
Relation of Gemfibrozil Treatment and Lipid Levels
Relation of Gemfibrozil Treatment and Lipid Levels
You might also like
- Necrotic Gnome - Winters Daughter 5eDocument52 pagesNecrotic Gnome - Winters Daughter 5eMc Roxas75% (12)
- The Worm Farmer's Handbook - Table of ContentsDocument2 pagesThe Worm Farmer's Handbook - Table of ContentsChelsea Green PublishingNo ratings yet
- Instagram For Business - The Definitive Guide by Sked Social PDFDocument61 pagesInstagram For Business - The Definitive Guide by Sked Social PDFGrace ToqueNo ratings yet
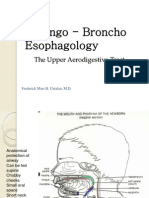
- Laryngo Broncho EsophagologyDocument94 pagesLaryngo Broncho EsophagologyFrederick Mars UntalanNo ratings yet
- Vitamin D Levels Predict All-Cause and Cardiovascular Disease Mortality in Subjects With The Metabolic SyndromeDocument7 pagesVitamin D Levels Predict All-Cause and Cardiovascular Disease Mortality in Subjects With The Metabolic SyndromeAgafioNo ratings yet
- Clinical Cardiology - October 1987 - Wolinsky - The Effects of Beta Adrenergic Blocking Agents On Blood Lipid LevelsDocument6 pagesClinical Cardiology - October 1987 - Wolinsky - The Effects of Beta Adrenergic Blocking Agents On Blood Lipid LevelsSrinivasa RaghavanNo ratings yet
- 2018 Dislipidemia-RevisaDocument16 pages2018 Dislipidemia-RevisaLuminita HutanuNo ratings yet
- Dislipidemia ACP 2017Document16 pagesDislipidemia ACP 2017José Luis PradoNo ratings yet
- High-Density Lipoprotein Cardiovascular Disease: Cholesterol andDocument8 pagesHigh-Density Lipoprotein Cardiovascular Disease: Cholesterol andStefania CristinaNo ratings yet
- Clinical ResearchDocument6 pagesClinical Researchnurul wahyuniNo ratings yet
- 8E - Lipid Sirt Study JANA 2010Document6 pages8E - Lipid Sirt Study JANA 2010alonso martinNo ratings yet
- New England Journal Medicine: The ofDocument13 pagesNew England Journal Medicine: The ofStefania CristinaNo ratings yet
- Hypertension JournalDocument5 pagesHypertension JournalYola SurbaktiNo ratings yet
- Barter (2007) HDL Cholesterol, Very Low Levels of LDLDocument10 pagesBarter (2007) HDL Cholesterol, Very Low Levels of LDLBruno TeixeiraNo ratings yet
- Circulationaha 122 063399Document12 pagesCirculationaha 122 063399Noel FrancoNo ratings yet
- Oxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaDocument9 pagesOxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaidiNo ratings yet
- Statin Intolerance, Bempedoic Acid, and Cardiovascular OutcomesDocument4 pagesStatin Intolerance, Bempedoic Acid, and Cardiovascular OutcomesAnderson Joel GomezNo ratings yet
- Artículo Dislipemia ESCDocument12 pagesArtículo Dislipemia ESCSMIBA MedicinaNo ratings yet
- Lipid Biomarkers Associated With Mortality in COVIDocument1 pageLipid Biomarkers Associated With Mortality in COVIConsultorio Pediatria ShaioNo ratings yet
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsDocument13 pagesEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiNo ratings yet
- 228A ABSTRACTS - Cardiac Function and Heart Failure Jacc March 3, 2004Document2 pages228A ABSTRACTS - Cardiac Function and Heart Failure Jacc March 3, 2004Yulianty Saulina FransiscaNo ratings yet
- Diabetes Treatment and Cardiovascular Safety: Achary Loomgarden MDDocument7 pagesDiabetes Treatment and Cardiovascular Safety: Achary Loomgarden MDCarlosECañasTorrealbaNo ratings yet
