Download as pdf or txt
You might also like
- r33 - Electric DiagramDocument31 pagesr33 - Electric Diagramalex.typexNo ratings yet
- Pressure TransducersDocument21 pagesPressure TransducersMahmoud Ashraf67% (3)
- EPC Challenges and Hot Topics - Huawei SingleEPC Solution - QI Workshop 12July2011-Part1 PDFDocument64 pagesEPC Challenges and Hot Topics - Huawei SingleEPC Solution - QI Workshop 12July2011-Part1 PDFFiras Ibrahim Al-Hamdany100% (1)
- 1 s2.0 S0021915022001393 MainDocument7 pages1 s2.0 S0021915022001393 MaincspprofessionalNo ratings yet
- Diabetes, Pancreatogenic Diabetes, and Pancreatic CancerDocument8 pagesDiabetes, Pancreatogenic Diabetes, and Pancreatic CancerTeodoraManNo ratings yet
- Fu RongDocument9 pagesFu RongTín NguyễnNo ratings yet
- International Journal of Cardiology: SciencedirectDocument8 pagesInternational Journal of Cardiology: SciencedirectsarahNo ratings yet
- UricDocument6 pagesUricLabontu IustinaNo ratings yet
- Central Venous Pressure and Acute Kidney Injury in Critically Ill Patients With Multiple Comorbidities A Large Retrospective Cohort StudyDocument10 pagesCentral Venous Pressure and Acute Kidney Injury in Critically Ill Patients With Multiple Comorbidities A Large Retrospective Cohort Studyady suciptoNo ratings yet
- Nutrients 14 00815 v2Document12 pagesNutrients 14 00815 v2donald duckNo ratings yet
- The Natural History Of, and Risk Factors For, Progressive Chronic Kidney Disease (CKD) : The Renal Impairment in Secondary Care (RIISC) Study Rationale and ProtocolDocument16 pagesThe Natural History Of, and Risk Factors For, Progressive Chronic Kidney Disease (CKD) : The Renal Impairment in Secondary Care (RIISC) Study Rationale and Protocolagung neutronNo ratings yet
- 1 s2.0 S0002870320302143 MainDocument9 pages1 s2.0 S0002870320302143 MaindeepNo ratings yet
- Clinical Laboratory Analysis - 2020 - Kayali - Glycosylated Hemoglobin A1c Predicts Coronary Artery Disease in Non Diabetic PDFDocument7 pagesClinical Laboratory Analysis - 2020 - Kayali - Glycosylated Hemoglobin A1c Predicts Coronary Artery Disease in Non Diabetic PDFrindayusticiaNo ratings yet
- Int J Clinical Practice - 2010 - Sinan Deveci - The Association Between Serum Uric Acid Level and Coronary Artery DiseaseDocument8 pagesInt J Clinical Practice - 2010 - Sinan Deveci - The Association Between Serum Uric Acid Level and Coronary Artery DiseasealitrnfbNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument7 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsMarco Antonio Guardamino OjedaNo ratings yet
- DBT y Obs SarcopenicaDocument8 pagesDBT y Obs SarcopenicaestesiesundriveNo ratings yet
- ĐTĐ Type 2Document10 pagesĐTĐ Type 2ngọc ngôNo ratings yet
- Journal Reading Bahan PDFDocument8 pagesJournal Reading Bahan PDFRudy Arindra WijayaNo ratings yet
- TestDocument11 pagesTestAfifahNo ratings yet
- Research Open AccessDocument12 pagesResearch Open AccessmartarguezNo ratings yet
- The Role of Glycemic Variability in Cardiovascular DisordersDocument15 pagesThe Role of Glycemic Variability in Cardiovascular DisordersNinaRicaR.RamosNo ratings yet
- Prevalence of Diabetes and Its Effects On Stroke Outcomes: A Meta-Analysis and Literature ReviewDocument13 pagesPrevalence of Diabetes and Its Effects On Stroke Outcomes: A Meta-Analysis and Literature ReviewarinyNo ratings yet
- Prediabetes: Why Should We Care?: Ashkan Zand, M.D. Karim Ibrahim, M.D. Bhargavi Patham, M.DDocument9 pagesPrediabetes: Why Should We Care?: Ashkan Zand, M.D. Karim Ibrahim, M.D. Bhargavi Patham, M.DCharlotte KeckhutNo ratings yet
