Download as docx, pdf, or txt
You might also like
- Full Ebook of Hospice and Palliative Care For Companion Animals 2Nd Amir Shanan Online PDF All ChapterDocument69 pagesFull Ebook of Hospice and Palliative Care For Companion Animals 2Nd Amir Shanan Online PDF All Chaptermarthaflipp154059100% (7)
- Health Assessment Handout MayannDocument9 pagesHealth Assessment Handout MayannDENNIS N. MUÑOZNo ratings yet
- High Risk PregnancyDocument14 pagesHigh Risk Pregnancymarlynperez867173No ratings yet
- NCP For Aspiration PnuemoniaDocument11 pagesNCP For Aspiration PnuemoniaChristy Rose AgrisNo ratings yet
- Miner'S Diseases & Dust Hazards: NystagmusDocument7 pagesMiner'S Diseases & Dust Hazards: NystagmusPrabir GhoshNo ratings yet
- PneumoconiosisDocument51 pagesPneumoconiosisManoj Ranjan SahooNo ratings yet
- Dust Lung DiseasesDocument38 pagesDust Lung Diseasesankitkumaramit99No ratings yet
- 5 - Dust in Mine Air and Control TechnologyDocument17 pages5 - Dust in Mine Air and Control TechnologySude Yağmur ÇalışırNo ratings yet
- 5 6226231896498503742Document62 pages5 6226231896498503742dessypoerwantoNo ratings yet
- Lecture 4 - Mine DustDocument63 pagesLecture 4 - Mine DustBial100% (1)
- PneumoconiosisDocument19 pagesPneumoconiosisgabriela.was.gabbbieNo ratings yet
- What Are The Effects of Dust On The Lungs?: Chemicals and MaterialsDocument6 pagesWhat Are The Effects of Dust On The Lungs?: Chemicals and MaterialsSaiful ArifinNo ratings yet
- Construction Medical SurveyDocument4 pagesConstruction Medical SurveyVishnu AravindNo ratings yet
- Objective 6Document2 pagesObjective 6Amira SaidinNo ratings yet
- PNEUMOCONIOSISDocument53 pagesPNEUMOCONIOSISmaeliszxc kim100% (1)
- Presentation FinalDocument24 pagesPresentation FinalRahulNo ratings yet
- Dr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - Occu. Lung Dis Asbestosis Silicosis ByssinosisDocument26 pagesDr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - Occu. Lung Dis Asbestosis Silicosis ByssinosisDr. Prakash Kulkarni100% (2)
- Occupational HealthDocument14 pagesOccupational HealthChandanaNo ratings yet
- Microplastics in The Air Sources, Inhalation, and Health ConcernsDocument2 pagesMicroplastics in The Air Sources, Inhalation, and Health ConcernsdsjkfhkjsdhfNo ratings yet
- AIR POLLUTANTS HellenDocument9 pagesAIR POLLUTANTS HellenEmmanuel OgunduboyeNo ratings yet
- B.SC Degree Course in Nursing (Basic) Medical - Surgical Nursing - II Unit - X Occupational Lung DiseasesDocument101 pagesB.SC Degree Course in Nursing (Basic) Medical - Surgical Nursing - II Unit - X Occupational Lung DiseasesvigneshNo ratings yet
- 1.industrial DiseasesDocument4 pages1.industrial DiseasesShintonial OzileNo ratings yet
- Causes of Air PollutionDocument4 pagesCauses of Air PollutionSaroj KumarNo ratings yet
- Occupational Lung Diseases 1 2021Document11 pagesOccupational Lung Diseases 1 2021EMMANUEL BOTSHELONo ratings yet
- Design of Pleated Bag Filter System For Particulate Emission Control in Cement IndustryDocument6 pagesDesign of Pleated Bag Filter System For Particulate Emission Control in Cement IndustrySHAILESH PATELNo ratings yet
- Unit-Iii Oce551 Apce Typed Notes PDFDocument9 pagesUnit-Iii Oce551 Apce Typed Notes PDFammian790% (1)
- Various Types of PneumoconiosisDocument20 pagesVarious Types of PneumoconiosisSharin K VargheseNo ratings yet
- PneumoconiosisDocument7 pagesPneumoconiosisFriends ZoneNo ratings yet
- Otbt AdekDocument7 pagesOtbt AdekRockyValovaNo ratings yet