- How Statistical Deception Created The Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular DiseaseDocument11 pagesHow Statistical Deception Created The Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular DiseaseodhiseoNo ratings yet
- López-Bautista Et Al. - 2018 - Vitamin D Deficiency Is Not Associated With Fatty Liver in A Mexican PopulationDocument7 pagesLópez-Bautista Et Al. - 2018 - Vitamin D Deficiency Is Not Associated With Fatty Liver in A Mexican PopulationFabiola LópezNo ratings yet
- López-Bautista Et Al. - 2018 - Vitamin D Deficiency Is Not Associated With Fatty Liver in A Mexican PopulationDocument7 pagesLópez-Bautista Et Al. - 2018 - Vitamin D Deficiency Is Not Associated With Fatty Liver in A Mexican PopulationFabiola LópezNo ratings yet
- Original ContributionDocument9 pagesOriginal ContributionAgafioNo ratings yet
- 88 TopDocument1 page88 Toptchn azharNo ratings yet
- Ijms-22-00287Document10 pagesIjms-22-00287vidhi parekhNo ratings yet
- Vitamina D 2010Document7 pagesVitamina D 2010amb251No ratings yet
- NIH Public Access: The Road Connecting Obesity and Coronary Vasomotor Function: Straight Line or U-Turn?Document4 pagesNIH Public Access: The Road Connecting Obesity and Coronary Vasomotor Function: Straight Line or U-Turn?bawalNo ratings yet
- Heart Disease Literature ReviewDocument9 pagesHeart Disease Literature Reviewjyzapydigip3100% (1)
- Elevated LDL Cholesterol Levels Among Lean Mass HyDocument4 pagesElevated LDL Cholesterol Levels Among Lean Mass Hy8v6y5jsykbNo ratings yet
- Article 9Document10 pagesArticle 9vzwsvt7hgkNo ratings yet
- Gene TikDocument9 pagesGene TikVidini Kusuma AjiNo ratings yet
- CCR 17 E051121189015Document15 pagesCCR 17 E051121189015Paramitha HarmanNo ratings yet
- Clinical Implications of The Genetic Architecture of Dilated CardiomyopathyDocument11 pagesClinical Implications of The Genetic Architecture of Dilated CardiomyopathyIsabella-Diana ChelbanNo ratings yet
- Vitamin D and Cardiovascular Disease: Time For Large Randomized TrialsDocument3 pagesVitamin D and Cardiovascular Disease: Time For Large Randomized TrialsOkky Winang SaktyawanNo ratings yet
- Índice de Castelli - Summary Estimates of Cholesterol UsedDocument6 pagesÍndice de Castelli - Summary Estimates of Cholesterol UsedmartaacNo ratings yet
- Intradialitic HypotensionDocument7 pagesIntradialitic HypotensionanitaNo ratings yet
- Agodoa Jama 2002Document12 pagesAgodoa Jama 2002NandaCastroMedUFJFNo ratings yet
- 10 - Metabolic SyndromeDocument12 pages10 - Metabolic SyndromeLuisErnestoRodriguezMNo ratings yet
- Association Between Baseline LDL-C Level and TotalDocument14 pagesAssociation Between Baseline LDL-C Level and TotalMr. LNo ratings yet
- New England Journal Medicine: The ofDocument15 pagesNew England Journal Medicine: The ofFerry Fawzi AnnorNo ratings yet
- Mechanisms, Clinical Implications, and Treatment of Intradialytic HypotensionDocument7 pagesMechanisms, Clinical Implications, and Treatment of Intradialytic Hypotensionhemer hadyn calderon alvitesNo ratings yet
- Cho Paradigm For Reduction of ASCVDDocument17 pagesCho Paradigm For Reduction of ASCVDBubu ToNo ratings yet
- Journal of Clinical & Translational EndocrinologyDocument7 pagesJournal of Clinical & Translational EndocrinologyArini NurlelaNo ratings yet
- 1 s2.0 S073510972207125X MainDocument12 pages1 s2.0 S073510972207125X MainAndreea RacovitaNo ratings yet