- Axial Myopia and Low HbA1c Level Are Correlated AnDocument8 pagesAxial Myopia and Low HbA1c Level Are Correlated AnGeert SmoldNo ratings yet
- Diabetes y Relacion Entre Carcinoma HepatocelularDocument7 pagesDiabetes y Relacion Entre Carcinoma HepatocelularAnha Lagos ReyesNo ratings yet
- Hypertension and Chronic Kidney Disease in Asian PopulationsDocument6 pagesHypertension and Chronic Kidney Disease in Asian PopulationsBIETRIS WARISYUNo ratings yet
- Oup Accepted Manuscript 2020Document11 pagesOup Accepted Manuscript 2020DendyNo ratings yet
- The Effect of Ketogenic Diet On Shared Risk Factors of Cardiovascular Disease and CancerDocument22 pagesThe Effect of Ketogenic Diet On Shared Risk Factors of Cardiovascular Disease and CancerCierra NolenNo ratings yet
- Platelets Distribution Width As A Clue of Vascular Complications in Diabetic PatientsDocument3 pagesPlatelets Distribution Width As A Clue of Vascular Complications in Diabetic PatientsDr. Asaad Mohammed Ahmed BabkerNo ratings yet
- Erc e HtaDocument10 pagesErc e HtamiguelalmenarezNo ratings yet
- Additive Effect of Sarcopenia and Anemia On The 10-Year Risk of Diab PDFDocument9 pagesAdditive Effect of Sarcopenia and Anemia On The 10-Year Risk of Diab PDFAfonsoNo ratings yet
- Sfad 101Document14 pagesSfad 101el himawatiNo ratings yet
- Gfad 118Document10 pagesGfad 118pepegiovannyNo ratings yet
- Dgab 636Document10 pagesDgab 636Fifi RetiatyNo ratings yet
- Study of Hemotologicalprofile and Serum Iron Indices in Chronic Kidney Disease in Tertiary Care CentreDocument5 pagesStudy of Hemotologicalprofile and Serum Iron Indices in Chronic Kidney Disease in Tertiary Care CentreIJAR JOURNALNo ratings yet
- The Definition of Acute Kidney Injury and Its Use in PracticeDocument12 pagesThe Definition of Acute Kidney Injury and Its Use in PracticewelinNo ratings yet
- Waist To Hip RatioDocument6 pagesWaist To Hip RatioChay AlcantaraNo ratings yet
- Novel Pathological Implications of Serum Uric Acid - 2023 - Diabetes Research AnDocument8 pagesNovel Pathological Implications of Serum Uric Acid - 2023 - Diabetes Research Analerta.bfcmNo ratings yet
- Relationship Between C-Reactive Protein, White Blood Cell Count and Metabolic Syndrome in Nigerians With Type 2 Diabetes MellitusDocument11 pagesRelationship Between C-Reactive Protein, White Blood Cell Count and Metabolic Syndrome in Nigerians With Type 2 Diabetes MellitusPaul Gesswein FonatabaNo ratings yet
- Glycated Hemoglobin and EterosclerosisDocument15 pagesGlycated Hemoglobin and EterosclerosisLIZARDO CRUZADO DIAZNo ratings yet
- Ev 12 2020 04 AG - 5359 0562Document6 pagesEv 12 2020 04 AG - 5359 0562Saran RalucaNo ratings yet
- JDR2019 7825804Document9 pagesJDR2019 7825804Anonymous Xc7NwZzoNo ratings yet
- JreadDocument1 pageJreadAiraa ShaneNo ratings yet
- Cost-Effectiveness - A Modeled AnalysisDocument13 pagesCost-Effectiveness - A Modeled AnalysisAngelo Cardoso PereiraNo ratings yet
- Singapur PDFDocument7 pagesSingapur PDFLeidy AguasNo ratings yet
- Role of Kidney Injury in Sepsis: Review Open AccessDocument6 pagesRole of Kidney Injury in Sepsis: Review Open AccessnudhakoNo ratings yet
- Diagnosis and Treatment of Acute Kidney Injury in PediatricsDocument13 pagesDiagnosis and Treatment of Acute Kidney Injury in PediatricsagungNo ratings yet
- Biomarcadores Post Aki A ErcDocument12 pagesBiomarcadores Post Aki A ErcGiss UrizarNo ratings yet
- DD 22Document5 pagesDD 22siska dwiNo ratings yet
- Review Paper - Hasna UlyaDocument4 pagesReview Paper - Hasna UlyaHasna Ulya AnnafisNo ratings yet