- Occupational Lung DiseasesDocument4 pagesOccupational Lung DiseasesMaha El BrashyNo ratings yet
- Air MicrobiologyDocument10 pagesAir MicrobiologyHazem BaderNo ratings yet
- Hazard To The Health in Workplace: by Dr. Rinaldo OslimDocument8 pagesHazard To The Health in Workplace: by Dr. Rinaldo OslimAidil AdlhaNo ratings yet
- SilicosisDocument11 pagesSilicosisDurge Raj GhalanNo ratings yet
- What Is SmogDocument4 pagesWhat Is SmogDebojyoti SarkarNo ratings yet
- Occupational Respiratory DiseasesDocument2 pagesOccupational Respiratory Diseases123No ratings yet
- SilicossisDocument72 pagesSilicossisAauLiiaa Lia LiiaNo ratings yet
- Air Microbiology 2009Document13 pagesAir Microbiology 2009Dr. SHIVA AITHAL100% (9)
- Compare Between The Following Terms:: I) Troposphere and Ionosphere LayersDocument2 pagesCompare Between The Following Terms:: I) Troposphere and Ionosphere LayersMohamed ahmedNo ratings yet
- Mine Gases and DustDocument85 pagesMine Gases and DustBenjaminNo ratings yet
- J NDF CGDocument6 pagesJ NDF CGDotia Modibo JamiuNo ratings yet
- Bab IDocument13 pagesBab IismailNo ratings yet
- Oration: Occupational Pneumoconiosis and TuberculosisDocument4 pagesOration: Occupational Pneumoconiosis and TuberculosisminingnovaNo ratings yet
- Chapter 9 - Mechanical Method To Remove PMDocument60 pagesChapter 9 - Mechanical Method To Remove PMCông Thành KiềuNo ratings yet
- How Damaging Is Breathing in Microplastics - Plastic Soup FoundationDocument1 pageHow Damaging Is Breathing in Microplastics - Plastic Soup FoundationkhamehameyaNo ratings yet
- Air, Noise and Thermal PollutionDocument13 pagesAir, Noise and Thermal PollutionRavneet KaurNo ratings yet
- Respiratory Diseases Among Dust Exposed WorkersDocument19 pagesRespiratory Diseases Among Dust Exposed WorkersAR MalikNo ratings yet
- PneumoconiosisDocument20 pagesPneumoconiosisankitkumaramit99No ratings yet
- Untitled Document 1Document2 pagesUntitled Document 1Sainath BhaleraoNo ratings yet
- L6 - AeromicrobiologyDocument41 pagesL6 - AeromicrobiologyFilipe Sobreira MunizNo ratings yet
- Air Pollution: Course: Environmental Planning & Practice (3671) Semester: Spring, 2020 Assignment - 1Document6 pagesAir Pollution: Course: Environmental Planning & Practice (3671) Semester: Spring, 2020 Assignment - 1adeel raziNo ratings yet
- Chapter 9 - Mechanical Method To Remove PMDocument50 pagesChapter 9 - Mechanical Method To Remove PMPhúc Nguyễn BáNo ratings yet
- Environmental & Occupational Lung DiseasesDocument12 pagesEnvironmental & Occupational Lung Diseasesamm1101No ratings yet
- Particulate MatterDocument4 pagesParticulate Matterniaz ahmedNo ratings yet
- Pollution Control in FoundriesDocument13 pagesPollution Control in FoundriesShabid Ashraf100% (2)
- SmogDocument2 pagesSmoganushjunejNo ratings yet
- Group 5 Presentation: Pneumoconiosis Pulmonary TumorDocument55 pagesGroup 5 Presentation: Pneumoconiosis Pulmonary Tumorchileshe chisalaNo ratings yet
- Health Hazards of Cement DustDocument20 pagesHealth Hazards of Cement DustRamu BanothNo ratings yet
- Write UpDocument4 pagesWrite Upbishtriya96No ratings yet
- 0511 REGmaterialspptDocument29 pages0511 REGmaterialspptazozinlcNo ratings yet
- "Particulates ": GROUP 3 - C19A1Document26 pages"Particulates ": GROUP 3 - C19A1Sherli VenandaNo ratings yet
- EE Mod4Document19 pagesEE Mod4B LIKHITH KUMARNo ratings yet
- Microplastic Crisis: Charting a Path to a Cleaner World: Global Collapse, #9From EverandMicroplastic Crisis: Charting a Path to a Cleaner World: Global Collapse, #9No ratings yet