- Journal Pbio 3001561Document23 pagesJournal Pbio 3001561philosophy-thoughtNo ratings yet
- Povsic Et Al 2024 Effect of Reconstituted Human Apolipoprotein A I On Recurrent Ischemic Events in Survivors of Acute MiDocument12 pagesPovsic Et Al 2024 Effect of Reconstituted Human Apolipoprotein A I On Recurrent Ischemic Events in Survivors of Acute MiCHARLES BROSLONo ratings yet
- Jamacardiology Zhang 2021 Oi 210061 1630597090.4739Document8 pagesJamacardiology Zhang 2021 Oi 210061 1630597090.4739AlizaPinkyNo ratings yet
- Diabetic Cardiomyopathy: Editorial (See Bertoni ET AL., P. 2 7 9 1)Document3 pagesDiabetic Cardiomyopathy: Editorial (See Bertoni ET AL., P. 2 7 9 1)aymenNo ratings yet
- Epidemiology of Familial Hypercholesterolaemia CoDocument9 pagesEpidemiology of Familial Hypercholesterolaemia CoSusana RocheNo ratings yet
- Srikant H 2016Document10 pagesSrikant H 2016aditya sekarNo ratings yet
- 1 s2.0 S0085253817304180 MainDocument8 pages1 s2.0 S0085253817304180 MainBryan FarrelNo ratings yet
- Soluble Adhesion Molecules and Coronary Heart Dise - 3Document1 pageSoluble Adhesion Molecules and Coronary Heart Dise - 3Ramón Díaz-AlersiNo ratings yet
- New England Journal Medicine: The ofDocument12 pagesNew England Journal Medicine: The ofrevi fitraNo ratings yet
- Preventing Cardiovascular Disease in Patients With.2 PDFDocument3 pagesPreventing Cardiovascular Disease in Patients With.2 PDFbacharelado2010No ratings yet
- Evacetrapib y Resultados Cardiovasculares en La Enfermedad Vascular de Alto RiesgoDocument10 pagesEvacetrapib y Resultados Cardiovasculares en La Enfermedad Vascular de Alto RiesgoAlan Villegas SorianoNo ratings yet
- Hta TtoDocument13 pagesHta TtoAmelia RiveraNo ratings yet
- Expanding Roles of Vitamin D: Edward GiovannucciDocument3 pagesExpanding Roles of Vitamin D: Edward GiovannucciAgafioNo ratings yet
- Association Between Serum Lipids and Survival in Hemodialysis Patients and Impact of RaceDocument11 pagesAssociation Between Serum Lipids and Survival in Hemodialysis Patients and Impact of RaceJuanCarlosGonzalezNo ratings yet
- Translating Molecular Discovery Into New Therapies For AtherosclerosisDocument11 pagesTranslating Molecular Discovery Into New Therapies For AtherosclerosisDzikrul Haq KarimullahNo ratings yet
- Pathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCDocument42 pagesPathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCCalvin LitraNo ratings yet
- Therapeutic LipidologyFrom EverandTherapeutic LipidologyMichael H. DavidsonNo ratings yet
- The Journal of Physiology - 2023 - Watkins - Myo Inositol Alters The Effects of Glucose Leptin and Insulin On PlacentalDocument19 pagesThe Journal of Physiology - 2023 - Watkins - Myo Inositol Alters The Effects of Glucose Leptin and Insulin On PlacentalMario CoelhoNo ratings yet
- J American Geriatrics Society - 2014 - Atkins - Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality ADocument8 pagesJ American Geriatrics Society - 2014 - Atkins - Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality AMario CoelhoNo ratings yet
- Evaluation of Anti-Aging Effects of Gemfibrozil OnDocument6 pagesEvaluation of Anti-Aging Effects of Gemfibrozil OnMario CoelhoNo ratings yet
- Antioxidants 13 00385Document19 pagesAntioxidants 13 00385Mario CoelhoNo ratings yet
- Lvac 001Document9 pagesLvac 001Mario CoelhoNo ratings yet