- Lipid Profile in CKDDocument4 pagesLipid Profile in CKDAmiyanshu BeheraNo ratings yet
- Literature Review On Acute Coronary SyndromeDocument7 pagesLiterature Review On Acute Coronary Syndromegazqaacnd100% (1)
- Platelet Indices in Diabetics and InflueDocument7 pagesPlatelet Indices in Diabetics and InflueRajesh DebbarmaNo ratings yet
- CKD Risk FactorsDocument14 pagesCKD Risk FactorsSrinivas PingaliNo ratings yet
- Effect of Coffee Consumption On Renal Outcome: A Systematic Review and Meta-Analysis of Clinical StudiesDocument16 pagesEffect of Coffee Consumption On Renal Outcome: A Systematic Review and Meta-Analysis of Clinical StudiesAbrilNo ratings yet
- DM Post Transplant StudyDocument7 pagesDM Post Transplant StudyKalpeshRohraNo ratings yet
- Hyperglycemiainacute Coronarysyndromes: From Mechanisms To Prognostic ImplicationsDocument18 pagesHyperglycemiainacute Coronarysyndromes: From Mechanisms To Prognostic ImplicationsFco Josue Orellana MarinNo ratings yet
- Research ArticleDocument11 pagesResearch ArticleWahyuniNo ratings yet
- 1 s2.0 S1051227616301789 MainDocument7 pages1 s2.0 S1051227616301789 MainResearch OfficeNo ratings yet
- Chronic Kidney Disease As Cardiovascular Risk Factor in Routine Clinical Practice A Position Statement by The Council of The European Renal AssociationDocument5 pagesChronic Kidney Disease As Cardiovascular Risk Factor in Routine Clinical Practice A Position Statement by The Council of The European Renal AssociationPepin SalasNo ratings yet
- Metabolic Dysfunction Associated Steatotic Liver Disease Increa 2023 EClinicDocument11 pagesMetabolic Dysfunction Associated Steatotic Liver Disease Increa 2023 EClinicronaldquezada038No ratings yet
- Fendo 13 1007557Document9 pagesFendo 13 1007557Isini sehansa amarathungaNo ratings yet
- The Human Gut-Liver-Axis in Health and DiseaseFrom EverandThe Human Gut-Liver-Axis in Health and DiseaseAleksander KragNo ratings yet
- The Journal of Physiology - 2023 - Watkins - Myo Inositol Alters The Effects of Glucose Leptin and Insulin On PlacentalDocument19 pagesThe Journal of Physiology - 2023 - Watkins - Myo Inositol Alters The Effects of Glucose Leptin and Insulin On PlacentalMario CoelhoNo ratings yet
- J American Geriatrics Society - 2014 - Atkins - Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality ADocument8 pagesJ American Geriatrics Society - 2014 - Atkins - Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality AMario CoelhoNo ratings yet
- Evaluation of Anti-Aging Effects of Gemfibrozil OnDocument6 pagesEvaluation of Anti-Aging Effects of Gemfibrozil OnMario CoelhoNo ratings yet
- Antioxidants 13 00385Document19 pagesAntioxidants 13 00385Mario CoelhoNo ratings yet
- Fnut 09 929891Document11 pagesFnut 09 929891Mario CoelhoNo ratings yet
- Vitd th17Document10 pagesVitd th17Mario CoelhoNo ratings yet
- Vit d3Document5 pagesVit d3Mario CoelhoNo ratings yet
- Safety of 5000 International Units Daily Oral Dosing of Vitamin d3 For Four Years in Various Diseases 5f28c908f2e62Document8 pagesSafety of 5000 International Units Daily Oral Dosing of Vitamin d3 For Four Years in Various Diseases 5f28c908f2e62Mario CoelhoNo ratings yet
- A Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisDocument14 pagesA Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisMario CoelhoNo ratings yet
- Astm C796Document6 pagesAstm C796Abel ClarosNo ratings yet
- Asmiv T I Dwgs For 3keDocument14 pagesAsmiv T I Dwgs For 3kePSI Guillermo Francisco RuizNo ratings yet
- 1.2m Type 123 Ku Ext RT Class II SpecDocument2 pages1.2m Type 123 Ku Ext RT Class II SpecPrithish DevadigaNo ratings yet