- The Natural vs. Human Causes of Air Pollution : Environment Textbooks | Children's Environment BooksFrom EverandThe Natural vs. Human Causes of Air Pollution : Environment Textbooks | Children's Environment BooksRating: 4 out of 5 stars4/5 (1)
- Gallstones CholelithiasisDocument35 pagesGallstones Cholelithiasiszerish0208No ratings yet
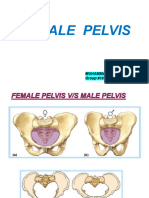
- Female Pelvis From Gynae and Obs Point of VeiwDocument46 pagesFemale Pelvis From Gynae and Obs Point of Veiwzerish0208No ratings yet
- Geography of Kyrgyzstan. Lectures 1-8Document31 pagesGeography of Kyrgyzstan. Lectures 1-8zerish02080% (1)
- Rheumatoid ArthritisDocument13 pagesRheumatoid Arthritiszerish0208No ratings yet
- Cardio-Respiratory Asessment For Physiotherapist: July 2015Document11 pagesCardio-Respiratory Asessment For Physiotherapist: July 2015Reza DehghaniNo ratings yet
- Eosinophilic Pneumonia-A Case ReportDocument1 pageEosinophilic Pneumonia-A Case ReportReitza RevilNo ratings yet
- Nursing Care Plan: Ineffective Breathing Pattern Related ToDocument4 pagesNursing Care Plan: Ineffective Breathing Pattern Related ToFrudz OrjalezaNo ratings yet
- Pulmonary EdemaDocument50 pagesPulmonary EdemaStacy LuceroNo ratings yet
- End-Of-Life Care: Managing Common Symptoms: Ross H. Albert, MD, PHD, Hartford Hospital, Hartford, ConnecticutDocument6 pagesEnd-Of-Life Care: Managing Common Symptoms: Ross H. Albert, MD, PHD, Hartford Hospital, Hartford, ConnecticutDoc CheebirdNo ratings yet
- Jurnal InternasionalDocument8 pagesJurnal InternasionalBerliana Via AnggeliNo ratings yet
- MS Compre 2015A Ans KeyDocument8 pagesMS Compre 2015A Ans KeyPaul Lexus Gomez LorenzoNo ratings yet
- Bronchial Asthma NCPDocument6 pagesBronchial Asthma NCPRacelle DelesNo ratings yet
- AsthmaDocument2 pagesAsthmaBerina ŠarićNo ratings yet
- Thoracic Trauma: Keperawatan Gawat Darurat 1 Ns. Siska Natalia, MSN-Palliative CareDocument22 pagesThoracic Trauma: Keperawatan Gawat Darurat 1 Ns. Siska Natalia, MSN-Palliative CareDevi Lamtiur GNo ratings yet
- Emergency Assistance Plan - Mango Bay - AZDocument6 pagesEmergency Assistance Plan - Mango Bay - AZThan WinNo ratings yet
- Final Exam Questions 3Document40 pagesFinal Exam Questions 3clarke skaikruNo ratings yet
- Case StudyDocument3 pagesCase StudyAnonymous Gof8o3No ratings yet
- Pediatrics Ratio PresentationDocument112 pagesPediatrics Ratio PresentationRobert John SaronaNo ratings yet
- Triage ATS PDFDocument7 pagesTriage ATS PDFkalembrowNo ratings yet
- Disease, Signs SymptomsDocument9 pagesDisease, Signs SymptomsGilang Putra RamadhanNo ratings yet
- DrowningDocument2 pagesDrowningAnonymous 0SYzMqje2No ratings yet
- 004 Practical-Manual PDFDocument72 pages004 Practical-Manual PDFRicardo Domingos100% (1)
- Cardiovascular Case StudyDocument13 pagesCardiovascular Case StudyJames MorganNo ratings yet
- Diagnostic ExaminationDocument10 pagesDiagnostic ExaminationHain YoloNo ratings yet
- Neonatal Respiratory Distress SyndromenhschoicesDocument6 pagesNeonatal Respiratory Distress SyndromenhschoicessehatkanNo ratings yet
- Anaphylaxis Clinical PresentationDocument9 pagesAnaphylaxis Clinical Presentationilhampaneja_x3No ratings yet
- Introduction To Bedside ClerkingDocument33 pagesIntroduction To Bedside ClerkingPrincewill SeiyefaNo ratings yet
- Activity IntoleranceDocument6 pagesActivity IntoleranceDenvEr CabaniLlasNo ratings yet
- CopdDocument30 pagesCopdsalmanhabeebekNo ratings yet
- Note On Asthma in AdultDocument5 pagesNote On Asthma in Adultshivam1969No ratings yet