- Vitd th17Document10 pagesVitd th17Mario CoelhoNo ratings yet
- Fnut 09 929891Document11 pagesFnut 09 929891Mario CoelhoNo ratings yet
- A Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisDocument14 pagesA Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisMario CoelhoNo ratings yet
- Vit d3Document5 pagesVit d3Mario CoelhoNo ratings yet
- Safety of 5000 International Units Daily Oral Dosing of Vitamin d3 For Four Years in Various Diseases 5f28c908f2e62Document8 pagesSafety of 5000 International Units Daily Oral Dosing of Vitamin d3 For Four Years in Various Diseases 5f28c908f2e62Mario CoelhoNo ratings yet
- UNDocument419 pagesUNSiti Masruroh ArohNo ratings yet
- Unit 3 Prepare and Interpret Technical DrawingDocument20 pagesUnit 3 Prepare and Interpret Technical Drawingtracert_atanNo ratings yet
- PPC DrainDocument6 pagesPPC Drainherysyam1980No ratings yet
- Franchise PackageDocument3 pagesFranchise PackageJayson Nonan100% (1)
- Module 5Document27 pagesModule 5Labour lawNo ratings yet
- Final Seats Matrix Ss Counelling - 2022 D.M M.CHDocument55 pagesFinal Seats Matrix Ss Counelling - 2022 D.M M.CHMinerva Medical Treatment Pvt LtdNo ratings yet
- Sales Rebates ProcessingDocument1 pageSales Rebates ProcessingNavjyot SinghviNo ratings yet
- Final Project ML Nikita Chaturvedi 03.10.2021 Text AnalyticsDocument32 pagesFinal Project ML Nikita Chaturvedi 03.10.2021 Text AnalyticsNikita ChaturvediNo ratings yet
- Topic 1 - Whole NumbersDocument38 pagesTopic 1 - Whole Numbersnazri100% (3)
- Shape Memory Alloy Rotary Actuator For Cubesat Deployable StructuresDocument82 pagesShape Memory Alloy Rotary Actuator For Cubesat Deployable StructuresFernando Jesús Medina RodríguezNo ratings yet
- Working Capital Management With Reference To Thirumala Milk Products PVT - LTDDocument103 pagesWorking Capital Management With Reference To Thirumala Milk Products PVT - LTDsaryumba5538No ratings yet
- Φουρνος- convotherm - 4Document120 pagesΦουρνος- convotherm - 4Dimitris ThanasopoulosNo ratings yet
- ARA DraftProgWEBSITE1MayDocument13 pagesARA DraftProgWEBSITE1MayHNNo ratings yet
- CWTS 2 Community Service Proposal 2019Document5 pagesCWTS 2 Community Service Proposal 2019Paul BandolaNo ratings yet
- Insulated Flooring StanvacDocument7 pagesInsulated Flooring StanvacRamesh RoyNo ratings yet
- DLP IN ORAL COMMUNICATION-GRADE 11-EditedDocument6 pagesDLP IN ORAL COMMUNICATION-GRADE 11-EditedMaeann MirandoNo ratings yet
- تقرير الانجليزيDocument2 pagesتقرير الانجليزيbasel.khashashneh.44No ratings yet
- Tally Assignment 12Document90 pagesTally Assignment 12Kaushal SharmaNo ratings yet
- Acknowledgement (Draft 2) : IntroductionDocument3 pagesAcknowledgement (Draft 2) : IntroductionSHAIK AASHIQUE RASOOL ARCH-UG- 2018 BATCHNo ratings yet
- IJSARTV6I738053Document3 pagesIJSARTV6I738053VISHAL BHOJWANINo ratings yet
- FD Schedule & QBDocument6 pagesFD Schedule & QBDrDhananjhay GangineniNo ratings yet
- Buisness Plan OutlineDocument10 pagesBuisness Plan OutlinevangheliexNo ratings yet
- PCE Nautilus en 20130318Document2 pagesPCE Nautilus en 20130318Iker BasqueAdventureNo ratings yet
- BCS RulesDocument40 pagesBCS RulesHKF1971No ratings yet
- Butterfly CircusDocument2 pagesButterfly CircusSalma BenjellounNo ratings yet
- Install LogDocument36 pagesInstall Logfrans parulianNo ratings yet


































































































