosing Wisely Listapi-277297976No ratings yet
- Handing and Taking OverDocument8 pagesHanding and Taking OverDivya Thomas100% (1)
- Rajasthan Government Health Scheme: List of Empaneled Hospitals As On 12-10-2021Document5 pagesRajasthan Government Health Scheme: List of Empaneled Hospitals As On 12-10-2021Ravindra RathoreNo ratings yet
- BSC (Hons) HNDDocument2 pagesBSC (Hons) HNDAli AzanNo ratings yet
- Comparación de La Efectividad Entre Telepractica y Terapia Presencial en EscolaresDocument6 pagesComparación de La Efectividad Entre Telepractica y Terapia Presencial en EscolaressdanobeitiaNo ratings yet
- Argumentative EssayDocument15 pagesArgumentative EssaySorna KailashNo ratings yet
- Communicable Disease QuestionsDocument51 pagesCommunicable Disease QuestionsHoney Lyn AlebioNo ratings yet
- Oral Antidiabetic Drugs in Pregnancy: The Other AlternativeDocument5 pagesOral Antidiabetic Drugs in Pregnancy: The Other AlternativePene Loredana MariellaNo ratings yet
- Chain Pharmacy: Assignment by Group 6 Zunaira Ahmed QaziDocument17 pagesChain Pharmacy: Assignment by Group 6 Zunaira Ahmed QaziJimmie ClassicNo ratings yet
- Holistic Approach To Full Mouth Rehab PDFDocument5 pagesHolistic Approach To Full Mouth Rehab PDFAna AlvaradoNo ratings yet
- Personal Accident: Claim FormDocument3 pagesPersonal Accident: Claim FormAmr TarekNo ratings yet
- PME FormDocument2 pagesPME FormManvi DaveNo ratings yet
- Darlene Jayle S. Satumba 2-B BS in Pharmacy PHARM 143 Activity 1Document2 pagesDarlene Jayle S. Satumba 2-B BS in Pharmacy PHARM 143 Activity 1Darlene Jayle SatumbaNo ratings yet
- Outbreak InvestigationDocument47 pagesOutbreak Investigationsarguss14100% (1)
- Hospital Valuation Insights and Perspectives BVR Webinar Barbo MeindlDocument24 pagesHospital Valuation Insights and Perspectives BVR Webinar Barbo MeindlText81No ratings yet
- Contact List of Education Support TeamDocument2 pagesContact List of Education Support Teamapi-671375887No ratings yet
- Announcement BSS BTKV 2018 - SEPT PDFDocument2 pagesAnnouncement BSS BTKV 2018 - SEPT PDFtenri ashariNo ratings yet
- Psycho Social MainDocument208 pagesPsycho Social MaintintuNo ratings yet
- Kenya Kwanza Manifesto Quick QuideDocument6 pagesKenya Kwanza Manifesto Quick QuideAden Duale0% (1)
- CBDRP Reporting Form 1Document1 pageCBDRP Reporting Form 1Romer EnajeNo ratings yet
- OGMCQs LJDocument4 pagesOGMCQs LJRyan ReNo ratings yet
- Blue Book 2019 2Document173 pagesBlue Book 2019 2MNo ratings yet
- Muscles TwitchDocument9 pagesMuscles TwitchPuspapuspa SuhaniNo ratings yet
- Sources of Public Health DataDocument11 pagesSources of Public Health Datadrtaa62No ratings yet
- Cecilia Laurente - Nursing Practice and CareerDocument11 pagesCecilia Laurente - Nursing Practice and CareerPrecious100% (1)
- C - II Review of Literature: HapterDocument31 pagesC - II Review of Literature: Haptersaikiabhasco100% (1)