- Determination of Negative Permittivity and PermeabDocument6 pagesDetermination of Negative Permittivity and PermeabNewton GomesNo ratings yet
- Calculation Welding RodsDocument37 pagesCalculation Welding RodsErlinawati Bintu SupiyoNo ratings yet
- Machine ToolsDocument48 pagesMachine ToolsPrabhu VNo ratings yet
- Abacus Masterycheckpoint Y3Document15 pagesAbacus Masterycheckpoint Y30502208864No ratings yet
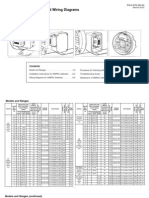
- Installation Instructions and Wiring Diagrams For All Models and RangesDocument8 pagesInstallation Instructions and Wiring Diagrams For All Models and RangesMaria MusyNo ratings yet
- Comparative Study On The Compressive Strength and Production Cost of Hollow Concrete Block (HCB) With and Without Red Ash in Tepi Town, EthiopiaDocument7 pagesComparative Study On The Compressive Strength and Production Cost of Hollow Concrete Block (HCB) With and Without Red Ash in Tepi Town, EthiopiaKaramara Training & ConsultancyNo ratings yet
- Absolute Value of Dance HandoutDocument3 pagesAbsolute Value of Dance Handoutapi-341104695No ratings yet
- Sub: Antenna & Radiowave Propogation Experiment No.2 Study of The Structure and Operation of Wired, Aperture, Planar and Array AntennasDocument10 pagesSub: Antenna & Radiowave Propogation Experiment No.2 Study of The Structure and Operation of Wired, Aperture, Planar and Array AntennasAtharv NigamNo ratings yet
- Transportation Engineering 1 Question Bank - Mumbai UniversityDocument10 pagesTransportation Engineering 1 Question Bank - Mumbai UniversityMegha Thomas0% (1)
- 73 Magazine 01 - January - 1961Document68 pages73 Magazine 01 - January - 1961viajerocanarioNo ratings yet
- Computation of Abutment Scour Using HEC-18 Equations SpreadsheetDocument7 pagesComputation of Abutment Scour Using HEC-18 Equations SpreadsheetAfolabi OladunniNo ratings yet
- Alloy - Wikipedia, The Free EncyclopediaDocument4 pagesAlloy - Wikipedia, The Free Encyclopediadonodoni0008No ratings yet
- Most Repeated Concepts & QuestionsDocument44 pagesMost Repeated Concepts & Questionsanshika tembhareNo ratings yet
- Emath 12Document8 pagesEmath 12Hanilen CatamaNo ratings yet
- FM Series: Measure CounterDocument1 pageFM Series: Measure CounterHarimurti HaryonoNo ratings yet
- FMEA Nu CorkDocument19 pagesFMEA Nu CorkAjit SamalNo ratings yet
- Project Report On Tpms DeviceDocument12 pagesProject Report On Tpms DeviceVikas KumarNo ratings yet
- Data Structures With C++Document169 pagesData Structures With C++Rachna BhatnagarNo ratings yet
- THUNDERDRIVE Series ENDocument1 pageTHUNDERDRIVE Series ENbaneaciprianNo ratings yet
- Computer Mcqs For NTS or Other TestsDocument89 pagesComputer Mcqs For NTS or Other TestsBetNex ExtraNo ratings yet
- Atos-Nt Rev 5-6-10Document486 pagesAtos-Nt Rev 5-6-10alessandro100% (1)
- Computer Science and EngineeringDocument235 pagesComputer Science and EngineeringABHISHEK CARMEL KURIANNo ratings yet
- Evsu-Occ Enrollment System: Subject Code Course Yearlevel Teacher Units Mid Grade Final Grade Grade RemarkDocument8 pagesEvsu-Occ Enrollment System: Subject Code Course Yearlevel Teacher Units Mid Grade Final Grade Grade RemarkMia Liza LapecirosNo ratings yet
- Analisa Teknis Pengujian Kekedapan Pengelasan Pada Tangki Tongkang Dengan Membandingkan Metode Chalk Test, Air Pressure Test Dan VacuumDocument18 pagesAnalisa Teknis Pengujian Kekedapan Pengelasan Pada Tangki Tongkang Dengan Membandingkan Metode Chalk Test, Air Pressure Test Dan VacuumIbnu HajarNo ratings yet