Download as pdf or txt
You might also like
- Necrotic Gnome - Winters Daughter 5eDocument52 pagesNecrotic Gnome - Winters Daughter 5eMc Roxas75% (12)
- The Worm Farmer's Handbook - Table of ContentsDocument2 pagesThe Worm Farmer's Handbook - Table of ContentsChelsea Green PublishingNo ratings yet
- Instagram For Business - The Definitive Guide by Sked Social PDFDocument61 pagesInstagram For Business - The Definitive Guide by Sked Social PDFGrace ToqueNo ratings yet
- Laryngo Broncho EsophagologyDocument94 pagesLaryngo Broncho EsophagologyFrederick Mars UntalanNo ratings yet
- Vitamin D Levels Predict All-Cause and Cardiovascular Disease Mortality in Subjects With The Metabolic SyndromeDocument7 pagesVitamin D Levels Predict All-Cause and Cardiovascular Disease Mortality in Subjects With The Metabolic SyndromeAgafioNo ratings yet
- Clinical Cardiology - October 1987 - Wolinsky - The Effects of Beta Adrenergic Blocking Agents On Blood Lipid LevelsDocument6 pagesClinical Cardiology - October 1987 - Wolinsky - The Effects of Beta Adrenergic Blocking Agents On Blood Lipid LevelsSrinivasa RaghavanNo ratings yet
- 2018 Dislipidemia-RevisaDocument16 pages2018 Dislipidemia-RevisaLuminita HutanuNo ratings yet
- Dislipidemia ACP 2017Document16 pagesDislipidemia ACP 2017José Luis PradoNo ratings yet
- High-Density Lipoprotein Cardiovascular Disease: Cholesterol andDocument8 pagesHigh-Density Lipoprotein Cardiovascular Disease: Cholesterol andStefania CristinaNo ratings yet
- Clinical ResearchDocument6 pagesClinical Researchnurul wahyuniNo ratings yet
- 8E - Lipid Sirt Study JANA 2010Document6 pages8E - Lipid Sirt Study JANA 2010alonso martinNo ratings yet
- New England Journal Medicine: The ofDocument13 pagesNew England Journal Medicine: The ofStefania CristinaNo ratings yet
- Hypertension JournalDocument5 pagesHypertension JournalYola SurbaktiNo ratings yet
- Barter (2007) HDL Cholesterol, Very Low Levels of LDLDocument10 pagesBarter (2007) HDL Cholesterol, Very Low Levels of LDLBruno TeixeiraNo ratings yet
- Circulationaha 122 063399Document12 pagesCirculationaha 122 063399Noel FrancoNo ratings yet
- Oxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaDocument9 pagesOxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaidiNo ratings yet
- Statin Intolerance, Bempedoic Acid, and Cardiovascular OutcomesDocument4 pagesStatin Intolerance, Bempedoic Acid, and Cardiovascular OutcomesAnderson Joel GomezNo ratings yet
- Artículo Dislipemia ESCDocument12 pagesArtículo Dislipemia ESCSMIBA MedicinaNo ratings yet
- Lipid Biomarkers Associated With Mortality in COVIDocument1 pageLipid Biomarkers Associated With Mortality in COVIConsultorio Pediatria ShaioNo ratings yet
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsDocument13 pagesEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiNo ratings yet
- 228A ABSTRACTS - Cardiac Function and Heart Failure Jacc March 3, 2004Document2 pages228A ABSTRACTS - Cardiac Function and Heart Failure Jacc March 3, 2004Yulianty Saulina FransiscaNo ratings yet
- Diabetes Treatment and Cardiovascular Safety: Achary Loomgarden MDDocument7 pagesDiabetes Treatment and Cardiovascular Safety: Achary Loomgarden MDCarlosECañasTorrealbaNo ratings yet
- How Statistical Deception Created The Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular DiseaseDocument11 pagesHow Statistical Deception Created The Appearance That Statins Are Safe and Effective in Primary and Secondary Prevention of Cardiovascular DiseaseodhiseoNo ratings yet
- López-Bautista Et Al. - 2018 - Vitamin D Deficiency Is Not Associated With Fatty Liver in A Mexican PopulationDocument7 pagesLópez-Bautista Et Al. - 2018 - Vitamin D Deficiency Is Not Associated With Fatty Liver in A Mexican PopulationFabiola LópezNo ratings yet
- López-Bautista Et Al. - 2018 - Vitamin D Deficiency Is Not Associated With Fatty Liver in A Mexican PopulationDocument7 pagesLópez-Bautista Et Al. - 2018 - Vitamin D Deficiency Is Not Associated With Fatty Liver in A Mexican PopulationFabiola LópezNo ratings yet
- Original ContributionDocument9 pagesOriginal ContributionAgafioNo ratings yet
- 88 TopDocument1 page88 Toptchn azharNo ratings yet
- Ijms-22-00287Document10 pagesIjms-22-00287vidhi parekhNo ratings yet
- Vitamina D 2010Document7 pagesVitamina D 2010amb251No ratings yet
- NIH Public Access: The Road Connecting Obesity and Coronary Vasomotor Function: Straight Line or U-Turn?Document4 pagesNIH Public Access: The Road Connecting Obesity and Coronary Vasomotor Function: Straight Line or U-Turn?bawalNo ratings yet
- Heart Disease Literature ReviewDocument9 pagesHeart Disease Literature Reviewjyzapydigip3100% (1)
- Elevated LDL Cholesterol Levels Among Lean Mass HyDocument4 pagesElevated LDL Cholesterol Levels Among Lean Mass Hy8v6y5jsykbNo ratings yet
- Article 9Document10 pagesArticle 9vzwsvt7hgkNo ratings yet
- Gene TikDocument9 pagesGene TikVidini Kusuma AjiNo ratings yet
- CCR 17 E051121189015Document15 pagesCCR 17 E051121189015Paramitha HarmanNo ratings yet
- Clinical Implications of The Genetic Architecture of Dilated CardiomyopathyDocument11 pagesClinical Implications of The Genetic Architecture of Dilated CardiomyopathyIsabella-Diana ChelbanNo ratings yet
- Vitamin D and Cardiovascular Disease: Time For Large Randomized TrialsDocument3 pagesVitamin D and Cardiovascular Disease: Time For Large Randomized TrialsOkky Winang SaktyawanNo ratings yet
- Índice de Castelli - Summary Estimates of Cholesterol UsedDocument6 pagesÍndice de Castelli - Summary Estimates of Cholesterol UsedmartaacNo ratings yet
- Intradialitic HypotensionDocument7 pagesIntradialitic HypotensionanitaNo ratings yet
- Agodoa Jama 2002Document12 pagesAgodoa Jama 2002NandaCastroMedUFJFNo ratings yet
- 10 - Metabolic SyndromeDocument12 pages10 - Metabolic SyndromeLuisErnestoRodriguezMNo ratings yet
- Association Between Baseline LDL-C Level and TotalDocument14 pagesAssociation Between Baseline LDL-C Level and TotalMr. LNo ratings yet
- New England Journal Medicine: The ofDocument15 pagesNew England Journal Medicine: The ofFerry Fawzi AnnorNo ratings yet
- Mechanisms, Clinical Implications, and Treatment of Intradialytic HypotensionDocument7 pagesMechanisms, Clinical Implications, and Treatment of Intradialytic Hypotensionhemer hadyn calderon alvitesNo ratings yet
- Cho Paradigm For Reduction of ASCVDDocument17 pagesCho Paradigm For Reduction of ASCVDBubu ToNo ratings yet
- Journal of Clinical & Translational EndocrinologyDocument7 pagesJournal of Clinical & Translational EndocrinologyArini NurlelaNo ratings yet
- 1 s2.0 S073510972207125X MainDocument12 pages1 s2.0 S073510972207125X MainAndreea RacovitaNo ratings yet
- Journal Pbio 3001561Document23 pagesJournal Pbio 3001561philosophy-thoughtNo ratings yet
- Povsic Et Al 2024 Effect of Reconstituted Human Apolipoprotein A I On Recurrent Ischemic Events in Survivors of Acute MiDocument12 pagesPovsic Et Al 2024 Effect of Reconstituted Human Apolipoprotein A I On Recurrent Ischemic Events in Survivors of Acute MiCHARLES BROSLONo ratings yet
- Jamacardiology Zhang 2021 Oi 210061 1630597090.4739Document8 pagesJamacardiology Zhang 2021 Oi 210061 1630597090.4739AlizaPinkyNo ratings yet
- Diabetic Cardiomyopathy: Editorial (See Bertoni ET AL., P. 2 7 9 1)Document3 pagesDiabetic Cardiomyopathy: Editorial (See Bertoni ET AL., P. 2 7 9 1)aymenNo ratings yet
- Epidemiology of Familial Hypercholesterolaemia CoDocument9 pagesEpidemiology of Familial Hypercholesterolaemia CoSusana RocheNo ratings yet
- Srikant H 2016Document10 pagesSrikant H 2016aditya sekarNo ratings yet
- 1 s2.0 S0085253817304180 MainDocument8 pages1 s2.0 S0085253817304180 MainBryan FarrelNo ratings yet
- Soluble Adhesion Molecules and Coronary Heart Dise - 3Document1 pageSoluble Adhesion Molecules and Coronary Heart Dise - 3Ramón Díaz-AlersiNo ratings yet
- New England Journal Medicine: The ofDocument12 pagesNew England Journal Medicine: The ofrevi fitraNo ratings yet
- Preventing Cardiovascular Disease in Patients With.2 PDFDocument3 pagesPreventing Cardiovascular Disease in Patients With.2 PDFbacharelado2010No ratings yet
- Evacetrapib y Resultados Cardiovasculares en La Enfermedad Vascular de Alto RiesgoDocument10 pagesEvacetrapib y Resultados Cardiovasculares en La Enfermedad Vascular de Alto RiesgoAlan Villegas SorianoNo ratings yet
- Hta TtoDocument13 pagesHta TtoAmelia RiveraNo ratings yet
- Expanding Roles of Vitamin D: Edward GiovannucciDocument3 pagesExpanding Roles of Vitamin D: Edward GiovannucciAgafioNo ratings yet
- Association Between Serum Lipids and Survival in Hemodialysis Patients and Impact of RaceDocument11 pagesAssociation Between Serum Lipids and Survival in Hemodialysis Patients and Impact of RaceJuanCarlosGonzalezNo ratings yet
- Translating Molecular Discovery Into New Therapies For AtherosclerosisDocument11 pagesTranslating Molecular Discovery Into New Therapies For AtherosclerosisDzikrul Haq KarimullahNo ratings yet
- Pathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCDocument42 pagesPathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCCalvin LitraNo ratings yet
- Therapeutic LipidologyFrom EverandTherapeutic LipidologyMichael H. DavidsonNo ratings yet
- The Journal of Physiology - 2023 - Watkins - Myo Inositol Alters The Effects of Glucose Leptin and Insulin On PlacentalDocument19 pagesThe Journal of Physiology - 2023 - Watkins - Myo Inositol Alters The Effects of Glucose Leptin and Insulin On PlacentalMario CoelhoNo ratings yet
- J American Geriatrics Society - 2014 - Atkins - Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality ADocument8 pagesJ American Geriatrics Society - 2014 - Atkins - Sarcopenic Obesity and Risk of Cardiovascular Disease and Mortality AMario CoelhoNo ratings yet
- Evaluation of Anti-Aging Effects of Gemfibrozil OnDocument6 pagesEvaluation of Anti-Aging Effects of Gemfibrozil OnMario CoelhoNo ratings yet
- Antioxidants 13 00385Document19 pagesAntioxidants 13 00385Mario CoelhoNo ratings yet
- Lvac 001Document9 pagesLvac 001Mario CoelhoNo ratings yet
- Vitd th17Document10 pagesVitd th17Mario CoelhoNo ratings yet
- Fnut 09 929891Document11 pagesFnut 09 929891Mario CoelhoNo ratings yet
- A Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisDocument14 pagesA Pilot Study Assessing The Effect of Prolonged Administration of High Daily Doses of Vitamin D On The Clinical Course of Vitiligo and PsoriasisMario CoelhoNo ratings yet
- Vit d3Document5 pagesVit d3Mario CoelhoNo ratings yet
- Safety of 5000 International Units Daily Oral Dosing of Vitamin d3 For Four Years in Various Diseases 5f28c908f2e62Document8 pagesSafety of 5000 International Units Daily Oral Dosing of Vitamin d3 For Four Years in Various Diseases 5f28c908f2e62Mario CoelhoNo ratings yet
- UNDocument419 pagesUNSiti Masruroh ArohNo ratings yet
- Unit 3 Prepare and Interpret Technical DrawingDocument20 pagesUnit 3 Prepare and Interpret Technical Drawingtracert_atanNo ratings yet
- PPC DrainDocument6 pagesPPC Drainherysyam1980No ratings yet
- Franchise PackageDocument3 pagesFranchise PackageJayson Nonan100% (1)
- Module 5Document27 pagesModule 5Labour lawNo ratings yet
- Final Seats Matrix Ss Counelling - 2022 D.M M.CHDocument55 pagesFinal Seats Matrix Ss Counelling - 2022 D.M M.CHMinerva Medical Treatment Pvt LtdNo ratings yet
- Sales Rebates ProcessingDocument1 pageSales Rebates ProcessingNavjyot SinghviNo ratings yet
- Final Project ML Nikita Chaturvedi 03.10.2021 Text AnalyticsDocument32 pagesFinal Project ML Nikita Chaturvedi 03.10.2021 Text AnalyticsNikita ChaturvediNo ratings yet
- Topic 1 - Whole NumbersDocument38 pagesTopic 1 - Whole Numbersnazri100% (3)
- Shape Memory Alloy Rotary Actuator For Cubesat Deployable StructuresDocument82 pagesShape Memory Alloy Rotary Actuator For Cubesat Deployable StructuresFernando Jesús Medina RodríguezNo ratings yet
- Working Capital Management With Reference To Thirumala Milk Products PVT - LTDDocument103 pagesWorking Capital Management With Reference To Thirumala Milk Products PVT - LTDsaryumba5538No ratings yet
- Φουρνος- convotherm - 4Document120 pagesΦουρνος- convotherm - 4Dimitris ThanasopoulosNo ratings yet
- ARA DraftProgWEBSITE1MayDocument13 pagesARA DraftProgWEBSITE1MayHNNo ratings yet
- CWTS 2 Community Service Proposal 2019Document5 pagesCWTS 2 Community Service Proposal 2019Paul BandolaNo ratings yet
- Insulated Flooring StanvacDocument7 pagesInsulated Flooring StanvacRamesh RoyNo ratings yet
- DLP IN ORAL COMMUNICATION-GRADE 11-EditedDocument6 pagesDLP IN ORAL COMMUNICATION-GRADE 11-EditedMaeann MirandoNo ratings yet
- تقرير الانجليزيDocument2 pagesتقرير الانجليزيbasel.khashashneh.44No ratings yet
- Tally Assignment 12Document90 pagesTally Assignment 12Kaushal SharmaNo ratings yet
- Acknowledgement (Draft 2) : IntroductionDocument3 pagesAcknowledgement (Draft 2) : IntroductionSHAIK AASHIQUE RASOOL ARCH-UG- 2018 BATCHNo ratings yet
- IJSARTV6I738053Document3 pagesIJSARTV6I738053VISHAL BHOJWANINo ratings yet
- FD Schedule & QBDocument6 pagesFD Schedule & QBDrDhananjhay GangineniNo ratings yet
- Buisness Plan OutlineDocument10 pagesBuisness Plan OutlinevangheliexNo ratings yet
- PCE Nautilus en 20130318Document2 pagesPCE Nautilus en 20130318Iker BasqueAdventureNo ratings yet
- BCS RulesDocument40 pagesBCS RulesHKF1971No ratings yet
- Butterfly CircusDocument2 pagesButterfly CircusSalma BenjellounNo ratings yet
- Install LogDocument36 pagesInstall Logfrans parulianNo ratings yet